
Abstract
Abstract
Severe aorto-iliac occlusive disease can cause disabling symptoms. The treatment of aorto-iliac occlusive disease has dramatically changed with the introduction of endoluminal techniques. However, according to the Trans-Atlantic Inter-Society Consensus for severe aorto-iliac disease, aorto-bifemoral bypass remains the therapy of choice. A recent addition to the open repair is laparoscopic-assisted aorto-bifemoral bypass, especially in occlusive arterial disease. In this article, we describe a new technique of performing gasless laparoscopic-assisted aorto-bifemoral bypass grafting with a self-designed abdominal wall-lifting system. We dealt with a patient who had a history of coronary artery disease and poor cardiopulmonary functional reserve. He had disabling symptoms of claudication and rest pain on bilateral lower extremities. Aorto-biliac-femoral occlusive disease was diagnosed in him, and he underwent the gasless laparoscopic-assisted aorto-bifemoral bypass. The total procedure time was 260 minutes. The patient was extubated 5 hours postoperatively. He was discharged home without complications 5 days after the surgery. This procedure is attractive not only to minimize the length of the wound and the time to extubation but also to avoid the possible lethal complications associated with the traditional laparascopic pneumoperitoneum. This device and technique can also provide a bridge for young or less-experienced surgeons to be familiar with total laparoscopic aortic surgery from traditional open repair.
Introduction
Case Report
The patient was a 69-year-old male smoker with a history of atrial fibrillation, gastric cancer, coronary artery disease, status post subtotal gastrectomy, and percutaneous coronary angioplasty. He had progressive worsening symptoms of claudication and rest pain after failed exercise training and optimal medical treatment. At this present admission, reconstructive computational tomography angiography showed total occlusion of bilateral common and external iliac arteries, left external iliac, left superficial femoral artery, and aneurysm formation of left internal iliac artery (Fig. 1). Taking into account his comorbidities and long-term outcome of the disease nature, gasless laparoscopic aorto-bifemoral bypass using self-designed abdominal lifting systems was planned.

(
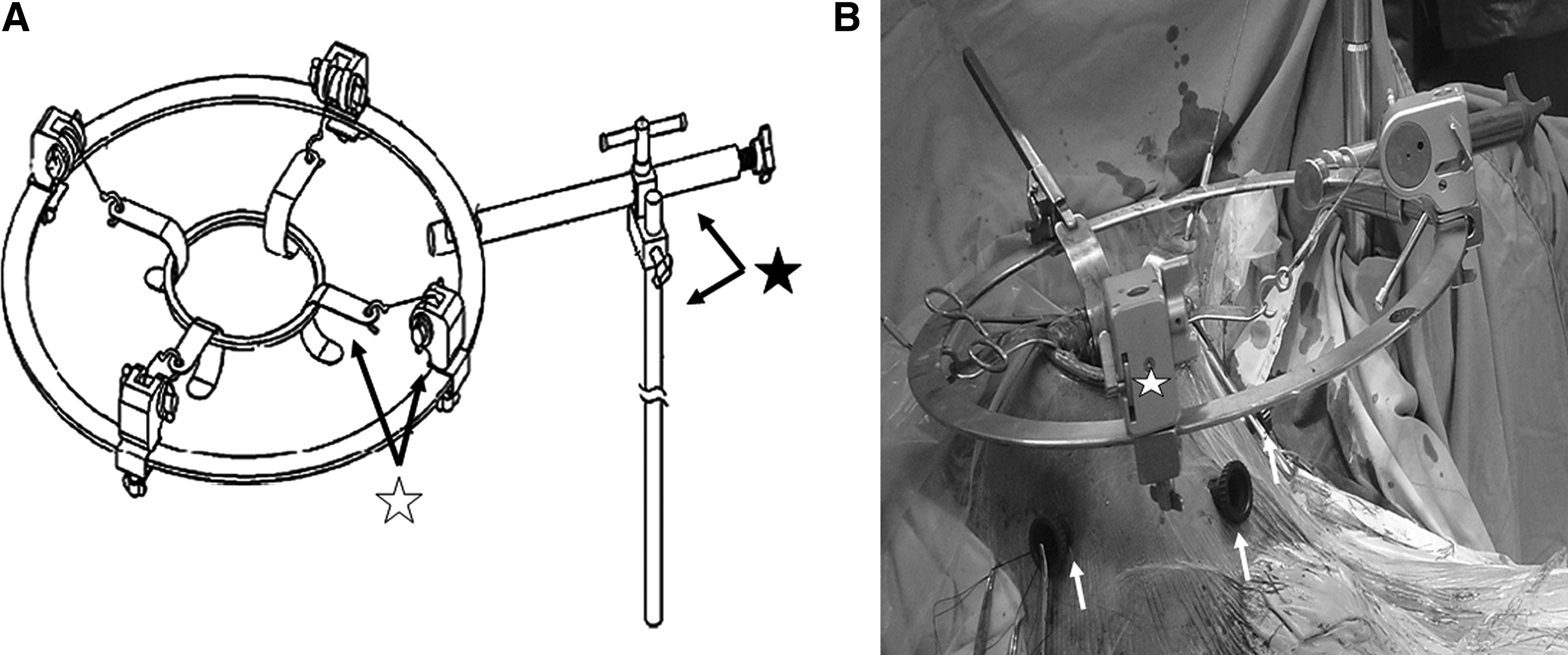
This patient was positioned in the supine position under general anesthesia. The operator stood on the right side of the patient, whereas the assistant stood on the left side. An 8-cm minilaparotomy was made in the midline of abdomen 3 cm above and 5 cm below the umbilicus. A wound protector was positioned over the minilaparotomy. The abdominal wall was then elevated by specially designed self-retaining retractors (Fig. 2A). Three trocard ports were created at the bilateral lower quadrant region and suprapubic area (Fig. 2B). A laparoscope was inserted either through the minilaparotomy or through any of the ports for thorough viewing of the distal abdominal aorta. A three-dimensional vision was efficiently obtained by direct viewing through the minilaparotomy and the laparoscopic image simultaneously. The intestine loops, transverse colon, and stomach were retracted and circumferentially packed under the abdominal wall with the big gauze pad to facilitate dissecting the aortoiliac bifurcation by directly using electrocautery from the minilaparotomy wound. The approach to the abdominal aorta was the same as that performed through an open xiphopubic incision. After mobilizing the distal abdominal aorta, the patient was heparinized with 7500 units to keep the activated clotting time above 300 seconds. We used atraumatic aortic clamp to partially clamp the aorta and sewing a bifurcated abdominal aortic graft (16-8-8, Hemasheild; Boston Scientific, Natick, MA) to the distal abdominal aorta with the end-to-side fashion. The anastomotic suture was done with 3-0 prolene through either the minilaparotomy wound or trocard ports to facilitate the circumferential stitches under the aid of laparoscopy. Bilateral common femoral arteries were dissected free in the conventional way through two groin incisions. Transperitoneal tunnelings to bilateral groins were performed, and the graft limbs were pulled out. The right common femoral artery anastomosis and additional profundoplasty were done with the end-to-end fashion. The left distal femoral artery anastomosis with end-to-side fashion was then performed.
(
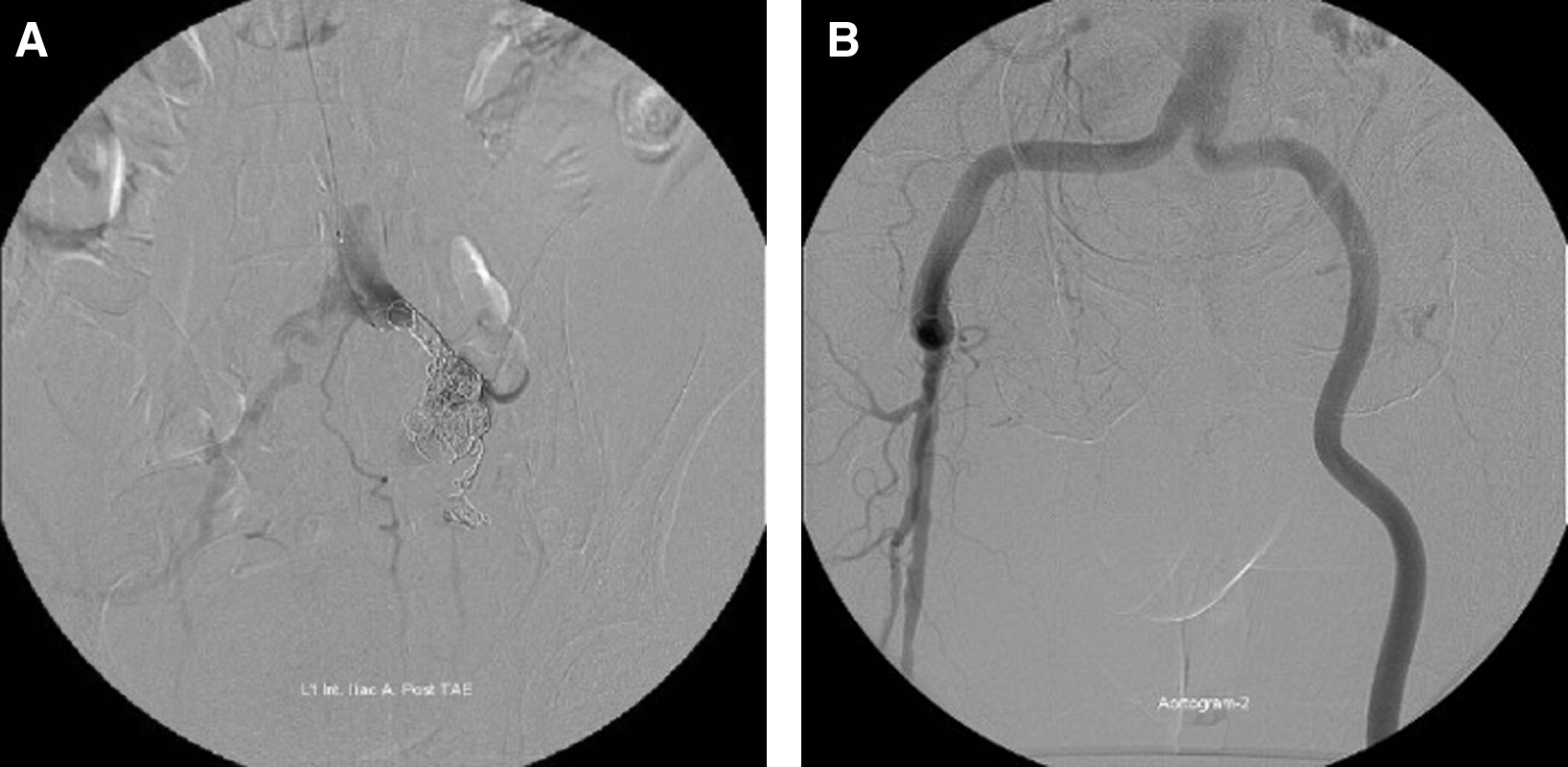
We placed two rubber tubes in a dependent area through the bilateral trocard ports and closed the abdominal wall in layers (Fig. 2C). The whole procedure time was 260 minutes. The aortic clamp time was 30 minutes, and the dissection of aorta took 32 minutes. No transfusion was necessary during the procedure. The patient was transferred to the intensive care unit and, subsequently, extubated in 5 hours. Peristalsis resumed in 20 hours after the surgery. Total intensive care unit stay was 1 day. Antegrade coil embolization of the internal iliac artery aneurysm from the left brachial artery was planned 3 days after the surgery (Fig. 3A), and the angiography showed patent aorto-bifemoral graft (Fig. 3B). The patient was discharged home 5 days after the surgery with an uncomplicated recovery. In 1 year follow up, this patient was symptom free and the vascular duplex showed patent aorto-bifemoral grafts.
(
Discussion
Surgical treatment is still the preferred treatment of recommendation for TASCII Type D aorto-iliac occlusive disease. Traditionally, this is treated with open surgical bypass grafting. Due to the high invasiveness of open repair, the TASC II also recently notes increasing interest in the laparoscopic approach. 11
Gasless laparoscopy-assisted abdominal surgery was introduced in general surgery to cope with the more complex laparoscopic procedures without jeopardizing the benefits of a minimal-access approach in our center since 2004. In the gas-filling total laparoscopic system, the creation of a pneumoperitoneum increased cardiac afterload and systemic vascular resistance, all of which might adversely affect the heart function in susceptible patients to a clinically significant degree.1,12 Moreover, difficulty in control of accidental massive bleeding and a steep learning curve were still major concerns in total laparoscopic aortic surgeries. Through the minilaparotomy made at the beginning of our procedure, the surgeon could perform dissection similar to traditional methods through direct vision. Direct control of the bleeding could be easily made, if needed, through the minilaparotomy; and vigorous suction could be accomplished through the ports or the minilaparotomy. The insertion of a hand inside the abdominal cavity restored tactile feedback to the operator and, thus, enabled the surgeon, by virtue of the restored tactile palpation and evaluation of the quality of the tissues (especially calcification of the arterial walls). 5 The aortic anastomosis could be easily performed through these three ports circumferentially with traditional instruments. In the transperitoneal approach to the abdominal aorta, the custom-made abdominal wall lift also played a primary role in retraction of the intestinal loops. It permitted a quick exposure of tissues, which was otherwise difficult to achieve by laparoscopic autostatic retraction systems.
Endovascular intervention was the treatment of choice for TASC type-A and B lesions but seldom tried in TASC C/TASC D lesions until recently. 11 In a review of these procedures, Karwowski and Zarins 2 concluded that the early results are promising, but the endografts need further evaluation before being accepted into routine use. In an uncontrolled study comparing 32 patients who had aortobifemoral bypass with 40 patients who underwent aortoiliac stenting, Hans et al. 1 concluded that both modalities gave satisfactory results. However, aorto-iliac stenting was associated with reduced primary patency at 48 months (69% ± 0.12% for aorto-iliac stenting and 93% ± 0.07% for aorto-bifemoral bypass).
Conclusion
The aim of laparoscopic vascular surgery in the aortoiliac segment is to replicate the excellent outcomes of open aortic surgery while providing the advantages of minimal invasive surgery. In this article, we reported 1 patient who was successfully treated by gasless laparoscopy-assisted aorto-bifemoral bypass with a newly developed retraction device. We found that few difficulties were encountered. This gasless procedure not only enjoyed the benefits of total laparoscopic surgery, including faster recovery, less postoperative pain, and fewer adverse cosmetic effects, but also preserved the advantages of open surgery, such as direct vision, tactile sensation, the use of traditional instruments, and prevented potential adverse effects of pneumoperitoneum from gas-filling laparoscopic surgery. Before introducing a total laparoscopic repair for aortoiliac occlusive disease, this gasless laparoscopy-assisted procedure can be a good intermediate candidate before surgeons can familiarize with total laparoscopic approach and should be considered as an option for aortic bypass when total laparoscopic repair is considered appropriate but not feasible.
Footnotes
Disclosure Statement
No competing financial interests exist.