
Abstract
Abstract
Objective:
The indications of various minimally invasive techniques for thyroidetomy are strictly limited to some selected patients; thus, only a minority of the patients can take advantages of them. In this study, we aim at describing a new technique of supraclavicular lateral collar incision for thyroidectomy and to verify the safety and efficacy of it as a beneficial supplement for minimally invasive approach and as a substitute for conventional transverse anterior approach, compared with which the lateral approach demonstrated a better cosmesis and comparative, extended indications.
Methods:
A prospective, nonrandomized analysis of consecutive thyroidectomies with different approaches was designed. From May 2006 to April 2009, 98 patients with lateral approach and 136 patients with conventional approach were analyzed to evaluate the eligibility of the new technique and its comparison with conventional approach for various clinical variables.
Results:
There were no statistical significances between the two groups in terms of age, gender, nodule size, anesthesia, estimated blood loss, operative time, and postoperative complications, whereas there were significant differences in terms of incision length (5.2 ± 1.04 cm versus 6.9 ± 1.14 cm, P < 0.001) and cosmetic result (8.7 ± 0.69 versus 6.7 ± 0.78, P < 0.001).
Conclusions:
The supraclavicular lateral collar incision is a feasible and safe approach for thyroidectomy. Compared with conventional approach, it holds the advantages of comparative extensive indications and similar complication rate but achieving a better cosmetic result. It provides a good alternative beyond conventional thyroidectomy, especially for those previously excluded from minimally invasive techniques.
Introduction
The aesthetic appearance of the incisional scar of the exposed neck area is important for women particularly, who constitute a large part of the patients who are affected by thyroid disease. Since 2006, we have been seeking and developed an innovative technique for performing thyroidetomy through a supraclavicular lateral collar incision, with which we have managed almost all of the cases that are indicated for conventional thyroidectomy, not only obtaining a better cosmesis but also gaining extended indications compared with the minimally invasive techniques. Our objective in the current study was to describe our new technique and to verify the safety and efficacy of it as a substitute for conventional thyroidectomy and as a probable supplement for minimally invasive techniques.
Materials and Methods
Patients selection and evaluation
From May 2006 to April 2009, 98 consecutive thyroidectomies via the supraclavicular lateral collar incision were performed in our department. A prospective nonrandomized study was designed to evaluate the eligibility of the new technique and its comparison with the conventional approach for different variables. The following patients were excluded from this study: (1) patients with thyroid malignancies that required a large scale neck dissection; (2) those who had previous thyroid surgery with conventional incision by other surgeons; and (3) patients who underwent endoscopic thyroidectomies. Otherwise, all benign and malignant diseases in spite of the nodule size or gland volume were included. Thus, another 136 thyroidectomies via the conventional approach performed at the same period were selected as a control group.
During the time of hospitalization, complete preoperative evaluations (biochemical assessment, laboratory thyroid function, ultrasonography, and computed tomography) were obtained and judged in all cases. Preoperative laryngoscope was performed to evaluate the vocal cord function if the patient had any symptoms of hoarseness that indicates the invasion of recurrent laryngeal nerve. Otherwise, the laryngoscope was not carried out as a routine. All the related data such as anesthesia, types of operation, length of incision, blood loss, operative time, final pathologic findings, postoperative complications and the demographic characteristics of the patients were collected and recorded into our database. All the patients gave informed consent for the procedure.
One month postoperatively, the cosmetic results were evaluated with a numerical score system ranging from 0 to 10. The patients at their follow-up were asked to score the degree of their satisfaction with the incision appearance. The scores were also recorded and evaluated into the database.
Surgical technique
Before being taken to the operating room, all the patients while sitting up were carefully marked for the incision location supraclavicularly and laterally to the neck along with the skin crease or under the shade of neck decorations such as a necklace. For bilaterally affected cases, the incision was designed on the dominantly enlarged side. Except for some bilateral large nodules or thyroid volume (with the diameter >6 cm), all the procedures were performed under cervical plexus blocking anesthesia and were necessarily converted to general anesthesia, at any time during the operation if there was complained intolerance of the operative manipulation by the patients.
The patient was placed in a supine position with a roll beneath the shoulders to slightly extend the neck. The incision was then made along the marker previously made with its medial end not exceeding the clavicular head of the sternomastoid muscle (Fig. 1A). The platysmal muscle was transected and subplatysmal flap was created as described in the conventional approach. Then, the cervical fascia was incised just along the anterior border of the sternocleidomastoid to expose the strap muscles, which were elevated and retracted bilaterally after blunt longitudinal division above the thyroid gland. Subsequently, the gland lobe was directly exposed just under the incision; this would facilitate the division and ligation of the middle vein, upper and lower vascular pedicles than usual (Fig. 1B–D). Next, the enlarged thyroid lobe and the isthmus were resected and removed. In our technique, the recurrent laryngeal nerve was not intentionally identified or traced as a routine, except for some complicated conditions that nerve injury was suspected (discussed below).
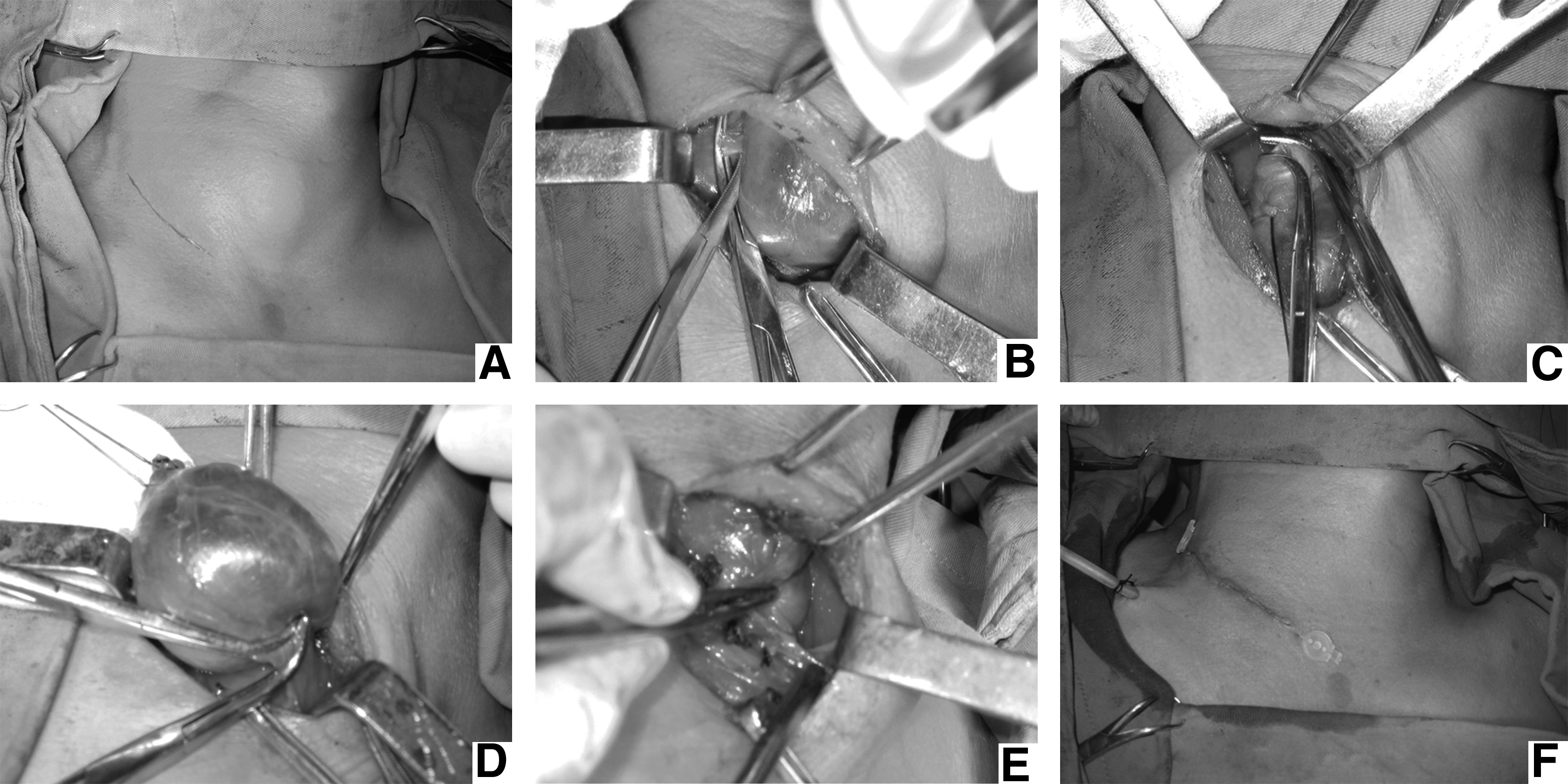
The resection of the dominantly enlarged lobe and the isthmus made it accessible to explore and resect the contralateral lobe if indicated. This technique commenced with further dissection contralaterally under the strap muscles (not platysmal muscle) beyond the trachea to establish a working space. Then by redirecting the retractions, the incision could be moved slightly around the neck to facilitate exposure for the counterpart lobe (Fig. 1E). As the remnant lobe was retracted medially, careful dissection and ligation of the upper pole, middle vein, and lower pole were performed, subsequently and respectively. Then, the specimen was removed likewise, and together with the previously resected part it was sent for frozen pathologic analysis. While awaiting the result that usually took about 30 minutes, the recurrent nerve was identified if indicated; any palpable lymph nodes were examined; careful inspection and haemostasis were pursued; and finally, sufficient irrigation was made before closure.
If the frozen pathologic findings revealed the presence of cancer, the incision could be lengthened along its medial end, if necessary, to the contralateral side of the neck, and an oncological surgical thyroidectomy was then further carried out with central compartment lymphadenectomy. A 12-gaged silicone tube was placed in the thyroid cavity, if indicated, through a small incision (5 mm) on the supraclavicular fossa (Fig. 1F). Then, the strap muscles and platysmal muscle were reapproximated; the incision was closed with subcutaneous monofilament to eliminate scar formation (Fig. 1F).
Statistical analysis
All the continuous variables were expressed as mean ± standard deviation. The statistical analysis was performed with the two-tailed student's t-test for normally distributive data. A nonparametric test (Mann–Whitney test) was performed when distribution was non-normal. All statistics were calculated using SPSS 15.0 for Windows (SPSS, Inc., Chicago, IL).
Results
In this study, a group of 98 patients with an average age of 47.2 years (range 9–73 year) underwent thyroidectomy by supraclavicular lateral collar incision; whereas another group of 136 patients with an average age of 45.5 years (range 19–78 year) underwent thyroidectomy by conventional transverse anterior incision. All the demographics of these patients are demonstrated in Table 1. There were no statistical significances between the two groups in terms of age, gender, and nodule size. The size of the nodule/thyroid was presented by the maximal diameter of the nodule or by the transverse diameter of the gland for multinodular goiters. The mean size of the nodule/thyroid was 3.9 ± 1.99 cm in the conventional group (range 1.0 to 10.0 cm) and 3.6 ± 1.88 cm in the lateral collar incision group (range 0.6 to 8.0 cm). Although there was no significant difference between the two groups regarding the nodule size, in our experience the largest nodule that could be treated by the lateral collar incision was limited to 8 cm unilaterally and 6 cm bilaterally (with one side lesion profoundly larger than another); all the other cases beyond the criteria were treated with the conventional approach.
Data expressed by mean ± standard deviation.
There were 14, 10, 4, and 2 of these patients that had concomitant nodular goiters, respectively.
In the lateral collar incision group, the procedures consisted of 9 subtotal lobectomies/nodulectomies, 34 lobectomies, 46 subtotal/near-total thyroidectomies, and 9 total thyroidectomies. In the conventional group, the number of cases was 11, 40, 71, and 18, respectively (Table 1). On the part of final pathologic findings, there were 30 patients in two groups who were deemed preoperatively to have multinodular goiters but finally revealed to have concomitant follicular adenomas and papillary cancers (see Table 1 annotations). There were also 7 cases in the conventional group and 3 cases in the lateral group who had concomitant thyroiditis but could be handled well by careful dissection against the adhesions of surrounding tissues.
All the intraoperative variables are shown in Table 2. There were no statistical significances between the two groups in terms of anesthesia, estimated blood loss, and operative time. A majority of the procedures could be accomplished under cervical plexus blocking anesthesia. The incision length was significantly different between the two groups; it was 5.2 ± 1.04 cm (range 3 to 8 cm) in the lateral collar incision group and 6.9 ± 1.14 cm (range 5 to 10 cm) in the conventional group (P < 0.001).
Data expressed by mean ± standard deviation.
Including time for frozen section, which took about 30 minutes.
The recurrent laryngeal nerve was not intentionally identified in all cases (discussed below); the exact data were not available for each group, and, therefore, statistical comparisons were not attempted. Nevertheless, there was only 1 patient in the lateral collar incision group and 2 patients in the conventional group who experienced temporary recurrent laryngeal nerve palsy and got cured within 1 month. There were no cases of permanent laryngeal nerve injury or hypoparathyroidism in each group. There were also no cases of wound hematoma, infection, or postoperative bleeding observed in our study. In terms of postoperative complications, there were no statistical differences between the two groups.
All the patients were asked 1 month after the operation to grade their satisfaction with the incision appearance by a numerical score system, ranging from 0 to 10. The cosmetic result was considered to be more satisfying to patients operated by lateral collar incision with a mean score of 8.7 ± 0.69, whereas the conventional group had a mean score of 6.7 ± 0.78 (P < 0.001). Figure 2 shows the picture of incisional appearance 1 month after the operation.

The appearance of the incision 1 month after the operation is demonstrated above. The right one shows that the incision can be hidden well by the necklace.
Discussion
In the last decade, various techniques for minimally invasive video-assisted/nonendoscpic thyroidectomy have been described.5–7 At the same time, plenty of studies concerning the comparison of these techniques with conventional techniques have been published with the evidence of beneficial outcomes.2–5 However, these procedures are exclusively indicated in strictly selected patients with small thyroid nodules (<35 mm) and thyroid volume (<25 mL), 9 which means only a minority of the patients can take advantages of these procedures, and the percentage has been reported to be 9.7% (n = 8580) by Miccoli et al. and 16% (n = 3165) by Lombardi et al., respectively.11,12 Since November 2005, we have attempted an innovative approach via supraclavicular lateral collar incision to access thyroidectomy, offering an alternative choice for the patients excluded from the criteria of minimally invasive procedures, and the new approach demonstrated a good result.
The new technique was initially designed to treat unilaterally affected thyroid disease to achieve a good cosmetic effect. As our experience accumulated, we found that it is feasible to explore and resect the contralateral lobe by dissecting the lose connective tissue between the strap muscles and the thyroid surgical fascia under most circumstances. Thanks to the flabbiness of the cervical skin, the incision can be slightly moved around the neck toward the other side, and with the redirection of the retractor, a resection of the contralateral thyroid lobe could be carried out. So, we extended the indications of this technique to bilaterally affected thyroid disease, especially for those in whom one side of the gland (<6 cm) was dominantly larger than the other (<3 cm). The incision was designed on the dominantly affected side, after removal of the larger lobe and isthmus; the accessibility to the contralateral part was feasible and safe. By now, we conceive the indications for this new technique to be as follows:
All benign thyroid disease indicated for the conventional approach except for the bilaterally enlarged gland such as both size >6 cm. For the cases that one lobe of the thyroid is <6 cm with or without the other lobe <3 cm, it is an optimal indication. Low-grade malignancies with the nodule size <3 cm that do not require large scale lymphatic dissection. History of thyroiditis and irradiation are not exclusion criteria.
Recurrent laryngeal nerve is an important tissue that should be carefully protected during neck surgery. In our studies, except for some complicated cases or total thyroidectomy, we did not intentionally dissect the recurrent laryngeal nerve as a routine. 13 The reasons are as follows: First of all, we mostly do subtotal/near-total thyroidectomies that leave a small remnant of thyroid tissue on the back in which the nerve lies and runs, which means the nerve can be left intact and protected 14 ; second, we believe that with increased experience and familiarization of the neck anatomy, the surgeons can avoid unnecessary injury to the recurrent nerve with careful resection; third, we hold our opinion that the manipulation of finding the nerve itself can raise the risk of nerve injury. The incidence of nerve palsy in our study of all the 172 operations was consistent with the previous report. 15 There were 1 and 2 cases in each group that developed postoperative nerve palsy represented by hoarseness, all of which were transient and cured within 1 month. There was no permanent recurrent nerve injury occurred in all cases. At the same time, the parathyroid gland could be saved and protected in a similar fashion, and in all cases of this study, there was no postoperative hypoparathyroidism observed either.
Compared with the conventional approach, the new technique revealed a significantly better cosmetic result with a numerical score of 8.7 ± 0.69 versus 6.7 ± 0.78 (P < 0.001). This pleasing cosmesis is, of course, substantially due to a smaller incision employed. It is notable that in a further analysis, we found up to 70.4% of the procedures could be accomplished through a small incision no >5 cm by lateral collar incision, whereas the peak value of the incision length was 7 cm for 77.2% cases by conventional approach (Fig. 3). Besides a smaller incision, we insist that some other factors also contribute to an optimal cosmesis. In one way, we marked all the incisions before the operation while the patients were sitting up; this could make the incision in a natural skin crease position and hidden behind the neck decoration or shirt-collar. 16 In another, during the operation, ligation of the anterior jugular vein and transversal resection of strap muscles could be avoided in most cases, thereby preventing the postoperative disturbance of venous return and subplatysmal scar formation. Also, the use of monofilament and careful approximation of the skin edges also minimized the chances of incisional scar formation.
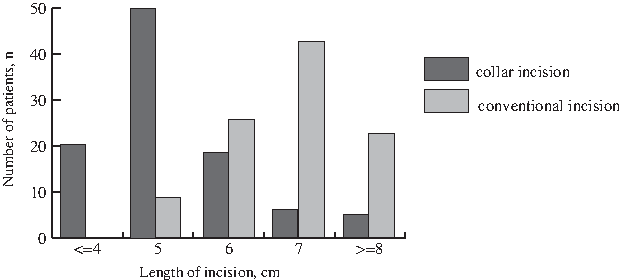
Distribution differences in incision length between the 2 groups are demonstrated. The differences were statistically significant (P < 0.001). Up to 70.4% of the procedures can be performed through an incision no >5 cm by the lateral approach.
The applications of various minimally invasive approaches for thyroid malignant diseases are still controversial since their emergences. 10 Great fear is concerned about the oncological radicality of the procedures confined to their limited operative space, such as central compartment lymphadenectomy, cancer cells deposit, and metastasis. However, the new technique is obviously exempt from such suspicions and achieves a comparable outcome with the standard conventional technique. If needed according to the operation decision, the incision could be extended to an L-shaped curve, thus maintaining a good operative manipulation vision.
Considering its feasibility and cosmesis, we propose this new approach as a substitute for conventional approach thyroidectomy and as a potent supplement to minimally invasive techniques. Here in our department, the surgical strategy for thyroid surgery falls into a proportion approximately such as 10% with minimally invasive techniques, 80% with collar incision approach, and the final 10% applying for conventional approach.
Moreover, this technique can be easily carried out by most of the surgeons who have traditional thyroidectomy experience with a very short learning curve. It requires no more special equipment or surgical instruments (such as endoscope and disposable ultrasonic scalpel), thus saving a large amount of medical expenditure especially for the developing countries.
Conclusions
The results of this study indicate that the supraclavicular lateral collar incision is a feasible and safe approach for thyroidectomy. Compared with the conventional approach, it holds the advantages of comparative extensive indications but a better cosmetic result. At this point, the new approach provides a good alternative beyond conventional thyroidectomy, achieving a balance between the existence of the conventional approach and comesis requirements of patients excluded from minimally invasive techniques.
Footnotes
Disclosure Statement
There is no special financial support or funding for this study from other authors or institutions. There is no conflict of interest with other authors or entities concerning this study. We have no personal or financial disclosures to reveal associated with this presentation.