
Abstract
Dear Editor:
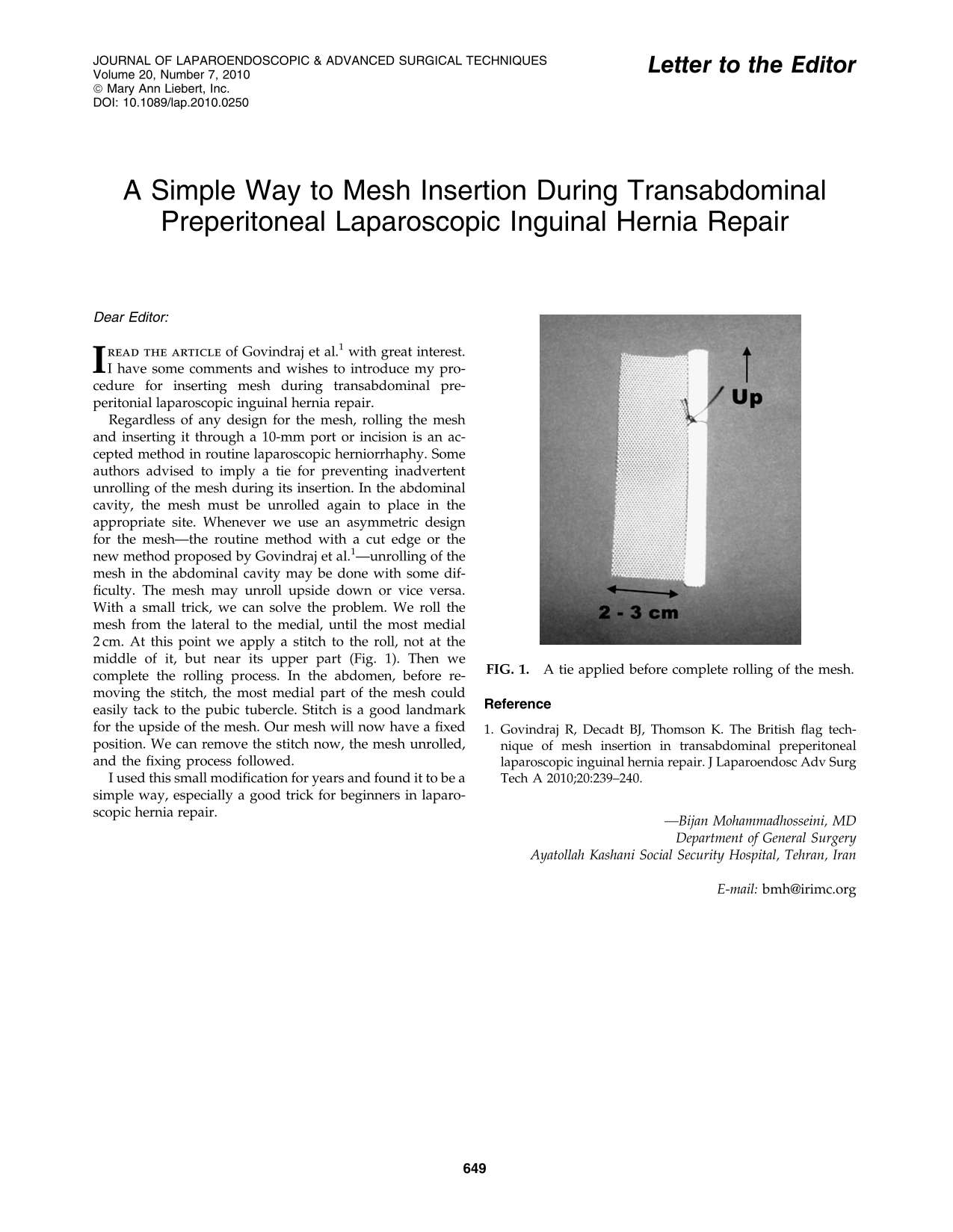
Regardless of any design for the mesh, rolling the mesh and inserting it through a 10-mm port or incision is an accepted method in routine laparoscopic herniorrhaphy. Some authors advised to imply a tie for preventing inadvertent unrolling of the mesh during its insertion. In the abdominal cavity, the mesh must be unrolled again to place in the appropriate site. Whenever we use an asymmetric design for the mesh—the routine method with a cut edge or the new method proposed by Govindraj et al. 1 —unrolling of the mesh in the abdominal cavity may be done with some difficulty. The mesh may unroll upside down or vice versa. With a small trick, we can solve the problem. We roll the mesh from the lateral to the medial, until the most medial 2 cm. At this point we apply a stitch to the roll, not at the middle of it, but near its upper part (Fig. 1). Then we complete the rolling process. In the abdomen, before removing the stitch, the most medial part of the mesh could easily tack to the pubic tubercle. Stitch is a good landmark for the upside of the mesh. Our mesh will now have a fixed position. We can remove the stitch now, the mesh unrolled, and the fixing process followed.

A tie applied before complete rolling of the mesh.
I used this small modification for years and found it to be a simple way, especially a good trick for beginners in laparoscopic hernia repair.