
Abstract
Abstract
Introduction:
Gasless laparoscopy-assisted surgery has been utilized in many abdominal diseases, and it has been proved to be effective and efficient compared with conventional open surgery. The study was conducted to evaluate the efficacy of gasless laparoscopy-assisted surgery in management of intraabdominal/retroperitoneal tumor of unknown origin.
Methods:
From June 2004 to April 2009, nine patients who underwent gasless laparoscopy-assisted surgery for intraabdominal/retroperitoneal tumor of unknown origin were recruited. Intraabdominal/retroperitoneal tumor of unknown origin was defined as (1) diagnosis of enlarged retroperitoneal lymph node; (2) evaluation of peritoneal or mesenteric lesion, or tumor of nondigestive systems; and (3) staging of intraabdominal malignancy.
Results:
Four patients underwent gasless laparoscopy-assisted surgery for retroperitoneal enlarged lymph nodes, four for evaluation of intraabdominal lesion, and two for staging of the malignancy. Sufficient tissue was obtained from all patients, and the diagnosis was as follows: three lymphomas, three peritoneal carcinomatoses, two chronic imflammations, and one benign tumor.
Conclusions:
Three purposes can be achieved: a familiar method for the surgeon compared with total laparoscopic surgery, easy accessibility for further oncological management, and intraoperative miniconversion for peritoneal examination. It is a safe and effective way to obtain tissue for pathology and feasible in case of necessary sequential tumor resection.
Introduction
Materials and Methods
From June 2004 to April 2009, patients' charts were reviewed retrospectively in our hospital. Definition of intraabdominal or retroperitoneal tumor of unknown origin was categorized as follows: (1) diagnosis of enlarged retroperitoneal lymph node; (2) evaluation of peritoneal or mesenteric lesion, or tumor of nondigestive systems, which was incidentally found either by imaging or during operation; and (3) staging of intraabdominal malignancy. During the period, a total of nine patients underwent gasless laparoscopy-assisted surgery for abdominal tumor of unknown origin and were included in the study. The demography including age, sex, underlying diseases, initial presentation, preoperative diagnosis, and indication for surgery was recorded. The preoperative radiologic parameters including preoperative image diagnosis, computed tomography (CT)/ultrasonographic findings, and biopsy pathology were also reviewed. The conversion of the laparoscopic surgery, intraoperative findings, and complications were collected in this study.
Operation method
A 3 cm midline minilaparotomy was made, and the wound was covered with wound protector. The abdominal wall was lifted by our designed self-retaining retractors and wall-lifting system (Fig. 1). One subumbilical and two subcostal ports were sequentially created. Through the subumbilical port, a laparoscope was used to inspect the peritoneal cavity. The sampling of the intraabdominal/retroperitoneal tumor could be performed by traditional or laparoscopic electrocautery. If the tumor was located deeply between the lethal organs of great vessels, then the other two to three trocars would be inserted. The laparoscope, traditional and laparoscopic instruments can be inserted through either the minilaparotomy wound or the trocars. The specimen will be retrieved from the minilaparotomy.
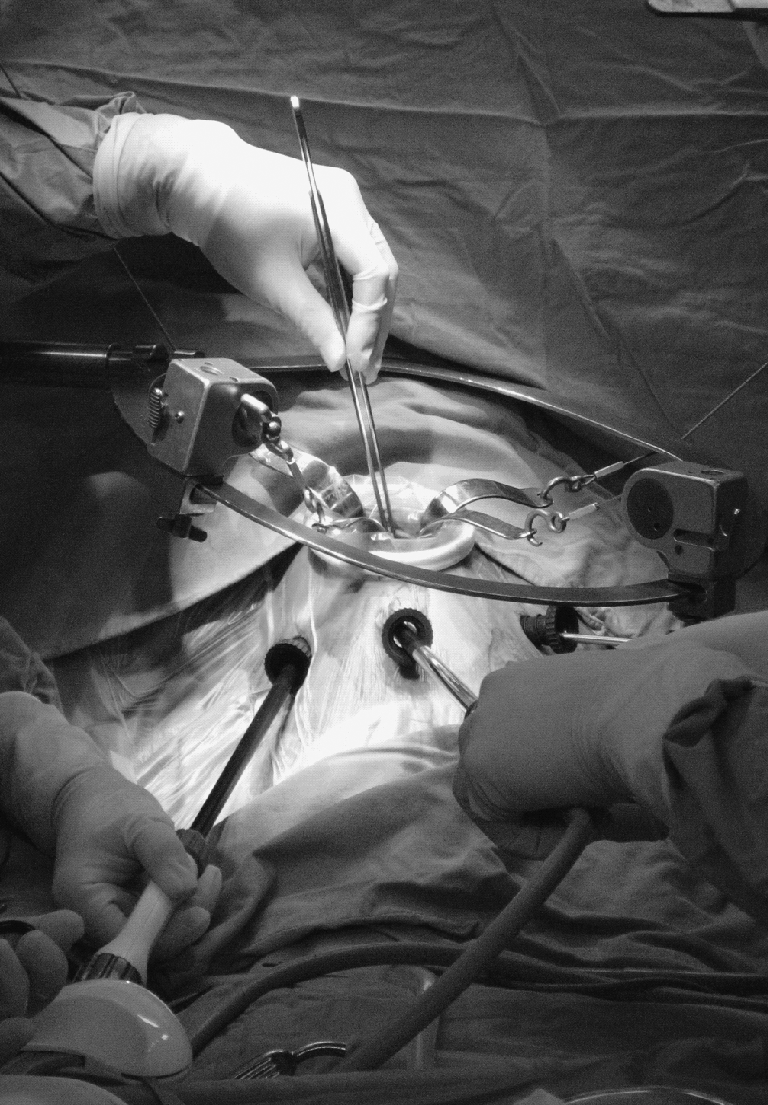
Gasless laparoscopy-assisted setting.
Results
A total of nine gasless laparoscopy-assisted surgeries for intraabdominal/retroperitoneal tumor of unknown origin were performed, including five men and four women. The median age was 64.8 years (range 47–80 years). The mean body mass index was 21.4. The underlying diseases, clinical presentation, and tumor location on CT of the patients were recorded (Table 1). The indication of surgery for each patient is shown in Table 2: Four patients underwent gasless laparoscopy-assisted surgery for diagnosis of retroperitoneal enlarged lymph nodes (case 3, 5, 7, 9), four patients for evaluation of intraabdominal lesion (case 1, 2, 5, 8), and two for staging of the malignancy (case 4, 6). Case 5 was found to have cervical mass and enlarged retroperitoneal lymph nodes on CT and met the indication one and two concomitantly. Preoperative CT was performed and demonstrated positive in all patients except case 8, for whom the peritoneal lesion was incidentally found intraoperatively (Fig. 2).

The computed tomography of the cases (except case 8) was demonstrated (red arrow).
BMI, body mass index; CT, computed tomography.
Surgical results
Among cases 1 to 3, lymphoma was diagnosed postoperatively. In case 1, intraoperative frozen biopsy revealed lymphoma and excisional biopsy was performed. In case 2, small bowel tumor was resected and jejunojejunal anastomosis was done by means of the gasless laparoscopy-assisted method with total intracorporeal anastomosis. In case 3, intraoperative frozen biopsy revealed no evidence of malignant lymphoma, and single enlarged lymph node was resected.
Among cases 4 to 6, peritoneal carcinomatosis was diagnosed intraoperatively. In cases 4 and 5, tumor biopsy was performed for final tissue proof. For case 6, gas-filling diagnostic laparoscopy was initially employed and miniconversion was consequently done for a jejunostomy after confirmation of peritoneal seeding.
In case 7, the pancreatic head was checked and a firm nodule was incidentally found. For case 8, minilaparotomy was initiated to remove the dialysis tube, and multiple elastic nodules were noticed overlying the omentum. Consequently, the gasless laparoscopy-assisted setting was employed for facilitating further peritoneal examination. In case 9, the mesenteric tumor was totally excised, and biopsy around surrounding tissue was performed (Table 3). For all nine patients, intraoperative hemostasis was achieved without requirement of transfusion.
LAP, lymphadenopathy; LN, lymph node; NTM, nontuberculosis mycobacterium.
Pathological diagnosis and outcomes
Among cases 1 to 3, sequential chemotherapy was arranged after confirming the diagnosis of lymphoma. In case 2, the patient expired due to multiple organ failure 4 months after the operation. For cases 4 to 6, peritoneal carcinomatosis was diagnosed intraoperatively. In case 4, the patient had a history of gastric cancer with abdominal wall metastasis, and metastatic gastric cancer with peritoneal carcinomatosis was diagnosed. In case 5, the patient received Tarceva (Erlotinib®) therapy after the confirmation of lung cancer with peritoneal carcinomatosis. In case 6, the patient expired due to gastric cancer-related multiple organ failure 4 months after the operation. In case 7, biopsy revealed nontuberculosis mycobacterium-related supurative granumatous inflammation. Pancreatic leakage occurred after operation, and the patient recovered after antibiotics treatment. Anti-tuberculosis therapy was soon initialized after recovery. In case 8, omentum nodule was checked as acute and chronic inflammation, and fibrosis peritonitis was diagnosed. The patient underwent arteriovenous shunt creation and received temporary hemodialysis through double lumen catheter. In case 9, the pathology revealed benign mesenteric cysts, and the patient was followed up without any disease evidence (Table 3). The disease distribution is shown in Table 4.
Discussion
Histopathologic biopsy is necessary for definite diagnosis and further management of intraabdominal/retroperitoneal tumor of unknown origin. Percutaneous ultrasonography/CT-guided biopsy is thought to be the first line of method if the tumor is adjacent to the abdominal wall or easily approachable.1,2 Although conventional laparotomy for tissue proof is the standard method for intraabdominal/retroperitoneal tumor of unknown origin, once the tumor is unapproachable by percutaneous image-guided biopsy, laparoscopic biopsy has been reported effective and efficient to obtain sufficient tissue for histopathology. 3 With a minimally invasive nature, laparoscopic surgery has been shown to be less painful and to provide better recovery compared with the conventional open method.4–6
Some disadvantages have been reported to be associated with totally gas-filling laparoscopic surgery. The concern regarding the use of pneumoperitoneum remains. The creation of pneumoperitoneum compromises cardiovascular function and renal function in the elders.7–9 The tumor growth at the peritoneum was promoted under the insufflation of carbon dioxide, which increased greater abdominal wall metastases. 10 Second, massive bleeding was uncontrollable due to lack of adequate suction, and difficulty in hemostasis under the circumstance of pneumoperitoneum became the leading cause of conversion to conventional open surgery. 11 Port-site metastasis was reported in patients who underwent gas-filling laparoscopic surgery in certain oncological resections of malignancy.12,13 Although the mechanism was not detailed, the chimney effect was claimed to be the most important factor. 14 Besides, it demanded time for a surgeon to overcome the learning curve of pure gas-filling laparoscopic surgery.15,16 Laparotomy for oncological resection of the tumor became inevitable after the totally laparoscopic biopsy if the tumor was located at a lethal organ or a gastrointestinal anastomosis was necessary.
We designed the gasless laparoscopy-assisted method initially to be used in early gastric cancer, which was proved to be safe and feasible. 17 The gasless laparoscopic setting was applied for many abdominal surgeries, and further several procedures were developed. 18 By the creation of minilaparotomy, a direct vision is present and a surgeon can employ the laparoscopic surgery in a familiar way with either direct vision or scopic view. Additionally, the traditional and laparoscopic instruments can be used concomitantly. Wall-lifting space without pneumoperitoneum enables vigorous suction, which minimizes the potential conversion while being confronted with uncontrollable bleeding.
Three purposes are achieved by means of gasless laparoscopy-assisted biopsy for intraabdominal/retroperitoneal tumor. First, with the abdominal wall-lifting setting, a familiar way can be obtained by the direct vision through the minilaparotomy. The conventional instruments can be applied with laparoscopic instruments concomitantly. Second, once the tumor has been proved to be malignant and a further surgical resection is indicated, the gasless laparoscopy-assisted surgery is suitable as a miniconversion. Successful applications of gasless laparoscopy-assisted surgery have been reported in gastric surgery, hepatobiliary surgery, and small bowel surgery.17,18 The minilaparotomy could be regarded as a miniconversion of pure laparoscopic surgery for easily bleeding tumors or potentially high possibility of further en bloc resection. The miniconversion enables further tumor excision and gastrointestinal anastomosis without performing conventional laparotomy. 19 Once surgical resection of the tumor is mandatory, the gasless laparoscopy-assisted surgery is an alternative choice in performing the operation. Third, as in our series, an intraoperatively, incidentally found tumor is manageable by the aid of the abdominal wall-lifting setting. With the aid of the abdominal wall-lifting setting, a combination of laparoscopy and minilaparotomy could serve as a tool instead of conversion to conventional open surgery and prevention from wound extension. The hybridized nature of gasless laparoscopy-assisted surgery makes it flexible and could be seen as a bridge between whole gas-filling laparoscopic surgery and traditional surgery.
Some limitations might exist on the gasless laparoscopy-assisted method. Encountering an obese patient, the abdominal wall is difficult to lift due to the relative thickening of adipose layers. Compared with the gasless laparoscopy-assisted setting, the conventional pneumoperitoneum created a better operative working space in the circumstances. Besides, the abdominal wall-lifting setting inevitably restricted the extension of the operative field and working space over the bilateral sides of the abdomen, which may, although not shown in our cases, influence the sampling of small nodules located at the lateral abdomen. Lateral field expansion will be improved in our next generation gasless setting.
In our series, all nine patients underwent gasless laparoscopy-assisted method for abdominal tumor of unknown origin, which was found either preoperatively or intraoperatively. The sequential diagnosis were lymphoma, peritoneal carcinomatosis, chronic inflammation (one nontuberculosis mycobacterium [NTM] and one fibrous peritonitis), and benign tumor. All patients received adequate management after the confirmation of the diagnosis and experienced an uneventful hospital course except one patient, who had intraabdominal infection and recovered after antibiotics treatment. The whole complication rate was 11% and was higher than that reported in literatures, 20 which might be related to the small number of patients recruited in the studies.
Conclusion
We concluded that minimally invasive gasless surgery offers an alternative way to perform biopsy when encountering an abdominal tumor. Our minimally invasive gasless laparoscopy-assisted surgery combined the benefits between open and pure gas-filling laparoscopic surgery. It is safe and effective to obtain tissue for pathology and feasible in sequential tumor resection.
Footnotes
Disclosure Statement
No competing financial interests exist.