
Abstract
Abstract
Laparoscopic cholecystectomy (LC) is one of the most commonly performed operations, yet the frequency of bile duct injury remains unacceptably high, and up to 25% of urgent LCs are converted to the open approach. Intraoperative laparoscopic biliary ultrasonography (IOUS) allows identification of portal structures before division of any structure, but the impact of IOUS on LC for acute biliary disease has not been clearly reported. A retrospective review was conducted of all patients who underwent cholecystectomy over a 29-month period. IOUS was performed after release of the medial and lateral peritoneal attachments of the gallbladder. Of the 65 patients, 43 (66%) had an urgent operation. Mean operative time was 89.6 minutes (range 45 to 196 minutes). IOUS was used routinely, when available, in 50 patients (77%). The biliary anatomy was completely observed in 48 patients (96%). IOUS identified significant biliary abnormalities in 20 patients (40%) including presence of a foreshortened cystic duct (CD) (<1 cm) in 7 patients (14%), common bile duct stones in 4 patients (8%), abnormal CD anatomy in 4 patients (8%), and abnormal vascular anatomy in 8 patients (16%). No patient was converted to open operation, no bile duct injury occurred, and no patient required subsequent biliary intervention. IOUS is effective at observing biliary anatomy in the setting of acute disease, and may be a useful tool during these difficult cases.
Introduction
An anonymous survey of American surgeons concluded that the “learning curve” plays a role in BDI. Early in practice, surgeons trained in LC during residency had fewer BDI than surgeons who learned the technique after residency training. However, after completing 200 LCs, BDI occurred at similar rates between the two groups, and persisted despite increasing experience. 3 It remains a general consensus among surgeons that BDI is largely caused by abnormal cystic duct (CD) anatomy and/or inflammation, and is an inevitable consequence of LC. 4 The “critical view” technique, if used to definitively identify the CD before division, minimizes the risk of BDI. 5 However, in cases of acute cholecystitis, impacted gallstones causing CD obstruction, or dense inflammatory adhesions in the Triangle of Calot, establishment of the critical view may be unobtainable. This may explain why 25% of inpatient cholecystectomies were still performed by the open approach as of 2000. 1
Routine intraoperative cholangiogram (IOC) has been described as a means to decrease the frequency and severity of BDI. It is estimated that only 11% of American hospitals perform routine IOC because of added cost and surgeon inconvenience. 6 Alternatively, several studies have attested to the safety, efficacy, and cost-effectiveness of routine intraoperative laparoscopic biliary ultrasonography (IOUS) in identifying portal structures and detecting common bile duct (CBD) stones, yet this technique remains underutilized. There are few reports on the specific findings of IOUS. A recent report suggests that IOUS allows safe identification of the CD and extrahepatic bile ducts during very difficult LCs, avoiding conversion to open cholecystectomy in 6% of cases. 7
Materials and Methods
Institutional review board approval was obtained before data collection. The data of all patients undergoing LC at a single academic institution by a single attending surgeon (S.P.B.) over a 29-month period was reviewed retrospectively. A surgical resident was the primary surgeon in each case.
The charts of 65 consecutive patients were reviewed. About 45 (69%) were women and 20 (31%) men. The mean age was 37.4 years and the mean American Society of Anesthesiologists classification 2.
Operations performed on patients admitted through the emergency room for biliary obstruction or acute inflammation were classified as urgent. Forty-three patients (66%) underwent LC urgently: 33 (51%) for acute cholecystitis, 6 (9%) for choledocholithiasis, and 4 (6%) for gallstone pancreatitis. Operations performed on an outpatient basis were classified as elective. Twenty-two patients (34%) underwent LC electively: 21 (32%) for symptomatic cholelithiasis and 1 (2%) for biliary dyskinesia.
Six patients (9%) with evidence of CBD obstruction underwent preoperative ERCP by the gastroenterology service. One patient had a retained CBD stone after ERCP, and underwent successful laparoscopic CBD exploration at the time of LC.
A 10 mm umbilical port was placed in the open Hasson technique and the abdomen was insufflated. After introduction of a 30 degree camera through the umbilical port, three additional ports were placed under direct observation: a 10 mm bladeless subxiphoid port and two 5 mm ports along the right costal margin. The gallbladder fundus was grasped and retracted cephalad, and the infundibulum retracted laterally to expose Calot's triangle. Using electrocautery, the lateral and medial peritoneal attachments of the gallbladder were fully released to improve observation and identification of vital structures. Impacted stones in the infundibulum were mobilized away from the CBD to facilitate IOUS.
After the release of the peritoneal attachments of the gallbladder, IOUS was routinely used in all patients when the equipment was available. A 10 mm laparoscopic ultrasonography device (Aloka or B&K) was introduced through the subxiphoid port, and a transverse view of the porta hepatis obtained. The Mickey Mouse view was obtained (Fig. 1), and duplex mode imaging was used to confirm correct identification. The CD–CBD junction was identified. The common hepatic duct and CBD were scanned from the liver hilum to the ampulla of Vater to measure the CBD diameter and detect CBD stones. Successful IOUS survey required observation of the CD–CBD junction, measurement of the CBD, and observation of the entire course of the common hepatic duct and CBD. The scan was repeated throughout the dissection as needed to ensure resident comfort with the scanning technique, and as clinically required.
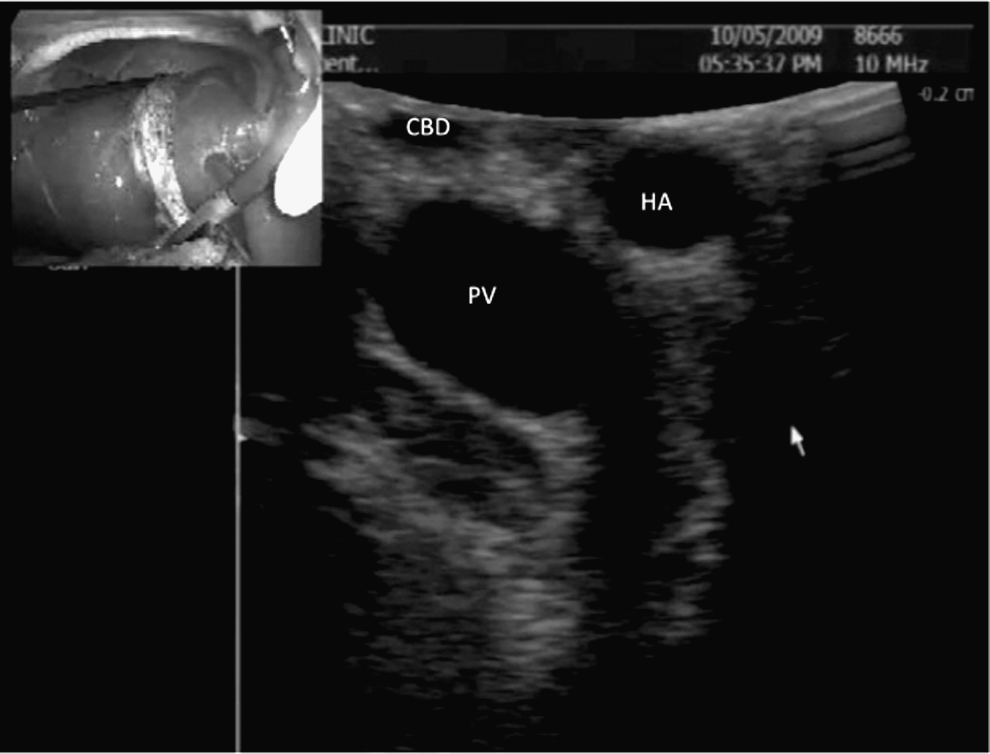
Ultrasonography view of Porta hepatis. CBD, common bile duct; HA, hepatic artery; PV, portal vein.
IOUS findings and the degree of inflammation in Calot's triangle guided the dissection method. In the majority of cases, the inflammatory adhesions in Calot's triangle were easily dissected, and the critical view was obtained (Fig. 2), allowing safe ligation and division of the CD and cystic artery. The gallbladder was then dissected from the liver bed using electrocautery and removed from the abdomen.

Critical view technique.
When inflammatory adhesions prevented establishment of the critical view, the lateral edge of the gallbladder was dissected from the liver at the level of the infundibulum. The cystic artery was ligated high on the medial aspect of the GB, and a window established around the infundibulum (Fig. 3). This dissection plane was then carried down to the Triangle of Calot and the CD identified. This dissection technique was termed the “infundibulum-down” approach.
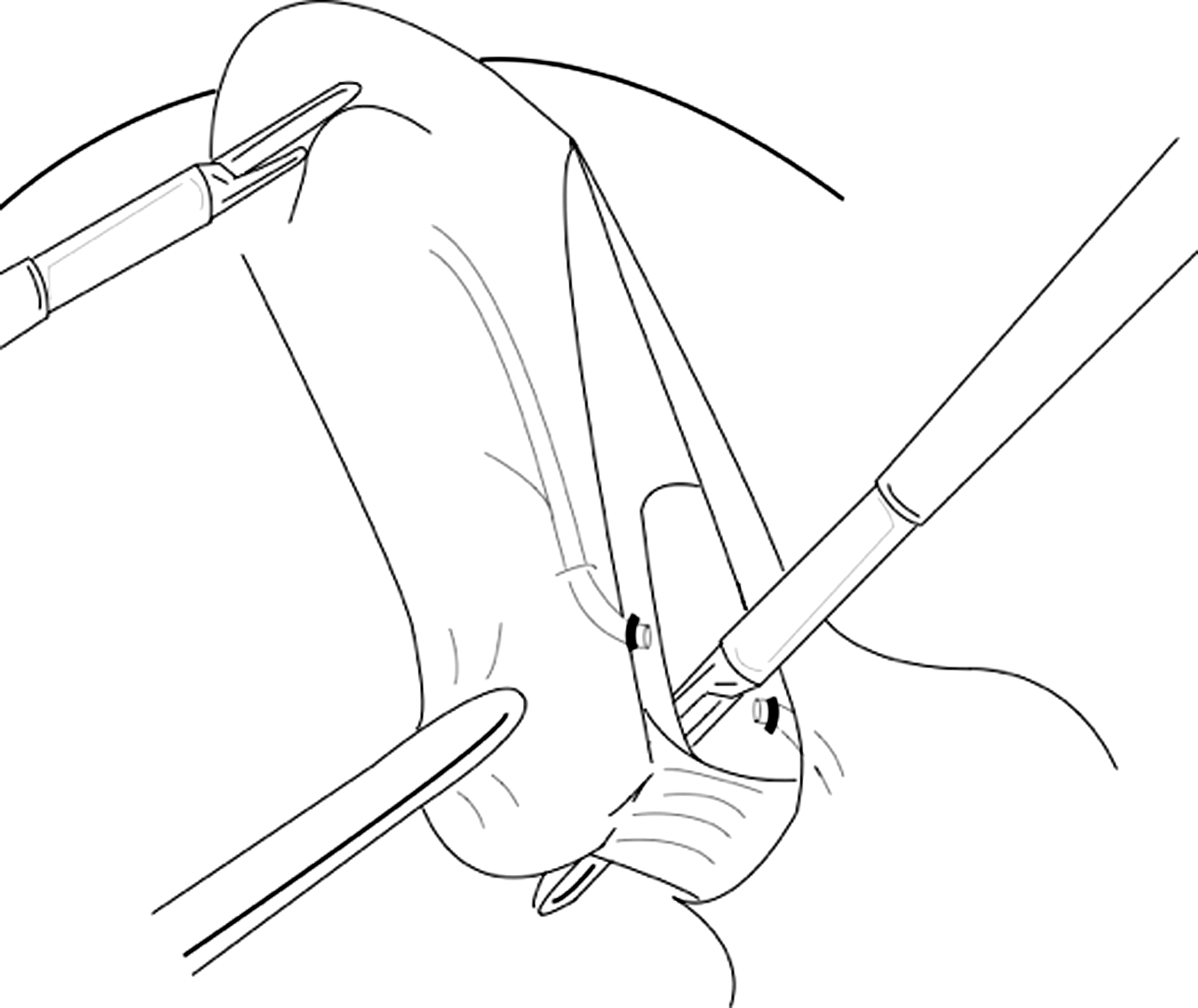
Infundibulum down technique.
The fundus-down approach was used when severe inflammation prohibited identification and safe dissection of the infundibulum. If the cystic artery could not be observed entering the GB because of inflammatory adhesions and a plane behind the infundibulum could not be safely established, the fundus-down approach was employed. A cotton gauze sponge was introduced into the abdomen and used to retract the liver cephalad. The dissection was initiated at the GB fundus, which was carefully dissected from the liver bed distally toward the CD (Fig. 4). The cystic artery was ligated when it was encountered.
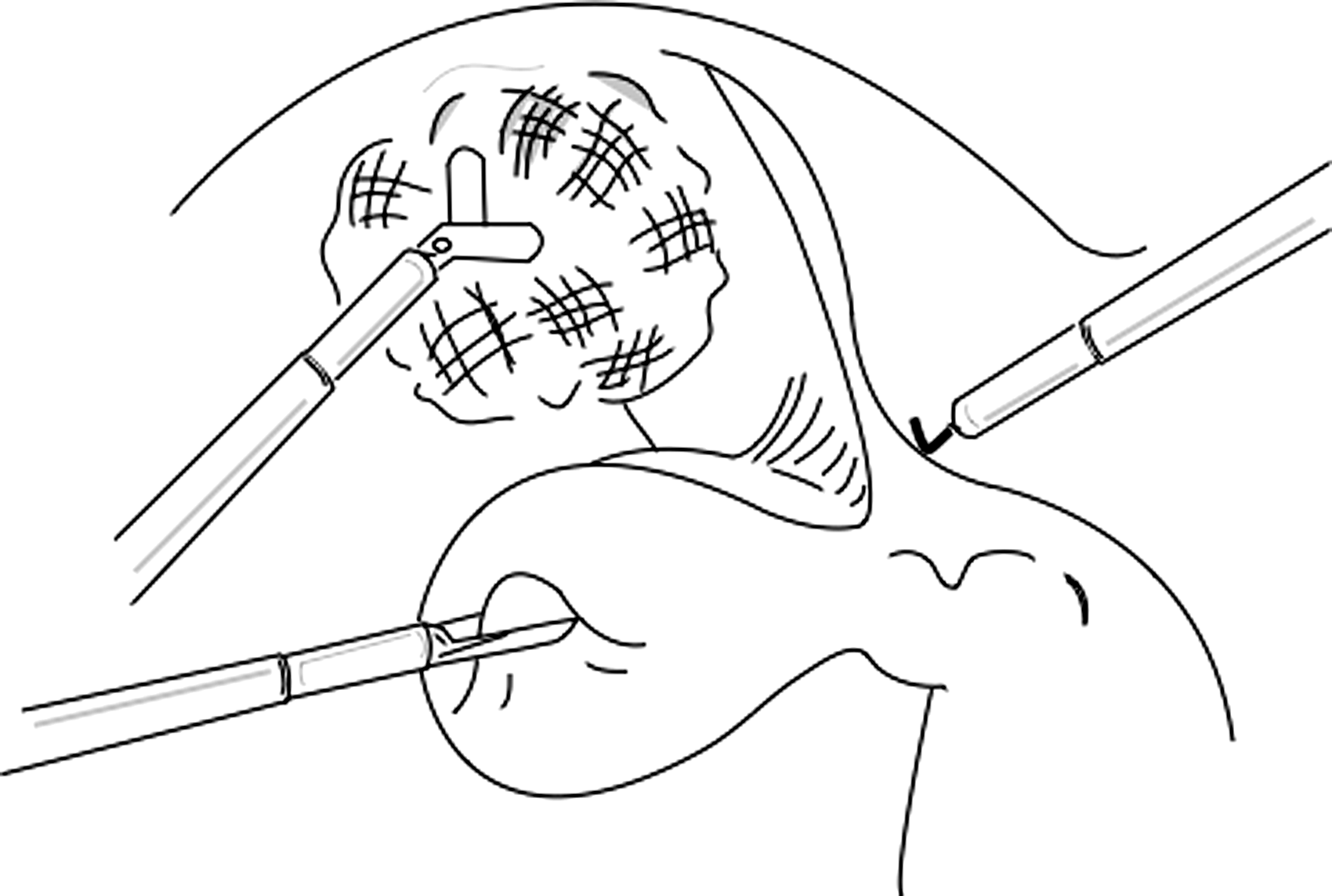
Fundus down technique.
When an impacted gallstone in the infundibulum restricted observation or exposure of the Triangle of Calot, or when inflammation rendered the CD undissectable, the “open infundibulum” approach was employed laparoscopically. A ligature was placed around the lowest circumferentially dissected portion of the gallbladder to minimize stone and bile spillage. The anterior infundibulum was opened and stones were retrieved to facilitate ultrasonography observation. Dissection proceeded if ultrasonography demonstrated an adequate CD length. When a short CD was encountered, the CD was oversewn from within the infundibulum, and the remnant gallbladder mucosa was ablated with electrocautery (Fig. 5).
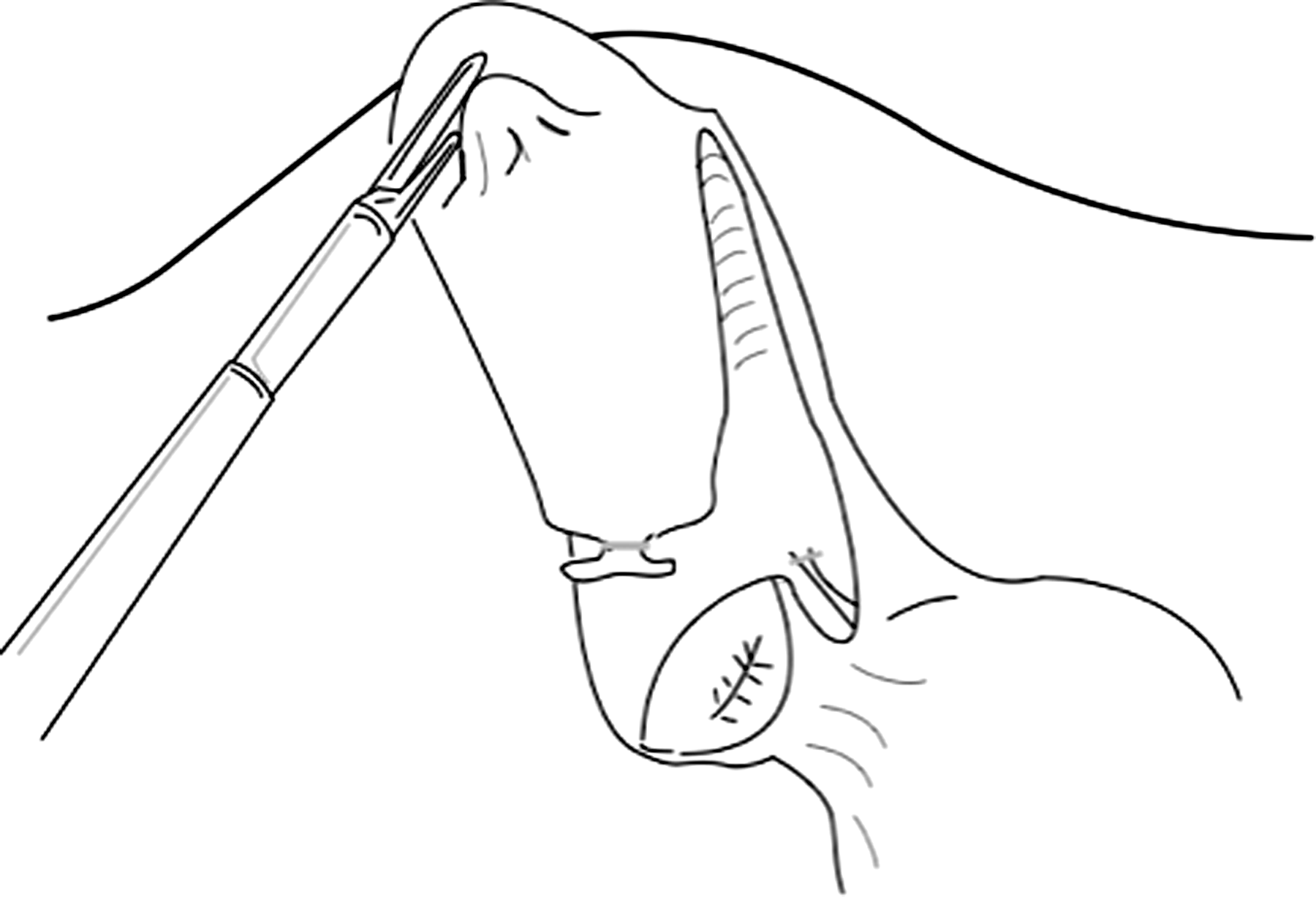
Open infundibulum technique.
Diagnostic IOC was performed when IOUS yielded incomplete CBD observation, or when IOUS was unavailable and bile duct observation was clinically indicated. Therapeutic IOC was performed when IOUS confirmed CBD stones. A high-volume mixture of saline and lidocaine was flushed intraductally, and intravenous glucagon was administered. Laparoscopic CBD exploration with stone retrieval was performed in cases of retained CBD stones after IOC.
Results
Mean operative time was 89.6 minutes (range 45–196 minutes). Dissection techniques included critical view in 50 patients (77%), infundibulum-down in 4 patients (6%), fundus-down in 4 patients (6%), and open infundibulum in 7 patients (11%).
IOUS was used in 50 patients (77%) and provided complete observation of the biliary anatomy in 48 (96%). The intrapancreatic CBD could not be observed in one case, and the CD–CBD junction was not seen in the other. Twenty-three significant biliary abnormalities were identified in 20 patients (40%), and are listed in Table 1. Aberrant vascular anatomy was encountered in 8 patients (16%), a foreshortened CD (<1 cm) in 7 patients (14%), abnormal cystic duct anatomy in 4 patients (8%), and CBD stones in 4 patients (8%). IOC was performed in 6 patients (12%): 2 patients for incomplete CBD observation by IOUS and 4 for CBD stones after IOUS. Two patients with CBD stones remaining after IOC were successfully treated with laparoscopic bile duct exploration.
CHD, common hepatic duct; RHA, right hepatic artery.
No cases were converted to an open operation. Mean postoperative length of stay was <1 day (range 0–6 days). No BDI occurred, and no subsequent biliary intervention was required. At 9 months postoperatively, one obese patient underwent uncomplicated surgical repair of a ventral incisional hernia at the supra-umbilical trocar site.
Discussion
Although the laparoscopic approach to cholecystectomy has been the preferred approach for nearly two decades, devastating bile duct injuries persist. The key to safe LC is correct identification of the CD at the time of operation. Releasing the medial and lateral peritoneal attachments of the gallbladder as the initial step of dissection provides improved gallbladder retraction, and it enlarges the working space in Calot's triangle. When the critical view of safety is established, the CD and cystic artery can be safely divided with confidence. 5 However, acute and chronic cholecystitis, impacted gallstones, and anatomic factors can make this view unobtainable. The critical view was obtained in only 77% of our patients. It is therefore important to be familiar with other methods of CD dissection, and we have attempted to describe our approach in these difficult cases. In our study population, 66% of patients underwent LC for an urgent indication. This figure is high because of our uninsured patient population's poor access to health. The majority of our patients were admitted through the emergency room with acute inflammation and underwent LC as inpatients.
IOUS, though used routinely by only a minority of surgeons, is well described in the literature. First used in open cholecystectomy (OC), it has been used in LC with increasing frequency over the last 10 years. IOUS has been reported to be associated with a lower incidence of BDI, 8 lower costs compared to routine IOC,8–10 and fewer conversions to OC. 8 It takes less time than IOC,9,11–15 is highly effective in observation of biliary anatomy,9,12,13,16 and its specificity in detecting CBD stones approaches 100%.11,13,16
This report suggests that routine IOUS may alert the surgeon of patients at risk of complications of LC. Abnormal biliary anatomy was demonstrated in over 40% of patients undergoing IOUS in our report, including 16% of patients with abnormal vascular anatomy (Fig. 6), 14% with a short CD (<1 cm), and 8% with CBD stones. It is difficult to estimate the clinical significance of these findings, but in LC for acute disease, correctly identifying biliary anatomy is crucial. In a report of 236 LCs utilizing IOUS by Perry, ultrasonography permitted safe identification of the CD and CBD during 13 very difficult LCs (6%), and allowed these cases to be completed without conversion to open cholecystectomy. 7 We believe the potential of ultrasonography findings to alter the operative course represents a real advantage of this technique.
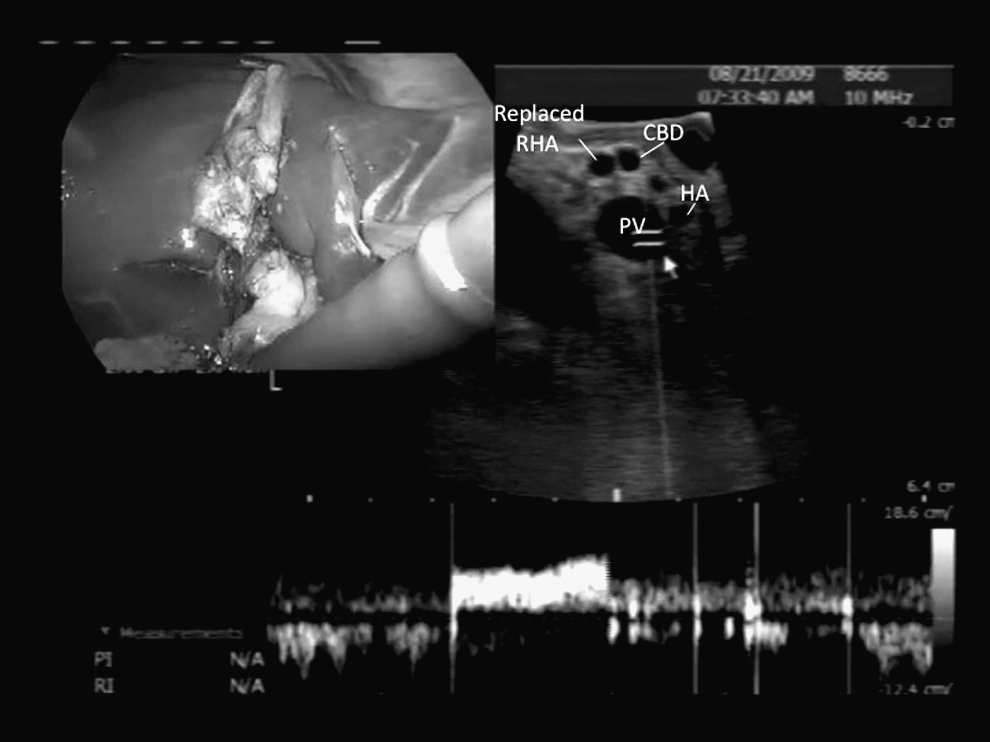
Ultrasonography view of replaced RHA. RHA, right hepatic artery.
Although one could advocate selective use of ultrasonography, routine use serves a better teaching role, not only for surgical residents, but also for operating room personnel responsible for operating the different modes of the ultrasonography machine. Although not specifically quantified in our results, we found that most residents are able to exhibit proficiency in IOUS after performing 10 cases, enabling them to subsequently use this technique in their own practices.
Footnotes
Disclosure Statement
No competing financial interests exist.