
Abstract
Abstract
Introduction:
India ink tattooing is widely used for tumor localization; however, the tattooing procedure is not yet standardized. This study aims to evaluate the efficacy of small-dose tattooing with sterile India ink using a saline test-injection method.
Patients and Methods:
Between April 2009 and August 2009, 20 patients underwent colonoscopic tattooing with prepackaged sterile India ink before resection of colorectal tumor. We injected 0.5 cc of India ink at three circumferential sites at the distal tumor using a saline test-injection method. Observation and leakage of India ink were evaluated during laparoscopic surgery, and the diameter of tattooing in the specimen was assessed.
Results:
Tattoos were observed intraoperatively in 18 patients (90%). In 2 patients, tattoos were not observed on the serosal surface but were detected on the mucosal surface. Localized leakage of ink was identified during surgery in 1 patient (5%), without fever or abdominal pain. Mean tattoo diameter was 2.1 cm on the serosal surface and 2.0 cm on the mucosal surface.
Conclusions:
Small-dose tattooing with sterile India ink using a saline test-injection method is effective for tumor localization.
Introduction
Colonoscopic tattooing is currently considered one of the most effective methods of tumor localization, with a previous study reporting observation and leakage rates of 80%–100% and 0%–14.3%, respectively.1–6 The procedure of India ink tattooing, however, has yet to be standardized. Our group reported previously that preoperative colonoscopic tattooing using a saline test-injection method with prepackaged, sterile India ink is a safe and effective method for tumor localization in laparoscopic colorectal surgery. 1 In the present study, we attempt to identify the appropriate amount of ink because spillage is greater at high injection volumes. This pilot study aims to evaluate the efficacy of small-dose tattooing with sterile India ink using a saline test-injection method.
Materials and Methods
This study enrolled 20 patients who underwent preoperative colonoscopic tattooing at the National Cancer Center, Korea, between April 2009 and August 2009. The study was performed in accordance with the Declaration of Helsinki and informed consent was obtained from all patients. The protocol was approved by the institutional review board of our hospital (NCCNCS-09-298).
Four expert endoscopists with over 7 years of specialist experience performed the preoperative colonoscopic tattooing. Patients were prepared with mechanical bowel preparation before colonoscopic tattooing. The patients received either two 45 mL doses of sodium phosphate (Fleet®; C.B. Fleet Co., Inc., Lynchburg, VA) or 4 L of polyethylene glycol solution (Colyte-F®; Taejoon Pharm, Seoul, Korea) and underwent colonoscopy under conscious sedation with midazolam.
Other than the amount of injection agent, the saline test-injection method was the same as that used in our previous study. 1 Using a 23 gauge sclerotherapy needle (Olympus Medical Systems Co. Ltd., Tokyo, Japan), 0.5 mL of saline was injected into the submucosal layer to form a proper submucosal elevation. Using a second syringe and needle, 0.5 mL of India ink (SPOT®; GI Supply, Camp Hill, PA) was injected per one injection site. This syringe was replaced by the first syringe containing saline, and 0.7 mL of saline was injected to flush out the India ink remaining in the needle device. The India ink was injected at three circumferential sites 120° apart and 1 cm distal to the tumor or previous endoscopic procedure site.
During the colonoscopic procedure, we classified the success of tattooing into four grades: excellent (well-observed three dark spots), good (well-observed two dark spots), fair (well-observed one dark spot), and poor (moderately or poorly observed three dark spots). We measured the diameter of preoperative colonoscopic tattooing in all resected specimens on both the serosal and mucosal surfaces. We examined whether tattooing sites were observed during surgery, and evaluated leakage.
Results
Patient characteristics are shown in Table 1. The mean age was 62 years (range, 34–80 years); 13 of the 20 patients were men. Nine of the 20 patients had undergone previous EMR. The median time interval between tattooing and surgery was 3 days (range, 0–45 days). The median procedure time for tattooing was 3 minutes (range, 2–15 minutes). The success of tattooing by the endoscopist was graded as excellent in 7, good in 9, fair in 3, and poor in 1. No patient experienced fever or abdominal pain after tattooing.
Time interval between tattooing and surgery.
T-colon, transverse colon; D-colon, descending colon; S-colon, sigmoid colon.
Indications for surgery were premalignant and malignant diseases of the colon (1 adenoma and 19 adenocarcinomas). The locations of lesions were 3 in the transverse colon, 2 in the descending colon, 14 in the sigmoid colon, and 1 in the rectum. Regarding the rectal lesion, we had considered that the tumor was located in the rectosigmoid colon based on preoperative examination, but the tumor was found in the upper rectum intraoperatively. Among the 19 cancer patients, 6 patients were stage II or III due to double primary lesions or the presence of a polyp that was malignant in appearance and located distal to the cancer.
Tattoos were observed intraoperatively in 18 patients (90%), with local leakage in 1 patient (5%). We were unable to locate the lesions during surgery in two patients whose lesions were located 18 and 15 cm from the anal verge. In these two cases, we conducted intraoperative colonoscopy to detect the lesions. In only 1 case, a small amount of India ink leaked locally into the mesocolon, without peritonitis or abdominal pain.
The mean diameter of the tattoos was 2.1 cm on the serosal surface (Fig. 1) and 2.0 cm on the mucosal surface (Fig. 2). The mean distal margin of the specimens was 5.0 cm.
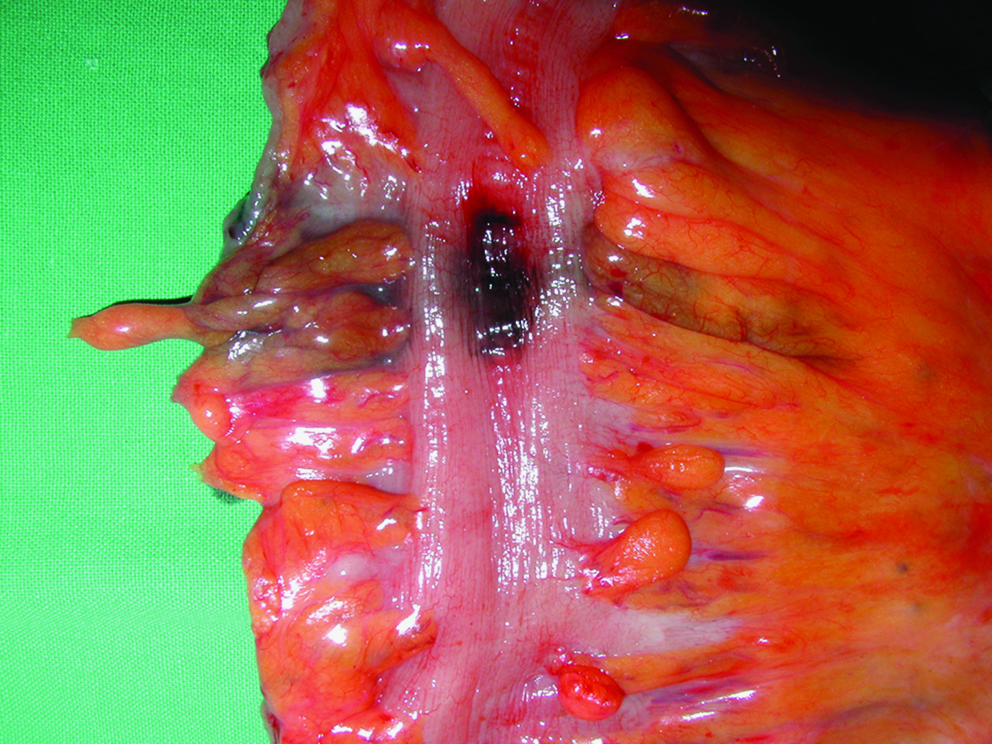
Gross appearance of serosal surface the colon specimen after the injection of India ink.
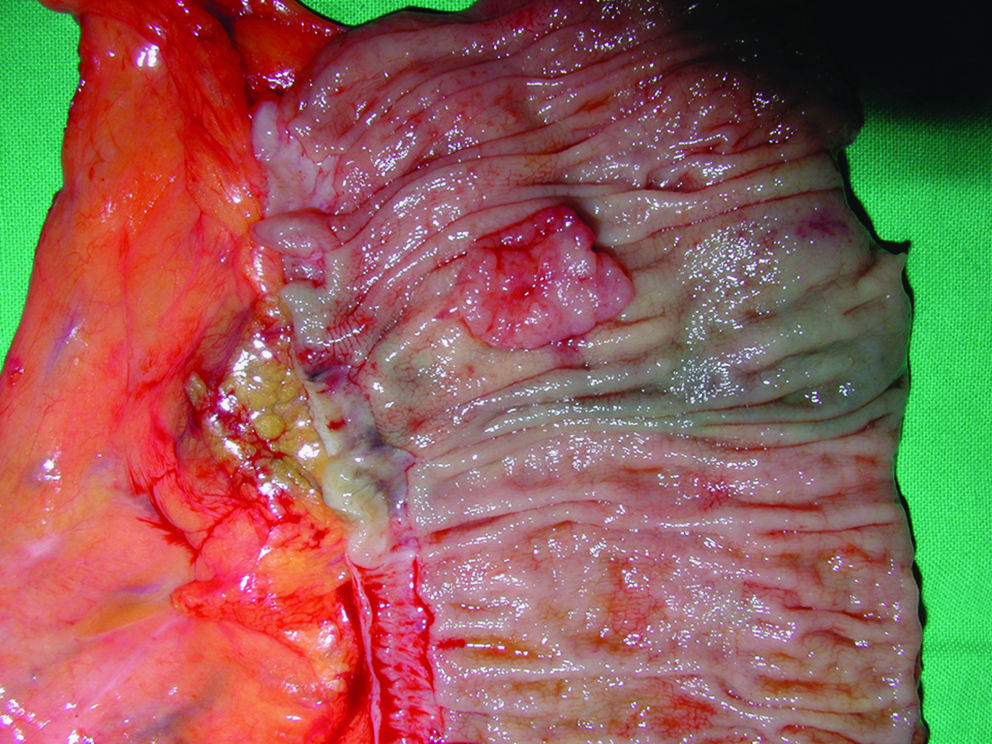
Gross appearance of mucosal surface the colon specimen after the injection of India ink.
Discussion
Several studies have shown that preoperative colonoscopic estimation of tumor location identifies tumor location incorrectly in up to 14% of cases. 7 There is a possibility that incorrect identification of tumor location invites a further laparotomy and resection of the missed tumor.7,8 Thus, precise preoperative localization is important in colorectal surgery. Early small lesions of the colon can be difficult to palpate, even at the time of open surgery and during laparoscopy, because of the lack of tactile sensation. Methods of tumor localization include barium enema examination, CT colonography, mucosal clipping, and tattooing; colonoscopy may be performed intraoperatively.8–11 Among these, endoscopic tattooing is the most reliable and widely used method of localization.12,13 Agents used for tattooing have included India ink, methylene blue, indigocarmine, and indocyanine green. India ink does not diffuse through the mesentery and is thus permanent. The incidence of clinically relevant complications after India ink injection is low (0.22%). 14 Methylene blue, indigocarmine, and indocyanine green also stain the bowel serosa, but these agents are rapidly absorbed and disappear within days.15–17
SPOT (GI Supply) is proven as a safe and effective agent and is widely used. 4 Previous studies using SPOT have reported no significant clinical complications such as infection, fever, or abdominal pain, even in cases of leakage, in agreement with the findings of the present study using SPOT. However, the leakage of ink can make it difficult to identify the tumor location. In this study, we attempt to identify the appropriate amount of ink because spillage is greater at high injection volumes. Two different methods are used for tattooing: traditional tattooing methods, in which the dye is injected directly into the colonic wall, 18 and the saline test-injection method in which sterile saline is injected into the submucosa to form a bleb, after which tattooing agents are injected, followed by a final injection of saline. In our center, we have used the saline test-injection method because it can improve observation and reduces leakage.1,2,19
In our experience, tattooing using 0.6–1.5 mL of India ink per injection gave observation and leakage rates of 75% and 5%, respectively, 20 whereas these rates were 98% and 9.5%, respectively, in a previous study that used 1–1.5 mL per injection. 1 In the present study, using 0.5 mL per injection, observation and leakage rates were 90% and 5%, respectively. By reducing the amount of India ink, observation was maintained and leakage rate was decreased. In terms of objective observation, the present study offers a unique perspective because the diameter of tattooing was measured. For injection of 0.5 mL of India ink using the saline test-injection method, the median serosal tattooing diameter was 2.0 cm (range, 0.5–4.0 cm). This tattoo size is thought to be appropriate for identifying the tumor site during operation.
Causes of nonobservation are multiple, including failure of submucosal injection (endoluminal spraying) and an inappropriate amount of saline or ink. Endoluminal spraying can be avoided by using the saline test-injection method. Fu et al. reported the injection of 3 mL of saline, 0.2 mL of India ink, and 2 mL of saline into the submucosal layer. 2 The total amount of injected fluid was 5.2 mL, which can cause inaccurate localization because the diluted ink causes the tattoo to appear indistinct and blurred. In the present study, the total amount of 1.7 mL of injected fluid enabled accurate localization because the tattoo was strong enough to be clearly visible. Table 2 shows a comparison of our results with the results of published studies describing preoperative India ink tattooing using the saline test-injection method for colorectal surgery.
In the present study, nonobservation occurred in 2 patients; in these cases, only mucosal tattoo was visible. The distances from the anal verge were 18 and 15 cm, and body mass indices (BMI) were 34 and 25 kg/m2 in the 2 patients. BMI is thought to be one of factor influencing the result of tattooing. In our study, BMI did not directly influence tattoo diameter (P > 0.05, detailed data not shown). However, it may not be reliable because it is limited by the small population in the present study. The other case of rectal tumor was also classified as nonobservation. Because the rectum is surrounded closely by the mesorectum, adjacent tissue can easily spread over the mesorectum during tattooing. Thus, a small amount of dye could become widespread and cause blurring; in this case of nonobservation, diluted ink may have resulted in the indistinct appearance of the tattoos. Therefore, we recommend marking at three locations 120° apart or at four locations 90° apart along the bowel circumference.
In conclusion, the results of the present study show that an injection volume of 0.5 mL of India ink is effective for accurate localization and prevention of leakage in colonic tattooing.
Footnotes
Acknowledgments
This study was supported by a grant from the National Cancer Center of Korea (NCC-0710362 and NCC-0910520). The authors wish to thank Jung Hyuk Suh, M.D., Sung Taek Jung, M.D., Sung Chan Park, M.D., and Hyo Seong Choi, M.D., for their assistance with data collection. All authors have no conflicts of interest or financial ties to disclose.
Disclosure Statement
No competing financial interests exist.