
Abstract
Abstract
There is a surge in interest in single-incision laparoscopic surgery in the recent years. Due to entry of all the ports and instruments from the same incision and obliquity of the instruments, the lowermost port exerts repeated pressure on the infraumbilical abdominal wall. We are reporting 2 cases of single-incision laparoscopic surgery cholecystectomy who presented with lower abdominal pain and contusion in the post operative period.
Introduction
Case Report
The first case is that of a 36-year-old woman who underwent SILS cholecystectomy for gallstone disease. The umbilicus was everted, and a vertical incision about 2.5 cm was made through its center. Blunt dissection was done to make space in the subcutaneous plane. Three ports were put as shown in Figure 1. A 10-mm rigid endoscope was passed through the 10-mm port, and rotaculating (Covidien, Norwalk, CT) or straight instruments were passed through two 5 mm ports for dissection as per need. Two sutures with 2-0 silk on a straight needle were taken through the fundus and the hartmann pouch of the gall bladder and taken out through the abdominal wall to give traction. There were moderately dense adhesions in the calot's triangle. The operation took about 100 minutes. The patient recovered well in the postoperative period, taking orally after 6 hours, and was discharged the next morning on tab diclofenac 75 mg twice a day. Postoperatively, she had a pain score of 1 out of 10 on visual analogue scale at 6 hours and a pain score of 2 at discharge (24 hours after the operation). The pain increased after discharge, and she reported a pain score of 5 at 36 hours postoperation, the pain being primarily in the infraumbilical region. On the second postoperative day (POD2), she was called for a check up. She was taking orally, passing flatus, and had normal vitals. On inspection, the abdomen and the wound were normal. On palpation, the abdomen was soft, and there was tenderness in the infraumbilical region. She was reassured and sent back home. The pain continued to the scale of 4/10 on POD3 as well. On POD4, she was again called for an examination, and tenderness was persisting in the infraumbilical abdominal wall. Muscle relaxant (Chlorzoxazone) was prescribed. She responded quite well and remained pain free after that. Analgesics and muscle relaxants were stopped on POD8.
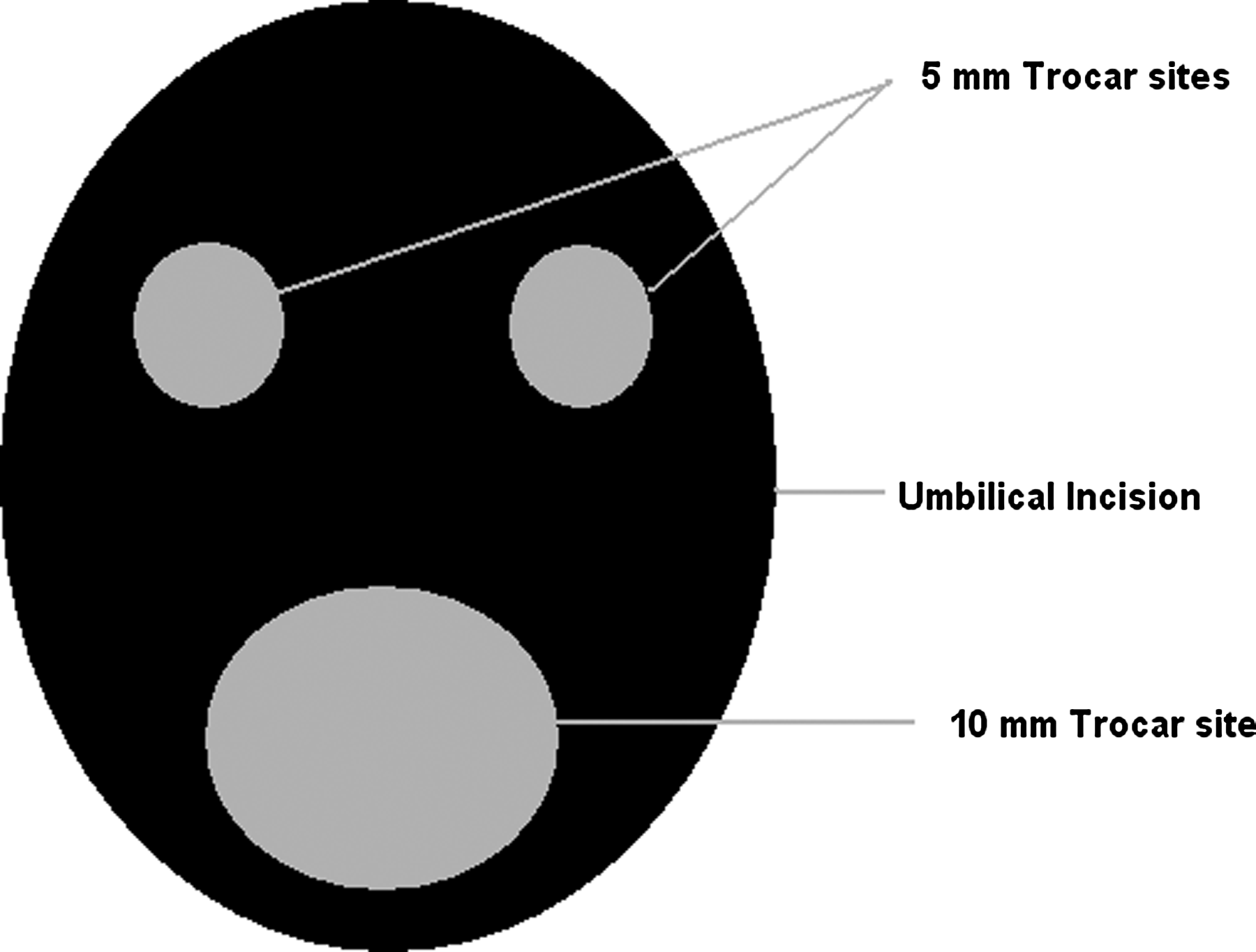
Port positions (diagram).
The second case was that of a 63-year-old man who also underwent SILS cholecystectomy for gallstones. He had a normal coagulation profile. The procedure and port positions (Fig. 2) were similar as described above. There were dense adhesions of omentum to the gall bladder and the cystic duct in calot's triangle. Due to difficulty in dissection because of these adhesions, the SILS operation was converted to four-port conventional laparoscopic surgery. The operation took 85 minutes for completion. The patient recovered well in the postoperative period and was discharged the next morning. Similar to the first patient, this patient also complained of increasing pain on POD1 with pain scores increasing from 1 to 5 on visual analogue scale. He also complained of pain primarily in the infraumbilical region. He was called for a check up on POD3. On inspection, a big contusion was seen on the anterior abdominal wall in the infraumbilical region (Fig. 3). The contused area corresponded to the region of tenderness. The same day, he was started on muscle relaxants to which he responded well. The patient remained asymptomatic on muscle relaxants and analgesics, and the contusion resolved in 10 days (Fig. 4).

Position of the ports.

Abdominal contusion—front view.

Contusion healed—10 days postoperation.
Discussion
As the experience with SILS grows, the complications specific to this procedure will become highlighted. The abdominal wall injury in the infraumbilical region leading to contusion and pain is one such complication. It has not been reported so far.
In SILS, all the ports and instruments enter the abdominal cavity from the same incision. There is paucity of space outside the abdomen for free movement of the instruments and since all the instruments are entering from the farthest port, they are also more obliquely placed compared with conventional laparoscopy. This leads to the lowermost port coming in contact and putting pressure on the lower abdominal wall (Fig. 2). Repeated pressure and longer duration of the operation (at least during the learning curve) could be the reason for the development of contusion. We put a 10-mm metal port in the lowermost position (Figs. 1 and 2). The wide 10-mm trocar could also be responsible for the pressure and the trauma.
This complication highlights the need for developing better instruments, slender longer ports, and light lead in line with the endoscope to increase the work space and better instruments with articulation at both the tip and the shaft.
Footnotes
Disclosure Statement
There is no support in form of grant, equipment, or anything else from any organization, company, or individual.