
Abstract
Abstract
Introduction:
A retroperitoneoscopic nephrectomy (RN) for symptomatic hydronephrosis (SH) is a challenging procedure because of the limited working space. This report describes a specific technical modification for efficient and successful RN for SH by using the SAND balloon catheter.
Patient and Methods:
A 38-year-old woman underwent RN for SH caused by extrinsic compression of the ureter by a pelvic endometriosis. The SAND balloon catheter was directly inserted into the expanded hydronephrotic sac, and the liquid was extracted, appropriately. Urine leakage from the hydronephrotic sac could be avoided because the puncture site was sealed firmly between the two adjacent balloons at the tip of the catheter. Disposal counter traction using the catheter facilitated the mobilization of the hydronephrotic sac.
Results:
The patient was discharged 3 days after undergoing this procedure.
Conclusions:
This method improves the surgeon's vision and facilitates resection without causing any injury to the hydronephrotic sac wall during RN.
Introduction
Methods
A 38-year-old woman presented with periodic right loin pain beginning in the middle of her menstrual periods and lasting for a few days afterward. She was found to have right severe hydronephrosis caused by extrinsic compression of the ureter by pelvic endometriosis in November 2004. She was initially treated with gonadotropin-releasing hormone analogs. However, the patient underwent the insertion of a Double-J stent and endometriotic excision with open laparotomic ureterolysis at Kurobe city hospital, because of the recurrent episodes of right pyelonephritis. The dissection started at the middle ureter, which was dilated without adhesions and progressed in the distal direction. Extensive involvement and obstruction of the distal part of the right ureter by the adjacent fibrotic cicatrizing tissue and the distal ureter could not be mobilized. Therefore, ureterolysis was abandoned. The adjacent fibrotic cicatrizing tissue was confirmed to be extraluminal endometriosis, histopathologically. Medical hormone therapy with danazol treatment was continued for 4 years; however, the periodic right loin pain related to the right hydronephrosis gradually became worse. The patient underwent a 99mTc-MAG3 with split function, which revealed the right kidney function to be only 6.7% of the total function. She was therefore referred to this hospital to undergo RN. Computed tomography and a retrograde pyelography demonstrated an advanced right hydronephrosis caused by the extrinsic compression by the pelvic endometriosis (Fig. 1). The patient underwent RN in February 2010 at Toyama University Hospital.
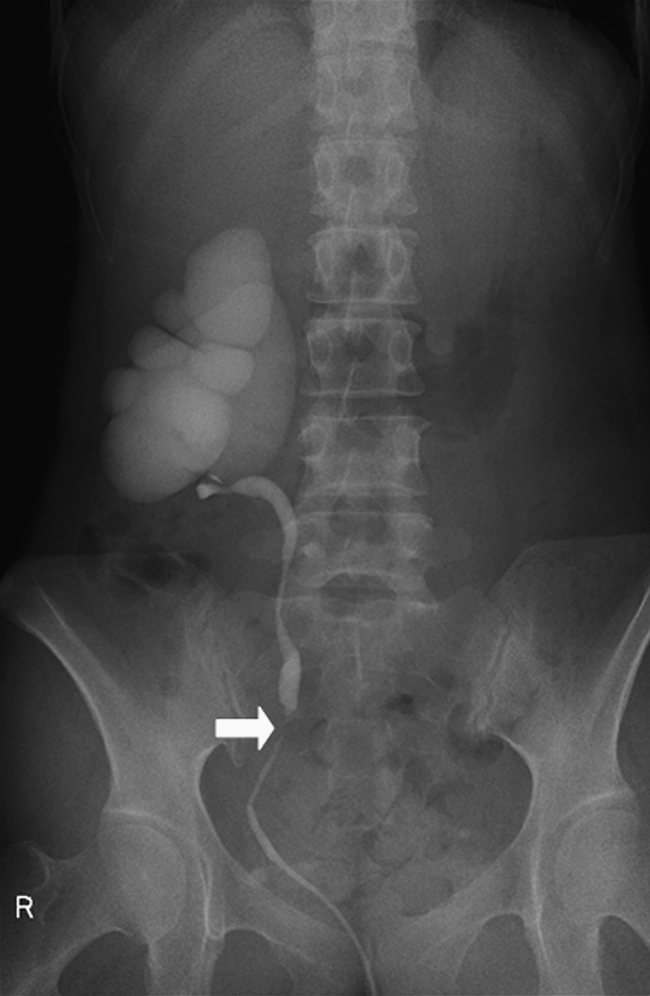
Retrograde pyelography revealed right giant hydronephrosis caused by an extrinsic obstruction (arrow) secondary to extraluminal endometriosis.
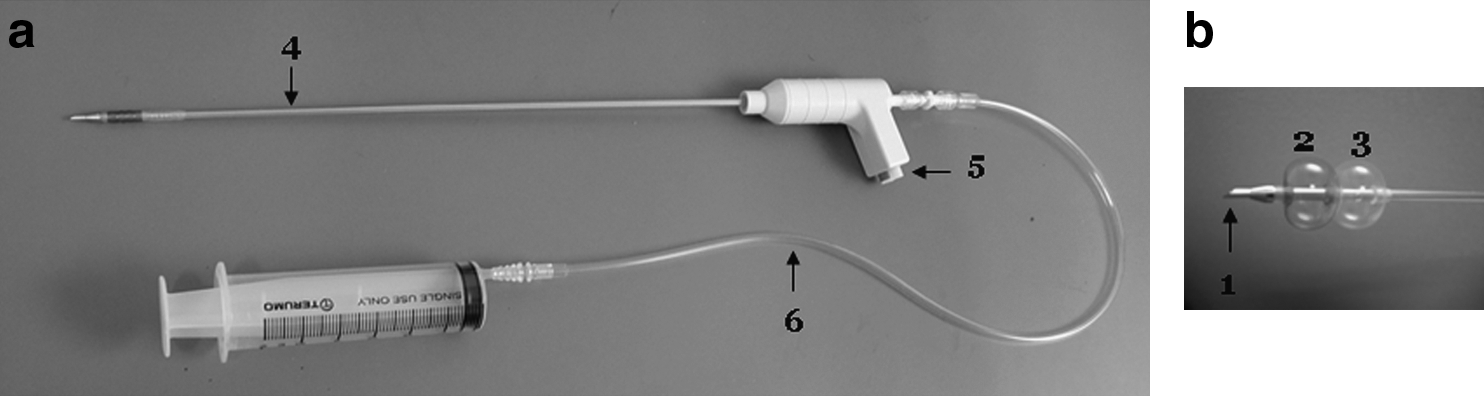
The patient was placed in the left-decubitus position. The first incision was made 2 cm below the tip of the 12th rib, and a retroperitoneum space was thus created using a preperitoneal distention balloon system. The working space was inspected through the balloon to ensure that the space was in the correct plane. Subsequently, the balloon trocar was replaced with a blunt-tip trocar, and insufflation pressure was maintained at 10 mm Hg. A 12-mm port was placed under vision in the anterior axillary line, while taking care to avoid the peritoneum. Another 5-mm port was placed posteriorly in the posterior axillary line. A grasper and monopolar scissors were used for dissection. The renal artery was identified anterior to the vena cava, ligated with clips, and divided. The renal vein was identified, and then carefully dissected and divided with an Endo-GIA stapler (ETSFlex 35 mm; Ethicon Endosurgery, Cincinnati, OH). The hilar vessels were dissected, and the kidney was mobilized from its remaining attachment. However, severe adhesion was found between the anterior kidney surface and the parietal peritoneum. The wall of the hydronephrotic sac remained intact. Next, a SAND balloon catheter was introduced through the 12-mm port, and the guide needle directly punctured the cavernous space within the hydronephrotic kidney (Fig. 2a). The diameter of this catheter was 2.75 mm and it contained two lumens that are connected to syringes, one for the balloon and one for the outflow or inflow port (Fig. 3). This catheter can be used through the port (>5-mm port) and there is no leakage of pneumoperitoneum during the procedure. The inner liquid was gradually removed through the catheter by the syringe. Next, the distal balloon was inflated with 5 cc saline in the inner liquid space. The distal balloon was adjusted to the thin wall adhering to the wall of hydronephrotic sac (Fig. 2b). Thereafter, the proximal balloon was inflated with 5 cc saline, thereby sealing the wall as soon as possible (Fig. 2c). After completing these maneuvers, the guide needle was removed. Leakage from the wall of the hydronephrotic sac could be avoided because the puncture site of the wall was sandwiched and sealed firmly between the two balloons. The expanded hydronephrotic sac was then drained easily and effectively by this catheter. However, a complete collapse of the sac was not useful because it was, therefore, difficult to identify the wall of hydronephrotic sac. Hence, the aspiration of the hydronephrotic sac was controlled.
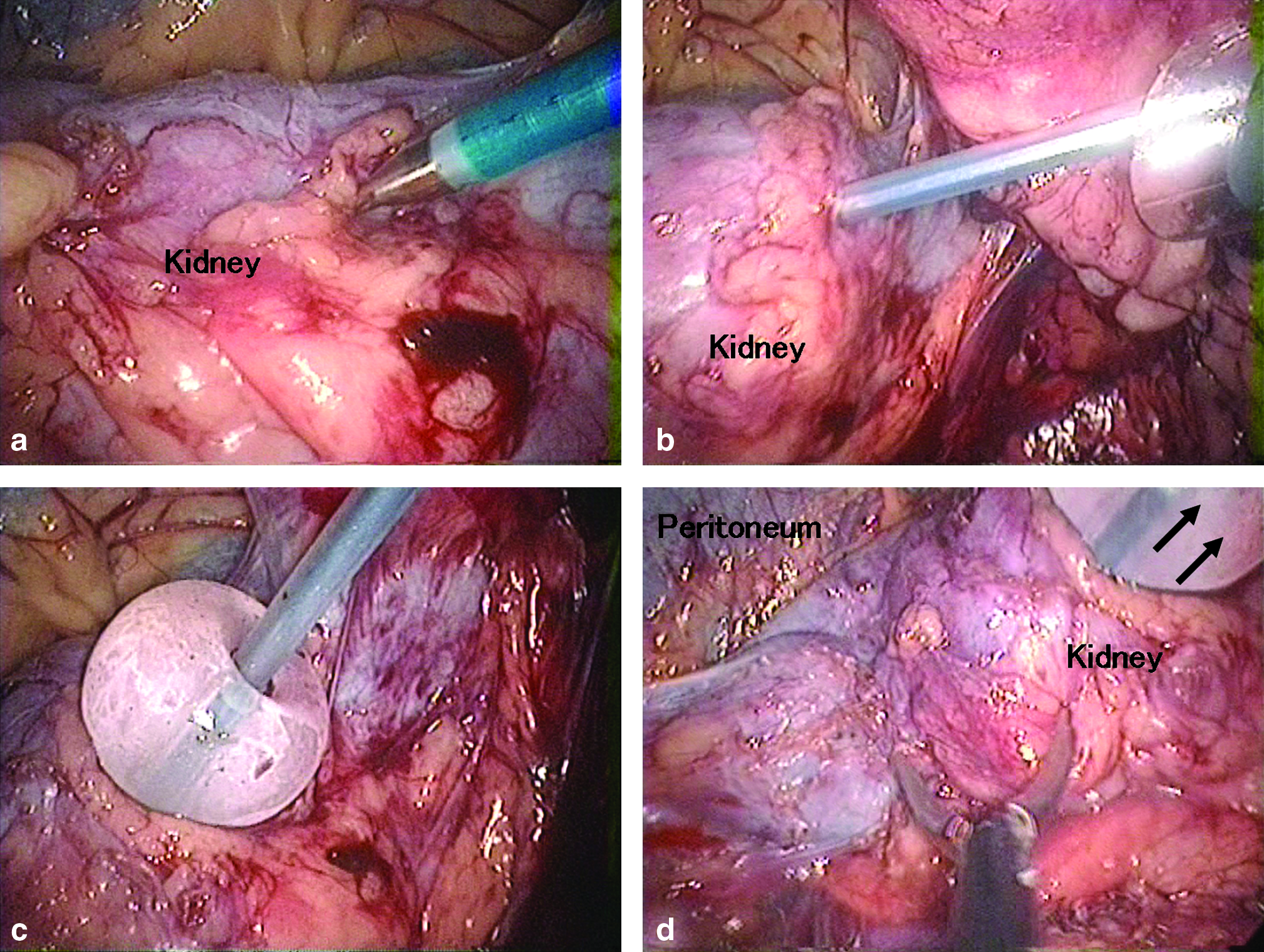
In addition, the SAND balloon catheter enables disposal and appropriate counter traction to expose the margin of the hydronephrotic sac and thus assists in its resection (Fig. 2d). Despite adhesion of the kidney to the surrounding structures as a result of previous inflammation, the disposal and appropriate counter traction of the SAND balloon catheter kept the margin between the thin hydronephrotic sac wall and surrounding tissue stretched, thus making it possible to perform a smooth dissection with sweeping movements. Gerota's fascia was dissected anteriorly from the parietal peritoneum without opening the thin hydronephrotic sac. This was followed by the complete excision of the hydronephrotic sac caudally and cranially as far as possible, using a Harmonic Scalpel (Ethicon Endosurgery) while leaving the hydronephrotic sac intact. The collapsed sac was kept on traction, and the ureter was identified, traced distally, and divided between the clips. Once free of the kidney, the hydronephrotic sac was inserted into the Endocatch (Endocatch Gold, 10 mm; Autosuture) with the SAND balloon catheter. Complete decompression of the hydronephrotic sac and deflation of the two balloons were performed within the Endocatch; therefore, no spillage of the hydronephrotic contents occurred. The originally huge hydronephrotic sac was removed through the camera port after the wound opening was enlarged to 3 cm. A drainage tube was left in place after the careful control of homeostasis, and irrigation with saline was then carried out. The fascial incision was closed with 2-0 Vicryl sutures and all wounds were closed.
Results
The operative time was 285 minutes, and blood loss was <50 mL. The resected kidney had a renal pelvic enlargement and parenchymal thinning, confirming no evidence of malignancy. Both walking and normal oral intake were allowed the next day. The patient was discharged 3 days after the surgery with no complications and no abdominal pain. Her periodic right loin pain related to her menstrual periods disappeared. She has since remained well with normal activity and good cosmetic results.
Comment
RN for SH is considered to be a more challenging procedure than RN for small nonfunctioning kidneys because of the limited space. Severe hydronephrosis limits the effective working space and observation of the lesion, which further thus limits the dissection. In addition, the risk of an inadvertent intraoperative rupture of the hydronephrotic sac because of the presence of dense adhesions around the kidney and possible spillage of its contents is another major concern. Although RN for SH is not technically impossible, it is difficult to resect such a huge kidney without violating the sac wall, because SH tends to usually be fairly large. Kojima et al. recommended ureteral catheterization for the drainage of urine from the hydronephrotic kidney to reduce the renal size and provide a better working space during surgery. 9 They emphasized that this technique limits the leakage of urine in the intraperitoneum and it is associated with fewer postoperative complications. Challacombe et al. recommended opening the renal pelvis and passing the laparoscope into the cavernous space within the kidney sac to facilitate the aspiration of the remaining fluid. The decompressed sac could be grasped using an Endo-Babcock and then be retracted through the anterior port site, extracorporeally. 4 However, the principle of surgery for resecting an inflamed mass must be the en bloc removal of the whole lesion without dissemination of its contents before leaving the body. This principle cannot be overemphasized.
This report describes a useful technique of hydronephrotic sac cannulation using the SAND balloon catheter. The outer diameter of the SAND balloon catheter is 2.75 mm; therefore, this catheter can be used through the port (>5-mm port) and there is no leakage of pneumoperitoneum during the procedure. In the center of the catheter is a needle, which punctures the expanded hydronephrotic sac. The needle, which has a diameter of 2.3 mm, can be removed after the puncture; this prevents tissue damage. Two balloons at the tip of the catheter grip and fix the sac wall in a stationary position. When the two balloons at the tip of the catheter are injected with 10 mL of physiological saline, each balloon swells to a diameter of ∼25 mm. The main advantage of this technique is the puncturing and suctioning of the sac contents early in the dissection, which facilitates mobilization of the hydronephrotic sac and allows the surgeon to maintain an adequate working space in the limited space. The leakage from the hydronephrotic sac can be also avoided because the puncture site of the sac wall is sandwiched and sealed firmly between the two balloons. However, complete collapse of the sac was not useful because it made identification of the sac wall difficult. Therefore, aspiration of the hydronephrotic sac must be controlled. An adequate volume of saline was simply injected through the catheter if too much suction was applied. The sac was then refilled to identify the distinct margin between the thin hydronephrotic sac wall and the surrounding tissue. When compared with the technique by using a laparoscopic suction needle to aspirate the contents and then an Endo-Babcock to provide traction and avoid spillage, our procedure significantly reduces the risk of spillage of the sac contents. The cost incurred by the use of the SAND balloon catheter was US$ 196. On the other hand, the cost incurred by the use of a laparoscopic suction needle (Hakko Medical Industry) and the Endo-Babcock (Covidien Autosuture, Mansfield, MA) was US$ 110 and US$ 274, respectively. Therefore, there was a savings of US$ 188 in our procedure.
Another advantage of this technique is that it allows for the disposal and counter traction of the hydronephrotic sac in an appropriate direction. This is necessary and important in cases where the kidney strongly adheres to the surrounding structures. In fact, Hemal et al. performed 12 RN for giant hydronephrosis and a peritoneal puncture occurred in 2 patients who underwent the standard retroperitoneal approach. 3 The adhesion of the kidney to the surrounding structures because of previous inflammation necessitated the disposal and appropriate counter traction for keeping the margin between the thin hydronephrotic sac wall and surrounding tissue stretched. The traction of the SAND balloon catheter was quite easy and precisely changed in a timely fashion; therefore, it allowed for the easy total mobilization of the hydronephrotic sac in the limited retroperitoneal space throughout the dissection. Moreover, this technique restores the tactile sense of touch to the surgeon, which thus allows the surgeon to avoid excessive and traumatic traction, while also reducing the risk of injury to the hydronephrotic sac and the thin parietal peritoneum. The complete decompression of the hydronephrotic sac and deflation of the two balloons and within the Endocatch were performed after freeing the sac from the kidney. Therefore, the originally huge hydronephrotic sac was extracted via a minimal incision (3 cm) and no spillage of the hydronephrotic contents occurred.
Conclusion
This new technique is therefore considered to be safe, feasible, and effective for solving the dilemmas associated with performing an RN for SH. This method improves the surgeon's vision and facilitates the performance of a resection without causing any injury to the sac wall during RN. This technique may also be useful for cystic lesions on other organs.
Footnotes
Disclosure Statement
No competing financial interests exist.