
Abstract
Abstract
Background:
Weight regain after Roux-en-Y gastric bypass (RYGB) is one of the possible complications bariatric surgeons are confronted with. An option for enhancing weight loss is the conversion of RYGB into distal RYGB (DRYGB), which is a malabsorptive procedure. We report the technical strategy and the preliminary outcomes of conversion of RYGB to DRYGB by laparoscopy.
Patients and Methods:
Between April 2005 and November 2009, 7 patients benefited from laparoscopic conversion of RYGB to DRYGB for weight regain mainly due to a new dietary behavior, namely, polyphagia (eating too frequent meals). At the time of RYGB, the mean weight and BMI was 120.5 ± 26.4 kg and 43.2 ± 6.7 kg/m2, respectively. Five patients suffered of obesity-related comorbidities. Mean interval time between RYGB and conversion was 41 ± 15.9 months. At the time of conversion, the mean weight, BMI, % excess weight loss were 100.7 ± 19.8 kg, 36.1 ± 4.8 kg/m2, and 33.7% ± 12.1%, respectively. Obesity-related comorbidities at that time affected 4 patients.
Results:
Mean operative time was 122.1 ± 34 minutes. There were no conversions to open surgery and no mortality. Postoperatively, 1 patient suffered of a bleeding. Mean hospital stay was 4.7 ± 2.5 days. After a mean follow-up of 19 ± 23.7 months, the mean weight, BMI, and % excess weight loss was 82.5 ± 19.7 kg, 29.5 ± 5.3 kg/m2, and 57.6% ± 8.1%, respectively. Obesity-related comorbidities remained unchanged after the conversion in the 4 patients. One patient required a surgical reoperation for internal hernia.
Conclusion:
Conversion of RYGB to DRYGB for weight regain can safely be performed by laparoscopy, with satisfactory early results.
Introduction
Possible causes of weight regain after RYGB can be related to technical failures as gastric pouch dilation, gastrojejunal anastomosis dilation, and development of gastro-gastric fistula. More often than not, weight regain depends on new dietary behavior of the patient. Treatment will take into account the cause of weight regain, with consequent proposal of revisional surgery by laparoscopy4,5 or endoluminal.6–9
As with other bariatric procedures, patients after RYGB frequently develop new dietary habits as hyperphagia, polyphagia, or sweet eating. In presence of hyperphagia (volume eating or eating too large meals), treatment can consist in increasing the restriction compartment, by placing around the gastric pouch an adjustable gastric band10–12 or a nonadjustable ring. 13 In the presence of polyphagia (eating too frequent meals or grazing), a conversion to malabsorptive procedures can be proposed. 14 In case of increased caloric intake by sweet eating, a conversion to malabsorptive procedures such as duodenal switch (DS) could be proposed as well. 15 Obviously, the nutritionist's counseling constitutes an important part of the multidisciplinary consultation, since mental disorders, such as binge eating and night eating disorders, must be ruled out. Consequently, it is our attitude, in absence of mental disorders, 16 to offer conversion to distal RYGB (DRYGB) in patients with RYGB presenting weight regain due to a new polyphagia diet.
In this retrospective study we report the technical strategy and the preliminary outcomes of the conversion of RYGB to DRYGB by laparoscopy, in a selected group of patients presenting weight regain due to de novo polyphagia behavior.
Patients and Methods
Between April 2005 and November 2009, 7 patients (5 females and 2 males) benefited from laparoscopic conversion of RYGB to DRYGB. The patients were informed of the new digestive circuit, of main advantage in term of weight loss and disadvantages in term of increased flatulence, bloating, and frequency of bowel movements.
Reason of conversion was weight regain, predominantly due to a new dietary behavior, such as polyphagia, diagnosed at the nutritionist's counseling. The psychologist's counseling ruled out mental disorders. The rest of the multidisciplinary consultation (gastroenterologist and radiologist) performing preoperative gastroscopy and barium swallow excluded technical causes for weight regain.
At the time of RYGB, the mean weight and BMI was 120.5 ± 26.4 kg (87–161) and 43.2 ± 6.7 kg/m2 (33.2–52.4), respectively. Obesity-related comorbidities affected 5 out of 7 patients, including arterial hypertension (2), type 2 diabetes (2), sleep apnea (2), and degenerative joint diseases (1). Mean age at the time of conversion was 51.8 ± 11.2 years (38–71). Mean interval time between RYGB and conversion was 41 ± 15.9 months (22–66). In this interval time, the extreme achieved weight, BMI, and %EWL was 91.1 ± 18.2 kg (67–115), 34.4 ± 6.1 kg/m2 (25.5–43.8), and 49.1% ± 14.5% (24.3–66.6), respectively.
At the time of conversion, the mean weight, BMI, and %EWL were 100.7 ± 19.8 kg (75–129), 36.1 ± 4.8 kg/m2 (28.6–44.6), and 33.7% ± 12.1% (12.1–46.1), respectively. Four out of 7 patients suffered from obesity-related comorbidities, including arterial hypertension (1), type 2 diabetes (1), sleep apnea (1), and degenerative joint diseases (1).
The main objective of our study was to describe the feasibility of our technique by laparoscopy and to document whether the conversion we used might lead to some success in terms stopping weight regain and reinducing further weight loss. Our sample size was small preventing us to carry out any statistical inference. We therefore used descriptive statistical methods. We reported frequency tabulations for categorical variables and mean and standard deviation as summary parameters of the observed distributions of continuous covariables or outcomes. The main criteria of evaluation was the %EWL calculated on the basis of the initial weight before the procedure of RYGB. The ideal weight for evaluation of %EWL was set at a BMI of 22 kg/m2. We also reported graphical representations of means of continuous outcomes during the first follow-up period and the second follow-up period.
Surgical technique
The patient was positioned supine with the legs apart and with both arms in abduction (French position). The surgeon stood between the patient's legs, the camera person to the patient's right, and the assistant to the patient's left. The procedure started with the insertion in the abdomen of the first 12-mm trocar using the Hasson technique on the left upper quadrant midclavicular line. Three additional trocars were placed under view, usually at the same position as in the original surgery: a 10-mm trocar some 20 cm below the xyphoid process, a 5-mm trocar on the right midclavicular line on the same horizontal line, and a 5-mm trocar just distal to the xyphoid process (Fig. 1). The procedure started by identification of the gastrojejunostomy, after adhesiolysis between the abdominal wall and Roux limb, and between the left liver lobe and the gastrojejunostomy. Once the anastomosis identified, the Roux limb was measured precisely by stretching the bowel along a 25-cm tape. The jejunojejunostomy came into view and each limb was marked at this level using 3 differently colored stitches, to identify the Roux, the biliary, and the common limbs. The Roux limb proximal to the jejunojejunostomy was sectioned by a firing of a linear stapler blue load (EndoGIA; Covidien, New Haven, CT) (Fig. 2a). The patient, camera person, and assistant now moved to the patient's left. The ileocaecal valve was identified and the small bowel measured so as to reach a total of 300 cm, including the previous Roux limb. At that level, a new side-to-side linear mechanical jejunojejunostomy (one firing of linear stapler white load and two 2/0 polydiaxone running sutures for the openings closure) was performed between the Roux and the new common limbs (Fig. 2b). The newly created mesenteric defect was closed by a nonabsorbable purse string suture (1 polypropylene). Cholecystectomy was performed as well, and the gallbladder retrieved by the left 12-mm upper quadrant trocar. The latter was closed in layers. The patient was allowed to a liquid diet on the first postoperative day, and typically was discharged from the hospital with a protein-rich diet.

Placement of the abdominal trocars.
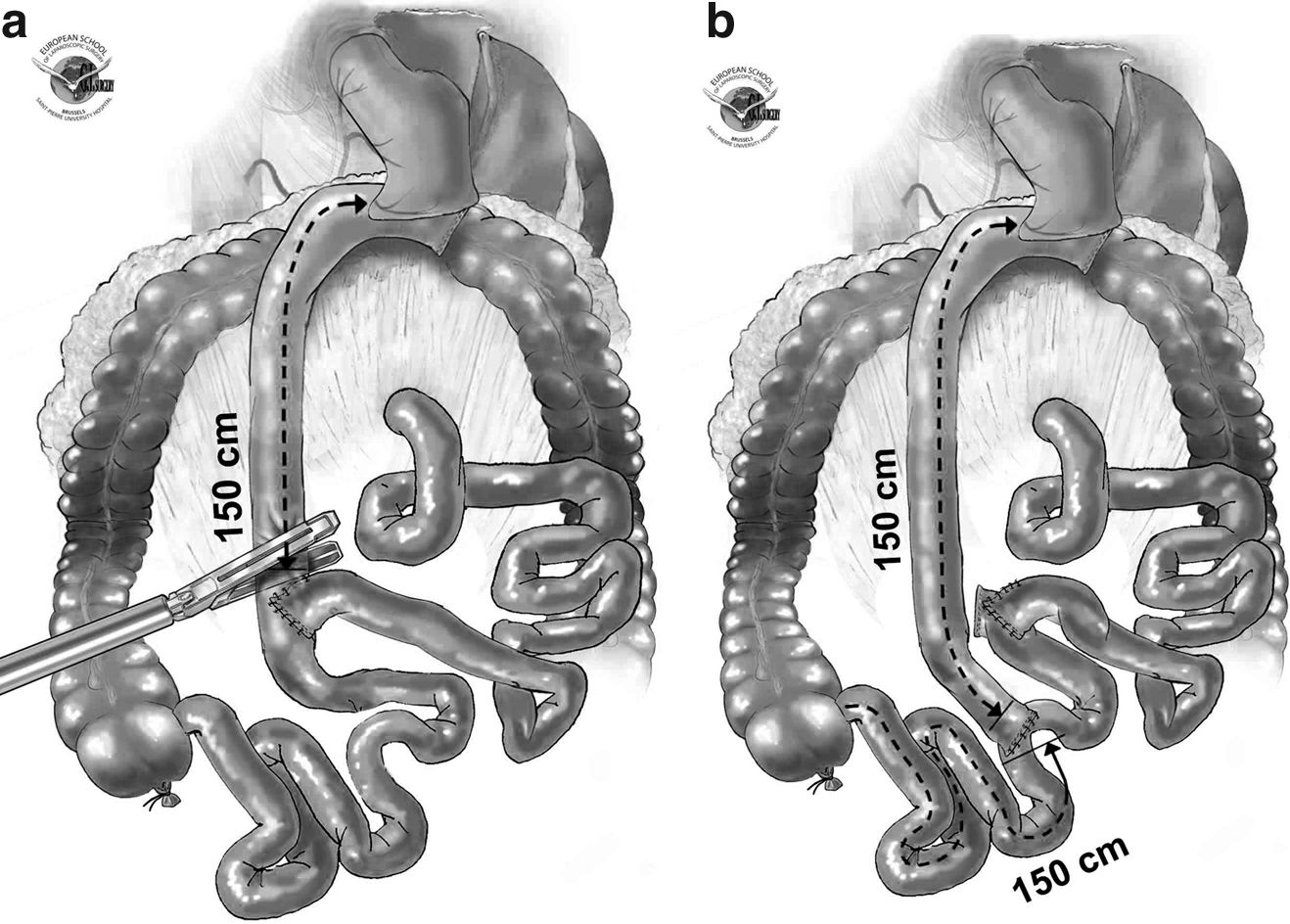
Schematic illustration of the conversion of RYGB to DRYGB: transposition of the distal end of Roux limb
Results
Peroperatively the Roux limb length appeared to measure exactly 150 cm, except in 1 patient where it was 110 cm. Gallbladder was still present at the time of the revision in 3 out of 7 patients; hence, cholecystectomy was performed in these latter patients. The internal hernia sites were systematically closed in all patients.
Mean operative time was 122.1 ± 34 minutes (90–180). There were no conversions to open surgery, and no mortality.
During the postoperative course, 1 patient (14.2%) suffered a significant abdominal bleeding, treated by blood transfusions. Mean hospital stay was 4.7 ± 2.5 days (2–10).
All patients were followed-up by office visits, with complete blood test, including albumin and protein level. After a mean follow-up of 19 ± 23.7 months (2–56), the mean weight, BMI, and %EWL was 82.5 ± 19.7 kg (52–105), 29.5 ± 5.3 kg/m2 (19.8–37.2), and 57.6% ± 8.1% (50–120.6), respectively (Fig. 3). No protein malnutrition or hepatic function failures were evidenced during this follow-up time, but all patients referred an increased flatulence and frequency of bowel movements. Frequency bowel movement was mostly influenced by the dietary, increasing with fat-rich diet. Obesity-related comorbidities affecting the 4 patients before the conversion remained unchanged during this follow-up time. One patient (14.2%) presented a late complication consisting of intestinal occlusion due to internal hernia, which required surgical reoperation.
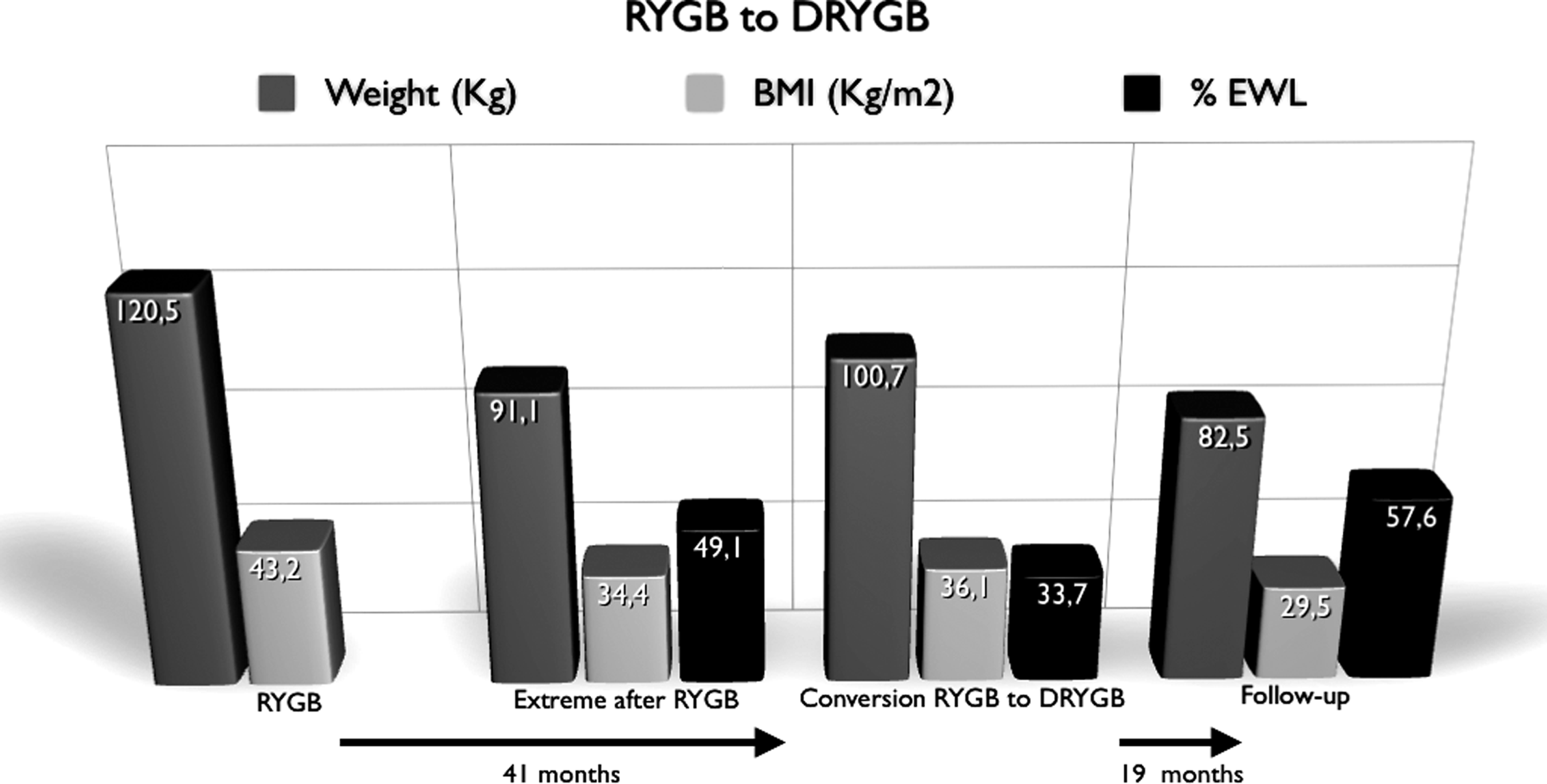
Comparison of weight, BMI, and % excess weight loss (%EWL) at RYGB, at extreme values before the conversion to DRYGB, at the conversion, and at follow-up (mean values).
Discussion
Provided mental disorders were ruled out, patients submitted to RYGB presenting weight regain due to new eating behavior such as polyphagia can benefit from conversion to DRYGB. The procedure of DRYGB was first reported to induce better weight loss than the standard RYGB in superobese patients, in a randomized trial. 17 The same authors also reported the conversion of RYGB to DRYGB for failures in superobese patients, and achieved a %EWL of 67% ± 5% and 69% ± 5% at follow-up of 3 and 5 years, respectively. 18 In this latter study, in 22 patients the revision included creation of a Roux limb of 145 cm and a common limb of 150 cm, whereas in 5 patients Roux limb of 200 cm and common limb of 50 cm were created. The reason of lengthening of the common limb in 22 out of 27 patients was mainly based on the development of severe protein–calorie malnutrition during follow-up.
In our department we adopted a similar technique as reported by Sugerman et al. 18 We created a total Roux and common limbs length of 300 cm. In our study, enrolling a smaller number of patients, we recorded a %EWL of 57.6% ± 8.1% at a mean follow-up of 19 ± 23.7 months, which is quite similar to that reported of 61% ± 4% at 1 year by Sugerman et al. 18
A similar revision with quite similar digestive construction was also reported by Fobi et al., 19 who revisioned 65 patients from RYGB to DRYGB. The authors reported a decrease of BMI from 41.8 to 34.6 kg/m2 after more than 1 year of follow-up. This is higher than our mean BMI of 29.5 ± 5.3 kg/m2, but this must be weighed against BMI level at the time of the conversion, and take into account the small series of our patients. Obviously, the increased weight loss after the revision is related to the addition of a malabsorptive process, which, on the other hand, can lead to protein malnutrition as late complication. Both Sugerman et al. 18 and Fobi et al. 19 reported late protein malnutrition, in 4 (18.1%) and 15 patients (23.2%), respectively. Furthermore, Brolin et al. corroborated these findings later. 14 Our follow-up time is one of the major weak aspects of the article, and could explain way in this limited time we did not record any proteins deficiency. On the other hand, other side effects, such as increased flatulence and frequency of bowel movements, were achieved in our patients. Interesting seems the increase of frequency bowel movement mostly related to the dietary type, especially fat-rich diet as it usually occurs in patients with other malabsorptive procedures as biliopancreatic diversion or DS.
Technically speaking, it is our strategy to start by a limited adhesiolysis in the left upper quadrant, just sufficient to obtain vision of the proximal end of the Roux limb and gastrojejunostomy, so as not to jeopardize the vascularization of this area. Then, the Roux limb is measured precisely allowing exact measurement of the new entire length of active bowel of 300 cm. It is mandatory to be able to recognize all three components at all times during surgery. This is the reason for placing different colored stitches on the loops of the three components at the jejunojejunostomy (distal end of the Roux limb, distal end of biliary limb, and proximal end of the old common limb). Placement of the marked stitches is extremely helpful because the measurement of the new common limb and the new jejunojejunostomy are performed using a different position of the surgeons (at the patient's left), which leads to confusion. The distal end of the Roux limb has to be sectioned close to the jejunojejunostomy, taking care to avoid stenosis. Finally, it is mandatory to close the new mesenteric defect, which is usually large and sometimes appears difficult to close, if exposure is not sufficient.
Our operative time highly depends on the sometimes lengthy adhesiolysis, but overall it is the measurement of the Roux and the new common limbs, which take the most time. Moreover, time to perform cholecystectomy, where it is present, has to be counted as well. We recommend performing cholecystectomy during this type of revision, because in 50% of the patients submitted to DRYGB, another revision was necessary for the development of cholecystitis. 18
In our study we recorded only one early complication as bleeding, which was medically treated. Consequently, hospital stay was longer in this latter patient. Usually, however, since the procedure involves just the dismanteling of the jejunojejunostomy and the manufacturing of a new anastomosis in another segment of the small bowel, the hospital stay is kept short. Anyway, other possible early complications, such as leaks, small bowel obstruction, or wound infection, can contribute to quite longer hospital stay. 19
Obesity-related comorbidities, affecting 4 out of our 7 patients at the time of the revision, remained unchanged during this follow-up, which is remarkable considering the satisfactory weight loss.
In this selected series of patients, we registered one late complication. Six months after the revision, the patient presented an intestinal occlusion due to internal hernia, which required a resection of the biliary limb by open surgery. This complication, well reported after the procedure of primary RYGB, 20 could become very dangerous in this category of patients, especially when the bowel resection includes the common or Roux limbs length, which are critical. Moreover, these data confirm that despite closure of the defect, as it was for our patient, the risk of the defect to open always persists. 21
In conclusion, conversion of RYGB to DRYGB for weight regain can safely be performed by laparoscopy, with satisfactory early results.
Footnotes
Disclosure Statement
No competing financial interests exist.