
Abstract
Abstract
We report a case of a perforated duodenal diverticulum that was diagnosed by computed tomography and treated by laparoscopic diverticulectomy. A 61-year-old woman visited the emergency room complaining of severe, sudden abdominal pain with nausea and vomiting. Computed tomography showed a round space containing air bubbles and food material in the posterior aspect of the second duodenal portion. The patient underwent an emergency laparoscopic exploration. Entering the posterior side of the duodenum, dirty reactive fluid was drained and an ∼4-cm perforated diverticulum was revealed at the posterolateral aspect of the second duodenal portion. After completing the peridiverticular dissection, a diverticulectomy was performed using ultrasonic shears, and the opening of the diverticulum was closed in two layers using intracorporeal hand-sewn sutures. She was discharged on postoperative day 10 without complications. To our knowledge, this is the first report of laparoscopic resection of a perforated duodenal diverticulum.
Introduction
Perforation is the rarest complication of duodenal diverticula, but is also associated with a mortality of up to 30%.1,5 No guidelines for treating perforated diverticula exist because of their rarity. Although nonoperative or endoscopic treatment of perforations can be attempted,6,7 care must be taken to not delay the surgical treatment. Concerning the surgical treatment, resection of the diverticulum after the Kocher maneuver with one- or two-layer closure of the duodenum has been described most frequently, but more aggressive surgery such as the Whipple procedure may be needed, depending on the location and grade of inflammation.
Several reports have described a laparoscopic approach for duodenal diverticula, with either diverticulectomy or an inversion procedure. This minimally invasive surgery can be limited by the location or extent of inflammation. We performed a laparoscopic diverticulectomy for an inflamed, perforated duodenal diverticulum successfully. To our knowledge, this is the first report of a perforated duodenal diverticulum treated by laparoscopic diverticulectomy.
Case
An institutional review board approved review of the case. A 61-year-old woman developed sudden, severe pain in the right upper abdominal quadrant with nausea and vomiting. She had been diagnosed with gastroesophageal reflux disease about 3 years earlier. On admission, she appeared acutely ill, and her blood pressure was 110/70 mm Hg, pulse 72 beats/min, and body temperature 36.8°C. On physical examination, the abdomen was not rigid, but there was direct and rebound tenderness in the right upper quadrant, with mild muscle guarding.
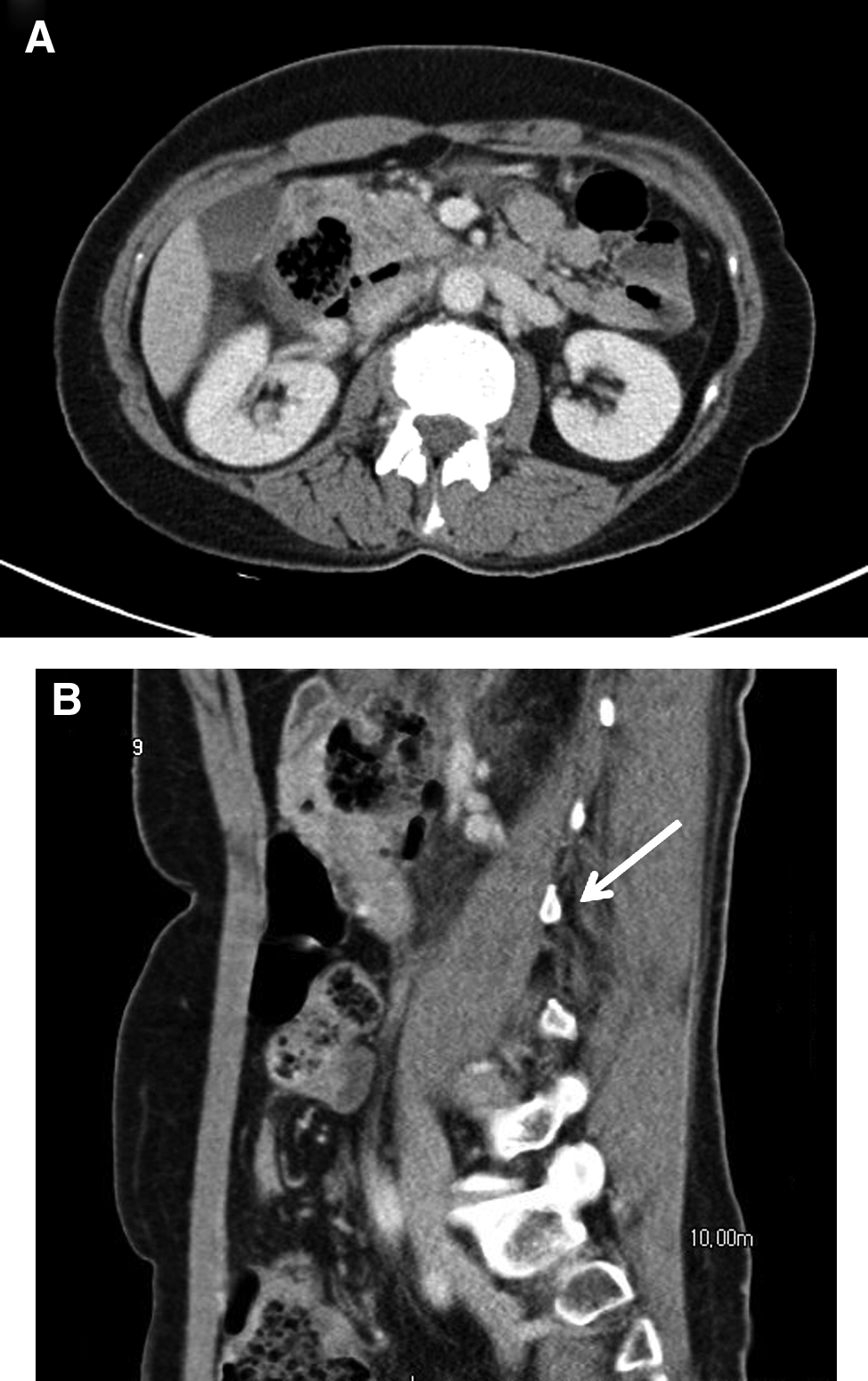
The laboratory findings were normal, except for an elevated white blood cell count (12.9 × 109 L−1). Chest and abdominal plain X-rays revealed only mild gastric-wall thickening. Computed tomography (CT) showed a 4.4-cm round space including air bubbles and food material in the posterior aspect of the second duodenal portion. Air collection and inflammatory changes were observed around the round space, and a small amount fluid had collected in the right pararenal space. A gallstone was discovered within the gallbladder (Fig. 1).
Under general anesthesia, with the patient in the supine, reverse Trendelenburg position, she underwent an emergency laparoscopic exploration. No nasogastric tube was inserted. A 10-mm trocar for the camera was inserted under the umbilicus using an open technique. After intra-abdominal insufflation with CO2, the pressure was kept at 12 mm Hg, and three working trocars were inserted. A 12-mm trocar was inserted in the right midclavicular line 2 cm above the level of the umbilicus. Two 5-mm trocars were inserted in the left midclavicular line, one at 4 cm above the level of umbilicus and the other in the upper abdomen in the right anterior axillary line (Fig. 2).
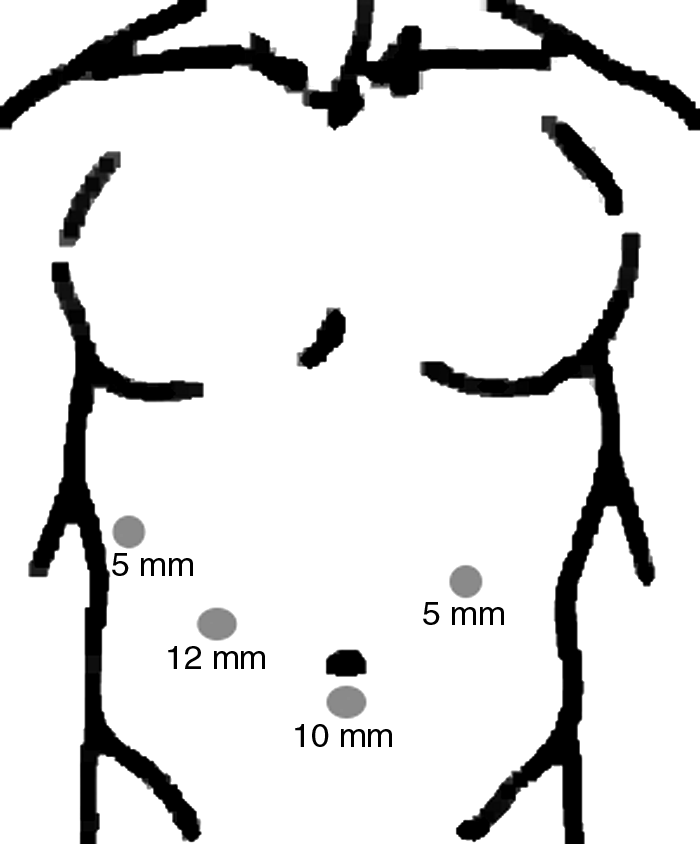
Trocar placement.
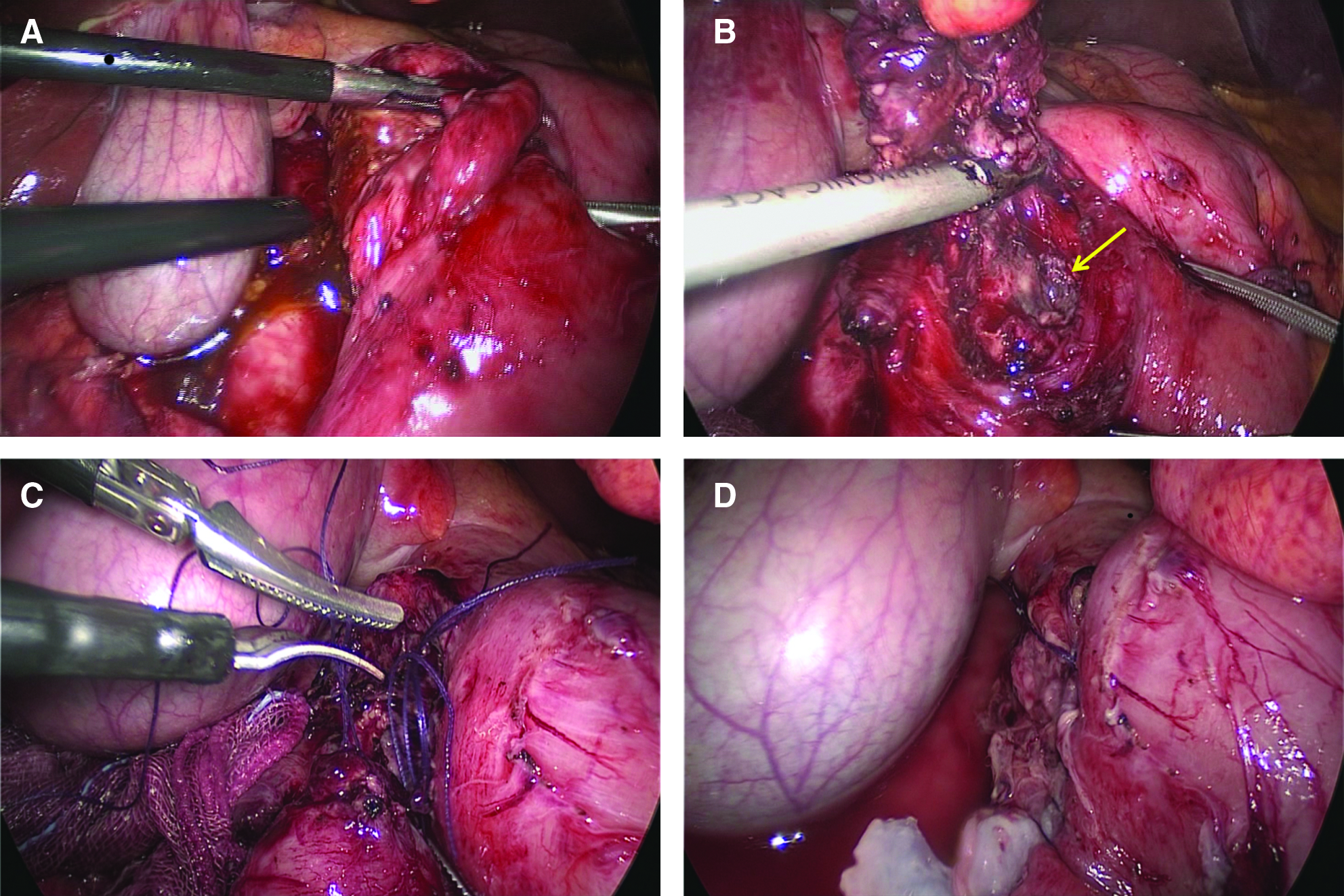
The dissection was begun by dividing the lateral side of the duodenum (Kocher maneuver) with laparoscopic ultrasonic shears (Ethicon Endo-Surgery, Cincinnati, OH). Entering the posterior side of the duodenum, dirty reactive fluid was drained and an ∼4-cm inflamed, perforated diverticulum was found at the posterolateral aspect of the second portion of the duodenum. After completing the peridiverticular dissection toward the neck of the duodenum, a diverticulectomy was performed using ultrasonic shears, and the opening of the diverticulum was closed in two layers with intracorporeal, hand-sewn No. 3-0 Vicryl sutures (Fig. 3). A closed drain was inserted through the 5-mm trocar site in the right anterior axillary line and placed at Morrison's pouch. The operating time was 115 minutes. An upper gastrointestinal series performed on postoperative day 7 showed no abnormality (Fig. 4), and the patient was discharged on postoperative day 10 without complications.

The postoperative upper gastrointestinal series shows no abnormality.
Discussion
Diverticulitis precedes the perforation of a duodenal diverticulum in most cases. 8 Perforations of duodenal diverticula result from various causes such as ulceration, necrosis, enterolithiasis, blunt abdominal trauma, and iatrogenic causes. 9 Perforation triggers acute right upper abdominal or epigastric pain, nausea, and vomiting, but the clinical signs and symptoms may be nonspecific. Perforation typically causes retroperitoneal abscesses, but the diverticulum may also perforate anteriorly or into the pancreas, colon, gallbladder, or aorta, leading to a duodenocolic fistula with steatorrhea or acute gastrointestinal bleeding secondary to perforation into the aorta.10,11
The preoperative diagnosis of a perforated duodenal diverticulum is very difficult because the symptoms usually mimic more common abdominal pathologies, such as a perforated duodenal ulcer, cholecystitis, and pancreatitis. Moreover, plain abdominal radiographs are normal in more than half of perforated duodenal diverticula because of free air in the retroperitoneal space. 8 CT is useful for identifying retroperitoneal air and fluid around the duodenum. 12 It is also helpful for demonstrating a thickened bowel wall, mesenteric fat inflammation, and the diverticulum itself. 7 In our patient, the plain radiograph did not show free air, whereas CT revealed the duodenal diverticulum and retroperitoneal air with fluid collection.
The standard operation involves a stapled or hand-sewn diverticulectomy with two-layer closure of the duodenum, taking care to avoid narrowing the duodenal lumen, with drainage of the retroperitoneal space.1,8,13 In addition, a tongue of the greater omentum can be patched over the closure. It remains controversial whether the addition of a gastric diversion procedure, such as pyloric exclusion and gastrojejunostomy or tube duodenostomy, is necessary to protect the closure. 14 Intraoperatively, in cases with a severely inflamed, friable duodenal wall or retroperitoneal abscess formation, pyloric exclusion can potentially lower the rates of duodenal fistula and suture line leakage over primary closure and drainage alone. 15 Another operative option is a Roux loop duodenojejunostomy, which has several advantages, including a tension-free repair with healthy tissue of jejunum and diversion of the gastric contents via the Roux loop, but the operation takes longer. 16
Open duodenal diverticulotomies have been reported frequently, whereas only a few laparoscopic procedures have been reported.17,18 Further, until now, laparoscopic diverticulectomy for a perforated duodenal diverticulum has not been reported.
To our knowledge, this is the first laparoscopic diverticulectomy performed for a perforated duodenal diverticulum.
Footnotes
Disclosure Statement
No competing financial interests exist.