
Abstract
Abstract
Introduction:
The effect of the choice of access upon endoscope control during a navigational task is explored within a simulator model.
Materials and Methods:
The study was conducted within the endoscopic–laparoscopic interdisciplinary training entity (ELITE) model (Minimally Invasive Therapy and Intervention Research Group [MITI], Technische Universität, Germany)—a validated natural orifice translumenal endoscopic surgery (NOTES) simulator. Seventeen subjects, 15 with no endoscopic experience, navigated the endoscope from predefined trans-sigmoidal and transgastric access points to the appendix and the gallbladder. A previously defined and validated quantitative analysis of endoscope control, in addition to time taken to complete the task, was used to evaluate overall performance. The quantitative analysis extrapolated the movements of the subject's wrist in control of the endoscope and rated the movements using a scoring system of 0–3 based upon the smoothness of the movements recorded.
Results:
Although no significant difference in terms of performance time was demonstrated between the two approaches to the appendix (36.6 ± 14.7 seconds TG and 29.8 ± 16 seconds TS) (P = .214), when the endoscope control score was compared, a significant difference was confirmed (3 TG and 7 TS) (P < .001). With regard to the approach to the gallbladder, a significant difference in terms of both the performance time (19.8 seconds TG and 35.6 seconds TS) (P < .001) and the quality of endoscope control (7 TG and 5 TS) (P = .001) was demonstrated.
Conclusion:
The choice of access route impacts directly on the ease with which the endoscopist navigates to the target. Within this study, the trans-sigmoidal appears the most appropriate to access the appendix and the transgastric for the gallbladder.
Introduction
One of the greatest assets of the endoscope is its flexibility, enabling it to access body cavities from points not otherwise considered feasible with rigid instruments offering a potential platform for NOTES. However, this flexibility, which is highly effective for intralumenal exploration, might also be an overwhelming drawback of the NOTES technique. 2 To navigate from the translumenal access point to the target organ, the endoscope needs to be manipulated within the three-dimensional spatial environment of the peritoneal cavity posing significant difficulty.
Many factors govern the choice of access route for NOTES, and this decision is predominantly dominated by the ability to ensure safe entry and secure closure of the translumenal breach. In light of this, the transvaginal route, having been extensively used by gynecologists for many years, has dominated early NOTES trials. 3 The alternative transgastric, transcolonic, and transvesical approaches have all been successfully trialed both in animals and, for the most, in humans.4–6 The transgastric approach is widely accepted as the alternative to the transvaginal route with the justification of its use subjugated by the ability to sterilize or disinfect the stomach before gastrotomy, thus reducing the bacterial load. However, gastrotomy closure still remains challenging and complex to undertake.
The transcolonic approach has, in general, been overlooked due to the fears surrounding bacterial contamination. Security of closure does expose the same difficulties as found with the transgastric approach, but if the transluminal access point is made in the rectosigmoid, then access and closure can be undertaken using the transanal endoscopic microsurgery (TEMS) technique. This poses a significant advantage over the transgastric approach, as TEMS is already widely available in many hospitals for the full-thickness resection of rectal polyps and early stage rectal cancer. 7 The exploration of utilizing TEMS as a means of developing the NOTES trans-sigmoidal approach in the animal laboratory has led to a defined repeatable, sterile access and closure method termed the innovative safe and sterile sigmoid access technique. 8 With this method, trans-sigmoidal access could be considered a safe NOTES approach and a suitable alternative to the transvaginal for the male patient.
Due to these reasons, the impact that the choice of access point may have on the ease of navigation to the target site may be overlooked, and this decision may profoundly influence the ease of performing the subsequent procedure and potentially as a result enhance safety. It is critical that key decisions with regard to NOTES are made on an evidence base not only for technical aspects such as efficacy of closure devices but also on the ergonomic aspects of the task, ensuring that optimal surgeon performance can be achieved.
The aim of this study was to compare the efficiency of endoscope navigation from the transgastric and trans-sigmoidal access sites to the appendix and gallbladder with the aim of determining which point is the most strategic to use for these procedures. It is hypothesized that a straight endoscopic navigational path will afford improved performance by obviating the necessity for scope retroflexion and the consequent navigational demands. It is thought that a trans-sigmoidal approach will lead to enhanced navigation to the gallbladder and that a transgastric route will improve passage to the appendix. A quantitative multimodal ergonomic evaluation was undertaken to investigate this within the endoscopic–laparoscopic interdisciplinary training entity (ELITE) model, a newly developed and validated NOTES simulator. 9
Materials and Methods
Subjects
Seventeen subjects (14 men and 3 women) were recruited from Imperial College staff and students and from the Department of Surgery, Klinikum rechts der Isar, Technische Universität, Germany. Fifteen subjects were novices with no experience of endoscopy, and two were experts with a combined experience of greater than 10,000 endoluminal cases, included as a means of validating the task. One expert had had previous experience of undertaking NOTES endoscopy within a porcine model although this was on a single occasion only.
The ELITE simulator
The trial was undertaken using the ELITE developed by the research group (Minimally Invasive Therapy and Intervention Research Group [MITI], Technische Universität, Germany) and manufactured by Coburger Lehrmittelanstalt (CLA, Coburg, Germany). The ELITE is a simulator model specifically designed to train clinicians in endoscopic, laparoscopic, and NOTES procedures. The model is a measured accurate reconstruction of the torso of an adult human female complete with various translumenal access routes to the abdominal cavity: transesophageal, transgastric, and trans-sigmoidal. The torso contains a complete organ package, including liver, gallbladder, appendix, spleen, and a full gastrointestinal tract with attached mesentery and omentum. The intestine is gas tight with valves at each of the proximal access points to enable successful insufflation. In addition, the model is supported by a fixed and expandable anterior abdominal wall to enable a realistic pneumoperitoneum to be established if required (Fig. 1). ELITE has been fully validated as a NOTES training system with the skills established on the model being fully translatable into clinical practice. 9
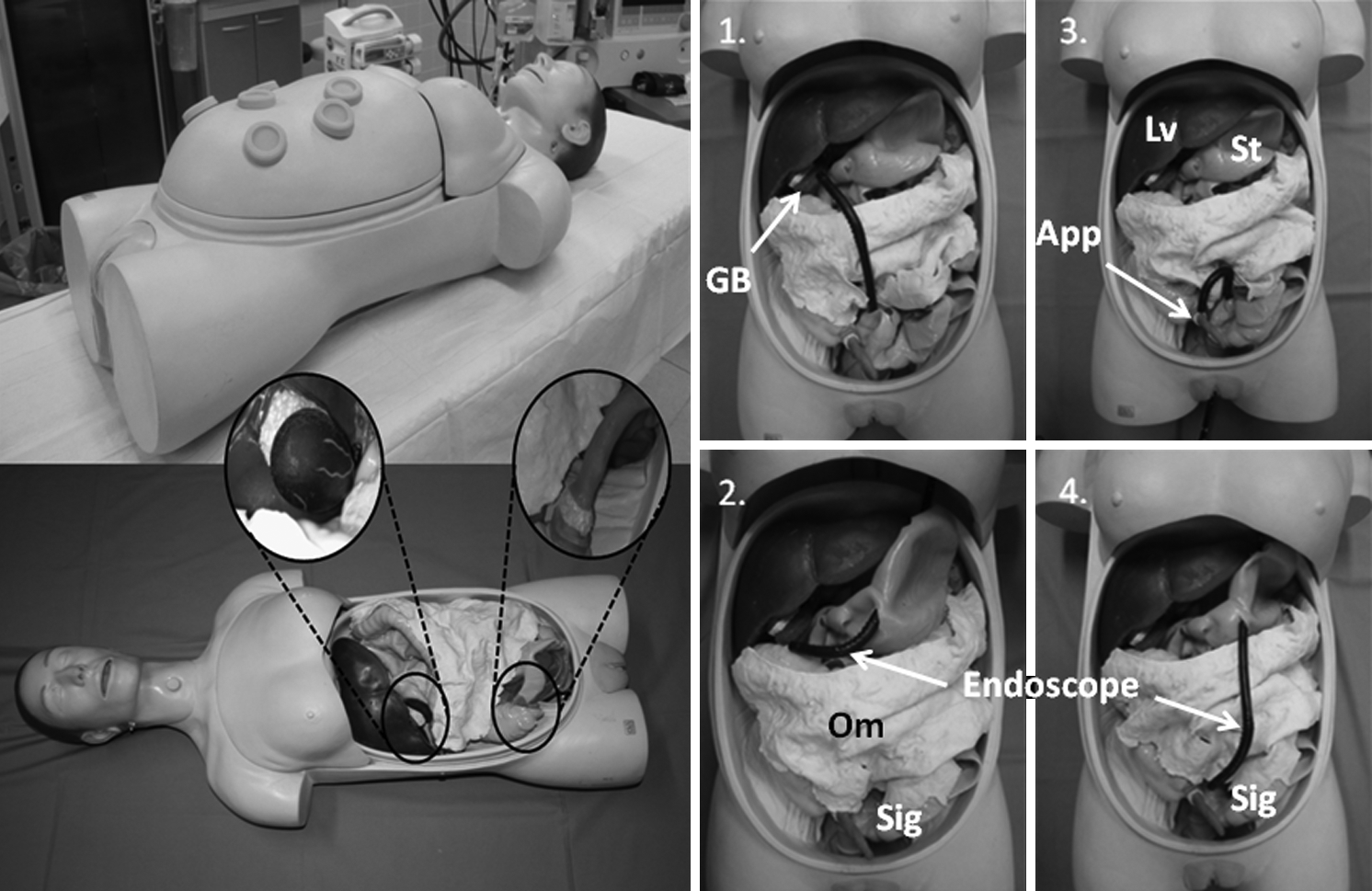
The endoscopic–laparoscopic interdisciplinary training entity (ELITE) simulator demonstrated with the four endoscopic navigation paths explored and the target organs (inset) as viewed from the endoscope.
The navigational task
The task involved navigating a 10.6-mm single-channeled sigmoidoscope (Karl Storz Endoskope, Tuttlingen, Germany) to both the gallbladder and the appendix using either the transgastric or trans-sigmoidal approach. To have standardized conditions, the transluminal breaches were predefined in the rectosigmoid and the greater curvature of the stomach for access. The navigation trial began from each of the relevant gastrointestinal transluminal access points to the required organ (Fig. 1). The endoluminal portion of each access route was not included. Each subject navigated to each organ (gallbladder and appendix) via each access route three times. The order in which the subject performed the navigational tasks in terms of the access route and target organ was randomized. The maximum task time required by the subject to reach the desired target was defined 60 seconds. The task was completed when the target organ had reached a specified size on the screen, equivalent to 2 cm from endoscope to target organ, which had been predefined with markers around the screen edge. The point at which the size had been met was agreed by two independent adjudicators. Once the target was reached or alternatively 60 seconds had passed, the endoscope was withdrawn to the translumenal access point within the simulator by one of the independent adjudicators and the scope re-orientated for the next run. The subject was blinded to the internal anatomy and position of the endoscope from the previous run by a screen while the endoscope was being retracted to its starting position.
Quantitative evaluation of endoscopic skill
Outcome metrics included time and a score derived from the quality of the users torque control of the endoscope during each navigation task. This score was measured using an inhouse-developed and -validated tool derived from tracking the movements of the wrist, which is controlling the shaft of the endoscope. 10
A video motion-tracking camera (Optotrak Certus, NDI) was used to track the movements of optical markers attached to the wrist of the subject to determine linear and rotational movement and therefore torque control of the endoscope. Each movement recorded by the motion tracker was sequenced through the position of the markers in three-dimensional space and compared against a template of previously defined movements to enable classification into either forward or backward linear motion and left or right rotation. For each individual subject and for each task, the movements recorded were summarized into a pattern of movement behavior over the trial time (Fig. 2).

Examples of the different patterns of movement extrapolated from the tracking of the endoscopist's wrist (
Determined by the pattern of behavior, a score of 3 was allocated to those demonstrating a purposeful precise movement to reach the target and a score of 1 when the pattern was repetitive and erratic. Each subject performed each of the navigation paths three times and as such a maximum allocated score of 9 is achievable for each of the routes. A score of 0 was assigned when the subject failed to reach the desired targets within the designated time irrelevant of the quantitative evaluation outcome.
The overall relationship of the defined movements and therefore the patterns produced were classified using an automated pattern recognition system validated against a blinded manual assessment, as being purposeful, unskilled, or random. The system had been previously defined and validated as a suitable assessment technique. 10
Previous trials have demonstrated that the movement of the wrist during navigation of a flexible endoscope within a NOTES environment and the subsequent quantitative evaluation correlates with endoscopic skill (r = 0.874) and therefore the quality of endoscopic control. 10 However, in this trial the assigned score is used as a method of delineating the more challenging navigational path in terms of endoscope control with each subject acting as their own control in terms of skill level.
Results
All 17 subjects completed the whole trial. Two hundred and four individual navigation trials (51 per course) were undertaken with an equal distribution in terms of the approach and the target organ. The order in which the trials were undertaken was randomized. No significant improvement in either the performance time or the endoscopic control score could be confirmed whether the navigational paths were randomized to the beginning or the end of the entire trial.
The overall mean time to complete all 12 trials for all subjects was 30.4 ± 7.7 seconds with a median endoscope control score of 6 (range 0–9). Raw values are highlighted in Table 1. A significant difference in terms of performance time (P < .001) and endoscope control (P = .002) was demonstrated between the experts (time 16.2 ± 12.3 seconds and median score 7 [range 2–9]) and novices (time 28.5 ± 6.6 seconds and median score 6 [range 0–9]). Overall, 41 targets (20%) were not reached within the set time frame. Fourteen occurred when attempting to reach the appendix transgastrically (TGApp) and 9 from the trans-sigmoidal approach (TSApp), with 6 missed while approaching the gallbladder from the transgastric access (TGGB) and 12 the trans-sigmoidal (TSGB).
Experts highlighted in bold.
Although no significant difference in terms of performance time was demonstrated between the two approaches to the appendix (36.6 ± 14.7 seconds TG and 29.8 ± 16 seconds TS) (P = .214), when the endoscope control score was compared, a significant difference was confirmed (3 TG and 7 TS) (P < .001) (Fig. 3a). With regard to the approach to the gallbladder, a significant difference in terms of both the performance time (19.8 seconds TG and 35.6 seconds TS) (P < .001) and the quality of endoscope control (7 TG and 5 TS) (P = .001) was demonstrated (Fig. 3b).

Performance results for navigating to the appendix
Discussion
The question of the adequate access and safe navigational path through the abdominal cavity to reach any organ still remains unclear. In this study, the impact of translumenal breach site on navigation to the gallbladder and appendix was assessed. A quantitative assessment of endoscopic torque control alongside task completion time was used as metrics of performance.
It was found that navigation to the gallbladder was enhanced in terms of both task completion time and efficiency of movement when a transgastric approach was employed, compared to the trans-sigmoidal. Navigation to the appendix was better in terms of efficiency of movement when a trans-sigmoidal approach compared to the transgastric; however, there was no difference in task completion time. This leads to the assumption that the various accesses in NOTES have specific advantages and disadvantages, and hypothesizes that the NOTES access route should be chosen according to the intended intervention.
It is possible that navigating out of the pelvis is more challenging and therefore any performance benefit that the trans-sigmoidal route yields is less marked. The local anatomy at the site of the translumenal breach may also influence subsequent navigation. The approach through the rectosigmoid affords less mobility than the access through the greater curvature of the stomach, and therefore endoscopic movement is likely to be restricted at this point. One of the limitations that may have influenced the outcome is that the simulator is modeled on a patient lying flat and not as would be the case for pelvic NOTES approaches, in the Lithotomy position, which would flatten the pelvis reducing the impact of the pelvic angle on the navigation.
A further limitation to the study reflects the lack of consideration given to the final orientation of the endoscope view at the target site. It is well documented that approaching the gallbladder from the transgastric site causes disorientation with the view inverted, which in itself challenges the safety of undertaking an operation, an aspect that would impact significantly on the decision as to the most appropriate access route for this procedure but as to whether this is seen for the appendix from the trans-sigmoidal approach was not assessed.
To encourage expansion of the technique, it is essential that more clinicians become exposed to the approach and are trained in the technique to develop and explore its full potential within their own surgical specialty. Developing formal training and assessment methods for NOTES will become essential to the continual expansion of the technique. As such training models may play a crucial role in this area in the future, particularly as simulator training is becoming more common place in surgical education. Only few analog and no virtual training model for NOTES have been evaluated yet. We chose one of the validated analog NOTES training model for our trial.
The ELITE simulator has full construct validation as a training module for NOTES with the skills acquired on the simulator fully transferable into the animal model. Also, in this trial experts could reliably distinguished from novices. A significant learning curve of the subjects of the three consecutive courses could not be demonstrated. This may result from the extremely short total task time. However, assessment of the endoscopic control remains challenging. Assessment during endoluminal endoscopy currently involves a subjective score specific for each endoscopic investigation 11 and therefore not appropriate for use in NOTES. An objective method of assessing torque control will therefore be invaluable in the training of future NOTES clinicians. However, as has been seen with this trial, the combined use of these training and assessment tools has the potential not only to be used within the remit of surgical education but also to expose the subtle nuances of the technique, particularly where endoscope control is important.
Natural orifice surgery remains an exciting area of development for the future of surgical practice. The enticement of no scars, less postoperative pain, fewer adhesions, and fewer chronic complications is compelling particularly when the overall impact of surgery on the patient should be minimized as a result. However, it is difficult to conceive that the technique will ever take over completely from conventional laparoscopic surgery or even, in some cases, the open approach, but it is far from inconceivable that it will find its place either as an adjunct to current surgical practice or as an alternative for procedures yet fully defined such as percutaneous endoscopic gastrostomy retrieval, the transgastric necrosectomy and drainage of pancreatic necrosis or cysts in pancreatitis, the placement of diaphragmatic pacing wires for weaning intractable patients off ventilators, 12 or, as some have predicted, bariatric surgery.
Currently, there is already a definite expansion of single-incision surgery into the realms of the natural orifice approach with the use of long semirigid instruments performing the dissection with the use of the endoscope for observation all through the vagina, 13 presenting a bridge between the two techniques. However, the challenges surrounding the endoscope in terms of its use as a single operating system without assistance from rigid or semirigid instruments are still some way off.
In terms of flexible endoscopic NOTES, navigation to designated target organs may be more efficient and less challenging to undertake from alternative translumenal access points promoting efficiency as well as safety. The choice of which route should depend on sound ergonomic evidence. As security and safety of the trans-sigmoidal approach improves, this access route may demonstrate significant benefits in terms of endoscopic navigation over the alternative routes and should not be disregarded as a suitable pelvic alternative to the transvaginal route in the male patient.
Conclusion
This study shows that navigation to the gallbladder was enhanced in terms of both task completion time and efficiency of endoscope control via a transgastric approach, whereas navigation to the appendix was better in terms of efficiency of control via the trans-sigmoidal route, despite there being no difference in task completion time. This underlines the consideration that the various access routes in NOTES offer specific advantages and disadvantages in terms of ergonomic simplicity of endoscope navigation for the user determined by the target organ under consideration. As such the choice of which would be the most appropriate should consider not only the safety and security of the route in question but also, additionally, the strategic advantage.
Footnotes
Disclosure Statement
No competing financial interests exist.