
Abstract
Abstract
Background:
Angelchik is a silicone gel-filled prosthesis that was historically placed around the gastro-esophageal junction like a horse's halter for the treatment of gastro-esophageal reflux disease. It was first described by Angelchik and Cohen in 1979, after which its usage expanded due to its simplicity and ease of insertion by open surgery. However, the use of this device has largely been abandoned due to numerous complications and a consequent high removal rate. The most common complications cited have been dysphagia, disruption, migration, and erosion into the stomach. Although many reports of Angelchik prosthesis removal have appeared in the literature, we present a case of laparoscopic removal of this device that has been inserted 25 years ago, followed immediately by Nissen fundoplication. The main indication for operation was recurrent severe reflux symptoms refractory to medical treatment.
Methods:
Case note review and literature search.
Results:
There was no intraoperative or postoperative complication although the procedure was extremely challenging laparoscopically primarily due to attenuated anatomy and dense adhesions. The patient made an uneventful recovery with subsequent complete resolution of symptoms.
Conclusion:
Patients who have severe recurrent gastro-esophageal reflux disease symptoms refractory to medical treatment after placement of an Angelchik prosthesis can be treated by laparoscopic removal of the device followed by Nissen fundoplication.
Introduction
Case Report
A 54-year-old lady presented with severe recurrent GORD despite being on maximal doses of proton pump inhibitors. Her main complaints were heartburn and regurgitation. Previously she had an Angelchik prosthesis inserted by open surgery in 1985. Unfortunately, after remaining well for several years, her symptoms recurred 10 years ago and progressively got worsened. She was willing to go ahead for the second anti-reflux operation despite that it would be difficult and high risk. Her other medical history included total abdominal hysterectomy and bilateral salpingoophrectomy. She had no co-morbidity.
Severe GORD was confirmed on 24-hour pH monitoring that showed DeMeester score of 26.3 and fraction time pH < 4 = 4.6. She has had total of 105 refluxes in 22 hours and 63 of them had pH < 4. Two of the refluxes were of >5 minute duration and the longest reflux was of 21 minute duration. Her reported symptoms correlated with the reflux. Esophageal manometry showed hypotensive lower esophageal sphincter (mean resting pressure of 2.7 mm Hg) with normal relaxation. Gastroscopy revealed mild gastritis. Biopsy of lower part of esophagus showed chronic reflux gastritis. Her computed axial tomography scan showed an unmigrated 6.5 cm doughnut-ring-shaped Angelchik prosthesis with radiopaque outer margins encircling GOJ (Fig. 1). At operation the Angelchik ring was dissected free from the proximal stomach, diaphragm, and liver after extensive adhesiolysis. The fibrous pseudocapsule enclosing the ring was divided. The anteriorly tied Dacron straps were untied and the prosthesis was removed intact from around the esophagus after identifying and dissecting the cruras and esophagus (Figs. 2 and 3). After this, Nissen fundoplication with a 360-degree wrap was carried out (Fig. 4). There were no intraoperative and postoperative complications. Oral intake was commenced on the first postoperative day and the patient was discharged home after normal dietary intake was established on third postoperative day. There was complete resolution of symptoms at 4-week follow-up.
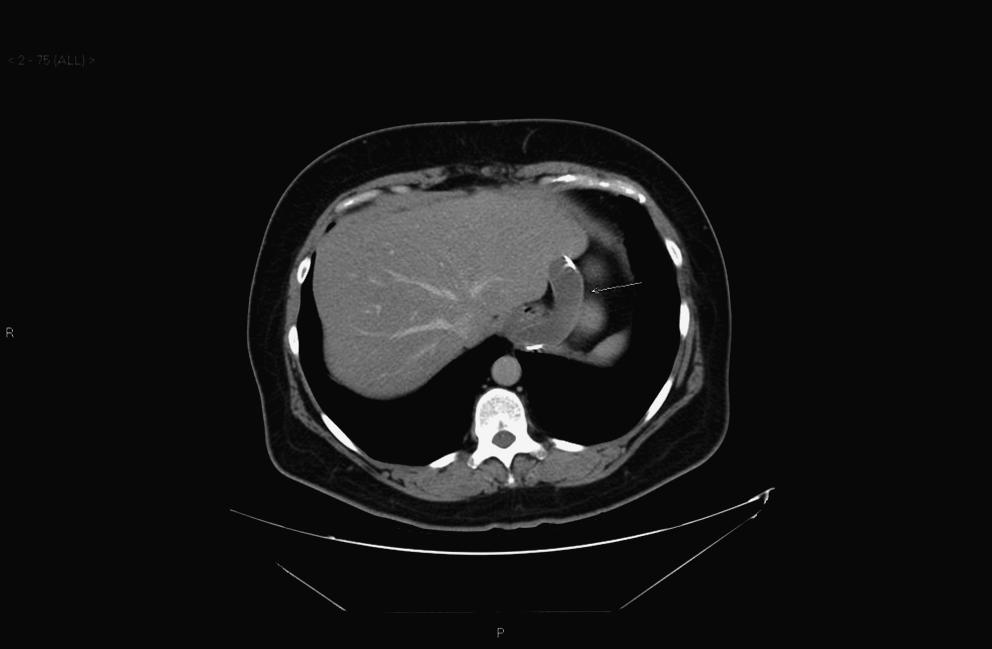
Computed tomography scan with Angelchik prosthesis in place.
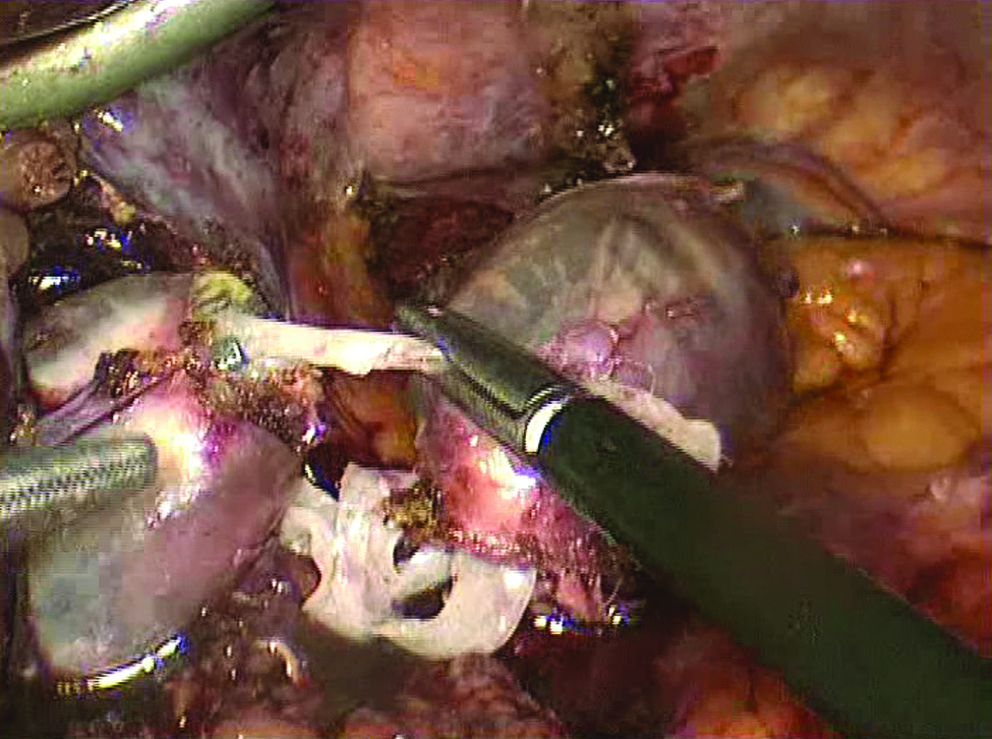
Angelchik prosthesis encircling gastro-esophageal junction.

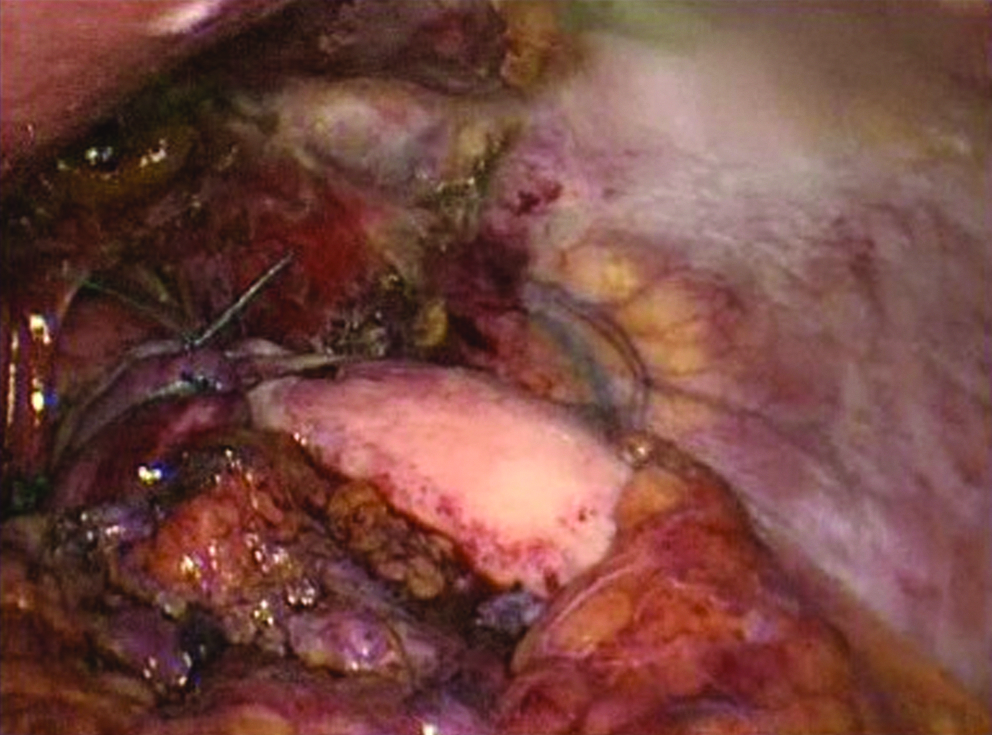
Intact Angelchik ring with pseudocapsule after surgical removal.
360-degree Nissen fundoplication.
Discussion
Angelchik prosthesis received premarket approval by the Food and Drug Administration's Bureau of Medical Devices in 1979. With time, its usage expanded, despite the absence of randomized controlled trials establishing the device's efficacy and safety. By 1989, >25,000 prostheses had been inserted worldwide but only 56 in the context of prospective randomized controlled trials (Table 1).
An early trial by Gear et al. in 1984 concluded that 96% of those receiving an Angelchik device achieved Visick grade 1 or 2 compared with 81% of those undergoing fundoplication. 6 About 38% of patients suffered early dysphagia, but resolution occurred in all but two within a few months.
Hill et al. 7 found that both Angelchik prosthesis and fundoplication treatment options provided lasting control of gastro-esophageal reflux, but complications, particularly dysphagia, led to removal of the device in up to10% of patients. 5 In this trial 17 of the 30 patients randomized to receive Angelchik prosthesis suffered transient dysphagia. There was absence of prosthesis-related complications beyond 12 months of prosthesis placement.
Another similar trial was analyzed early, and subsequently discontinued because of a subjective impression that the prosthesis group had a worse outcome than the fundoplication patients. 8
A consecutive series of 119 patients receiving Angelchik prosthesis showed good or excellent control of reflux with correctly positioned prosthesis in 85% of cases. (mean follow-up, 39 months). Troublesome dysphagia (Visick grade 3 or 4) was experienced in eight of the 119 patients. 9
There are a few long-term follow-up reports of Angelchik prosthesis, but all of them have suggested that in a significant number of patients the prosthesis either failed to control symptoms or itself lead to problems. Gastro-esophageal reflux is known to be a major risk factor in the development of Barrett's metaplasia and adenocarcinoma of the GOJ. Mercer et al. 10 described three cases of adenocarcinoma of the GOJ occurring in patients with Angelchik prosthesis.
Hitherto, the longest follow-up study in the literature is comprised of 65 patients with a follow-up of 145 months and it has shown poor long-term results with only 66% attaining Visick 1 and 2 grade. This study showed a prosthesis removal rate of 15%, mainly due to migration. About 12% and 17% had transient and persistent dysphagia, respectively. 11
Another long-term follow-up study of 46 patients found that 24% had prosthesis removed, all but one for intractable dysphagia. The interval between insertion and removal of prosthesis ranged between 1 and 109 months, with nearly half of the devices removed after 5 years. This study also found that 20 of 26 patients with prosthesis in situ had dysphagia and concluded that the Angelchik prosthesis caused long-term dysphagia in a high proportion of patients. 12
In addition, several case reports have been published highlighting the removal of Angelchik prosthesis by conventional open surgery primarily for dysphagia, disruption, migration, and erosion into the stomach.13,14
We report the successful case description of laparoscopic removal of an unmigrated Angelchik prosthesis followed by Nissen fundoplication for severe recurrent GORD. At operation the device was found to be enclosed in a fibrous pseudocapsule densely adherent to proximal stomach, diaphragm, and the liver. The prosthesis was removed intact from around the esophagus. There was minimal blood loss and no intraoperative and postoperative complications. Recovery was uneventful with complete resolution of symptoms at 4-week follow-up.
This review suggests that although the short-term control of reflux by the prosthesis is comparable to that achieved by Nissen fundoplication, in long term, the prosthesis fails to control the symptoms as in our case. Dysphagia has proved to be the principal cause of poor results with the Angelchik prosthesis. Owing to short-term anti-reflux efficacy and relative ease of performance of the operation, it may be useful for the reflux control in elderly patients at high surgical risk and in obese patients.
This case suggests that laparoscopic removal of Angelchik prosthetic rings is feasible for surgeons familiar with advanced procedures of the esophageal hiatus and should be considered for patients with recurrent reflux especially if their symptoms are refractory to medical therapy.
Footnotes
Disclosure Statement
No competing financial interests exist.