
Abstract
Abstract
Background:
Cyst excision with hepaticojejunostomy is the treatment of choice for choledochal cyst. However, late complications after definitive surgery develop occasionally, including intrahepatic stones and cholangitis, because of bile stasis resulting from anastomotic stricture, intrahepatic bile duct stricture, and remnants of intrahepatic ductal dilatation. In type IV-A choledochal cysts in particular, biliary stricture is frequently observed around the hepatic hilum, and ductoplasty for stricture is necessary. In this article, we present our experiences with totally laparoscopic surgery comprising excision of the extrahepatic bile duct, Roux-en-Y jejunojejunostomy, and wide hepaticojejunostomy combined with hilar ductoplasty for choledochal cyst.
Methods:
We performed totally laparoscopic surgery on 8 children with choledochal cyst between June 2009 and October 2010. One of them had undergone bile drainage through gallbladder laparoscopically for biliary perforation. Four patients (1 Ic and 3 IV-A cysts) had hepatic duct stricture around the hepatic hilum. Laparoscopic surgery comprising excision of the extrahepatic bile duct and wide Roux-en-Y hepaticojejunostomy with ductoplasty was performed by using four trocars.
Results:
The operation was completed laparoscopically for all patients. The mean operation time was 390 minutes (range, 310–460). The mean postoperative stay was 8.4 days (range, 7–14). After surgery, the dilatation of the intrahepatic bile duct was remarkably reduced in size, and all patients are doing well.
Conclusion:
Laparoscopic surgery comprising excision of the extrahepatic bile duct, Roux-en-Y limb formation, and wide hepaticojejunostomy with hilar ductoplasty appears to be feasible for children with choledochal cyst. When there is a stricture near the confluence of the hepatic ducts, laparoscopic ductoplasty appears to be feasible for the surgeon with an advanced laparoscopic skill set.
Introduction
Recently, laparoscopic management for choledochal cyst has been reported with increasing frequency.8–16 However, most reports on laparoscopic surgery for choledochal cyst have not clearly described the management of bile duct stricture, and the Roux-en-Y jejunal limb is usually created extracorporeally in children. In this article, we present our experiences with totally laparoscopic surgery comprising excision of the extrahepatic bile duct, Roux-en-Y jejunojejunostomy, and wide hepaticojejunostomy combined with hilar ductoplasty for choledochal cysts with hilar bile duct stricture, and discuss the technical points.
Patients and Methods
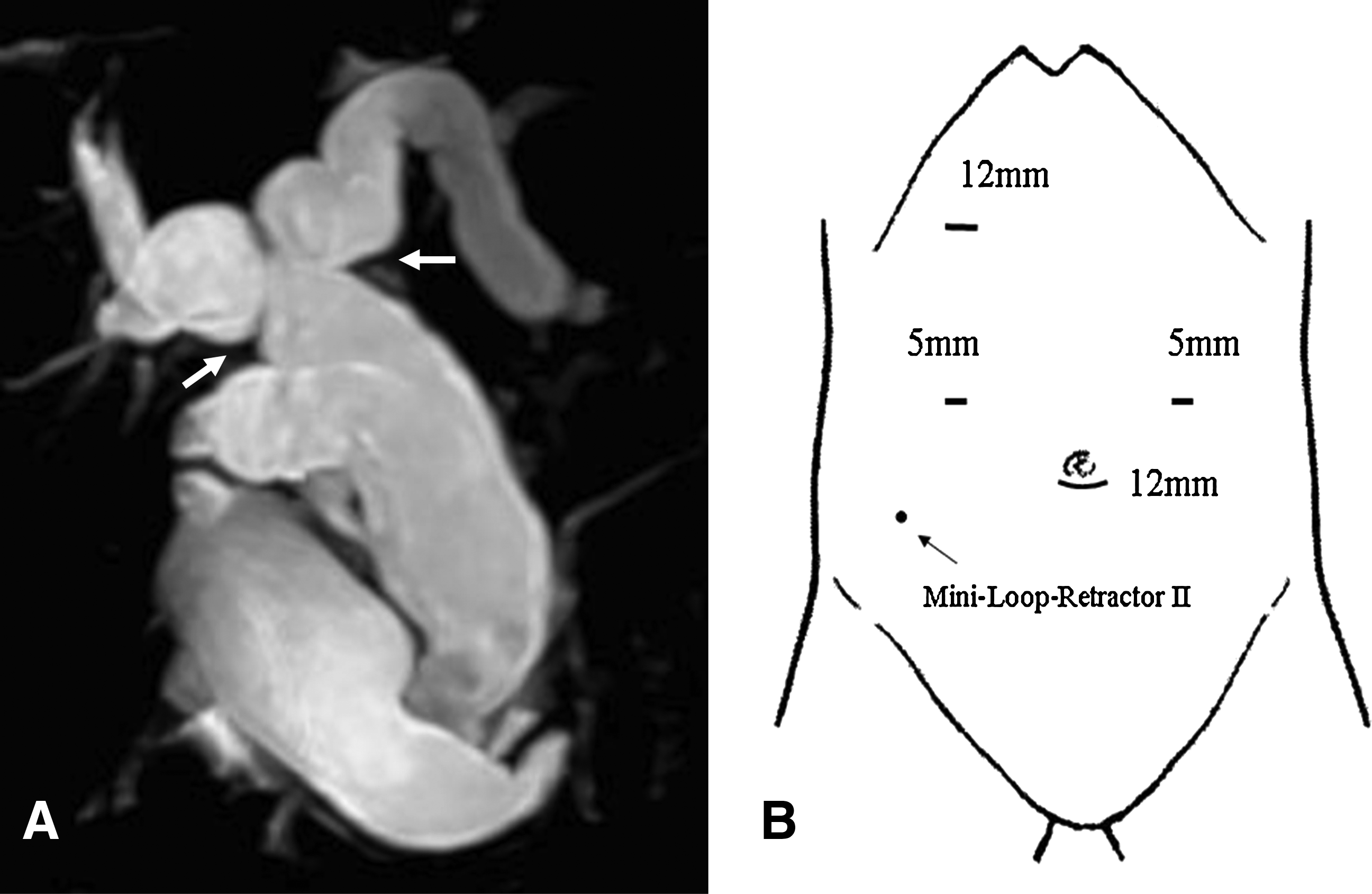
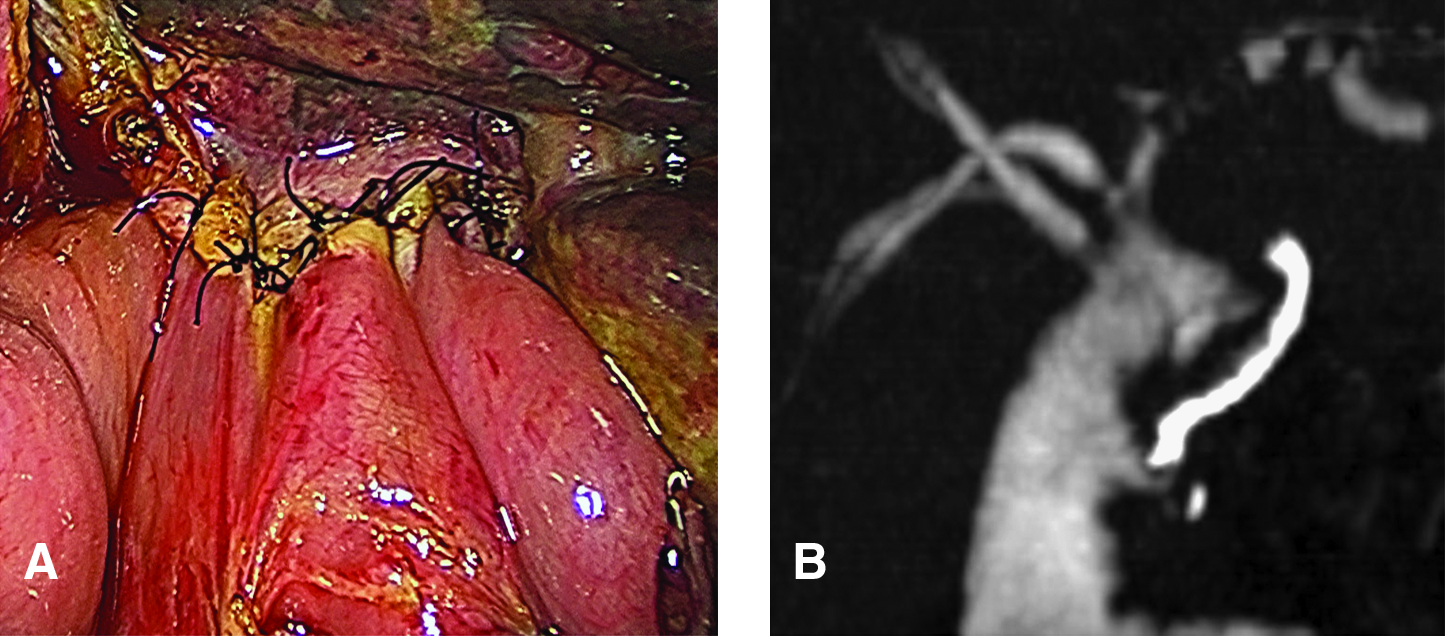
Between June 2009 and October 2010, we performed totally laparoscopic surgery on 8 children (1 boy and 7 girls) with choledochal cyst, at Shizuoka Children's Hospital. The median age was 4.1 years (range, 19 months–7 years). All patients had abdominal pain with hyperamylasemia; 1 had had jaundice. A two-year-old girl had biliary perforation, and peritoneal drainage and bile drainage through the gallbladder were performed laparoscopically on the day of admission. She underwent laparoscopic cyst excision at 14 days after the bile drainage. Preoperatively, ultrasound, magnetic resonance cholangiopancreaticography, and thin-section spiral computed tomography (CT) were performed to clarify the type of bile duct dilatation and pancreatobiliary malunion. All patients had a dilatation of the extrahepatic duct associated with pancreatobiliary malunion. Three patients had intrahepatic ductal dilatation. According to Todani's classification, there were two type Ia (cystic), three type Ic (fusiform), and three type IV-A cysts, respectively. One patient with Ic cyst had the right hepatic duct stricture, and 3 patients with IV-A cyst had the bilateral hepatic stricture (Fig. 1A). In 2 cases, the right hepatic artery ran anterior of the dilated common hepatic duct. After the attack was settled, all patients underwent totally laparoscopic surgery comprising excision of the extrahepatic bile duct, Roux-en-Y limb formation, and wide hepaticojejunostomy combined with hilar ductoplasty for bile duct stricture. CT-intravenous cholangiography at 6–10 days after surgery was performed to evaluate the intrahepatic duct.
Surgical technique
Under general anesthesia, the patient was placed in a frog-leg position. A 12 mm trocar for a 30° 10 mm telescope was inserted through an infraumbilical incision by using an open technique, and pneumoperitoneum of 10–12 mmHg was established. Three additional ports were placed: one 12 mm right subcostal port for cholangiography and assistance, and two 5 mm ports to the right and left upper quadrants for 3 and 5 mm instruments (Fig. 1B).
First, intraoperative cholangiography was performed after exteriorization of the gallbladder via the right subcostal trocar incision. In 1 case, protein plugs were observed in the dilatated common channel, and these were washed out from the common channel by saline irrigation via a catheter inserted through the gallbladder. The gallbladder was then returned to the abdomen after cholecystotomy for the cholangiogram was suture ligated, and pneumoperitoneum was reestablished. The fundus of the gallbladder was grasped by the loop wire of a Mini-Loop-Retractor II (Covidien), which was inserted from the right lower quadrant, and retracted cephalad to expose the hepatic hilum. When necessary, the round ligament was sutured and lifted to the abdominal wall. The Kocher maneuver was performed, and bile duct dissection was started along the supraduodenal margin by using ultrasonic shears (Covidien), bipolar bovies, and a monopolar hook. The choledochal cyst was circumferentially dissected from the hepatic artery and the portal vein. The distal bile duct was then dissected carefully into the pancreas by traction of the cyst until the narrow part of the common bile duct was clearly identified. At this point, dissection was performed by using the bipolar bovies to scrape pancreatic tissue away from the bile duct wall. This distal duct was ligated with 4–0 PDS and divided near the level of the pancreatobiliary junction (Fig. 2A). The proximal stump was also closed with a clip for preventing bile stagnation. The distal stump of the bile duct and the dissected pancreatic surface were covered using the dissected surrounding tissues of the cyst and the posterior duodenal wall by sutures of 4–0 vicryl to prevent bleeding and pancreatic leak (Fig. 2B). Next, the proximal dissection was extended to the hepatic hilum by traction of the divided stump, and the right hepatic artery was separated from the bile duct. In 2 cases, the right hepatic artery was located just anterior of the common hepatic duct, and the bile duct was, therefore, moved anterior of the hepatic artery after amputation of the cystic duct. The proximal bile duct was not divided until the Roux-en-Y limb was made up, to prevent excessive bile stagnation in the abdomen.
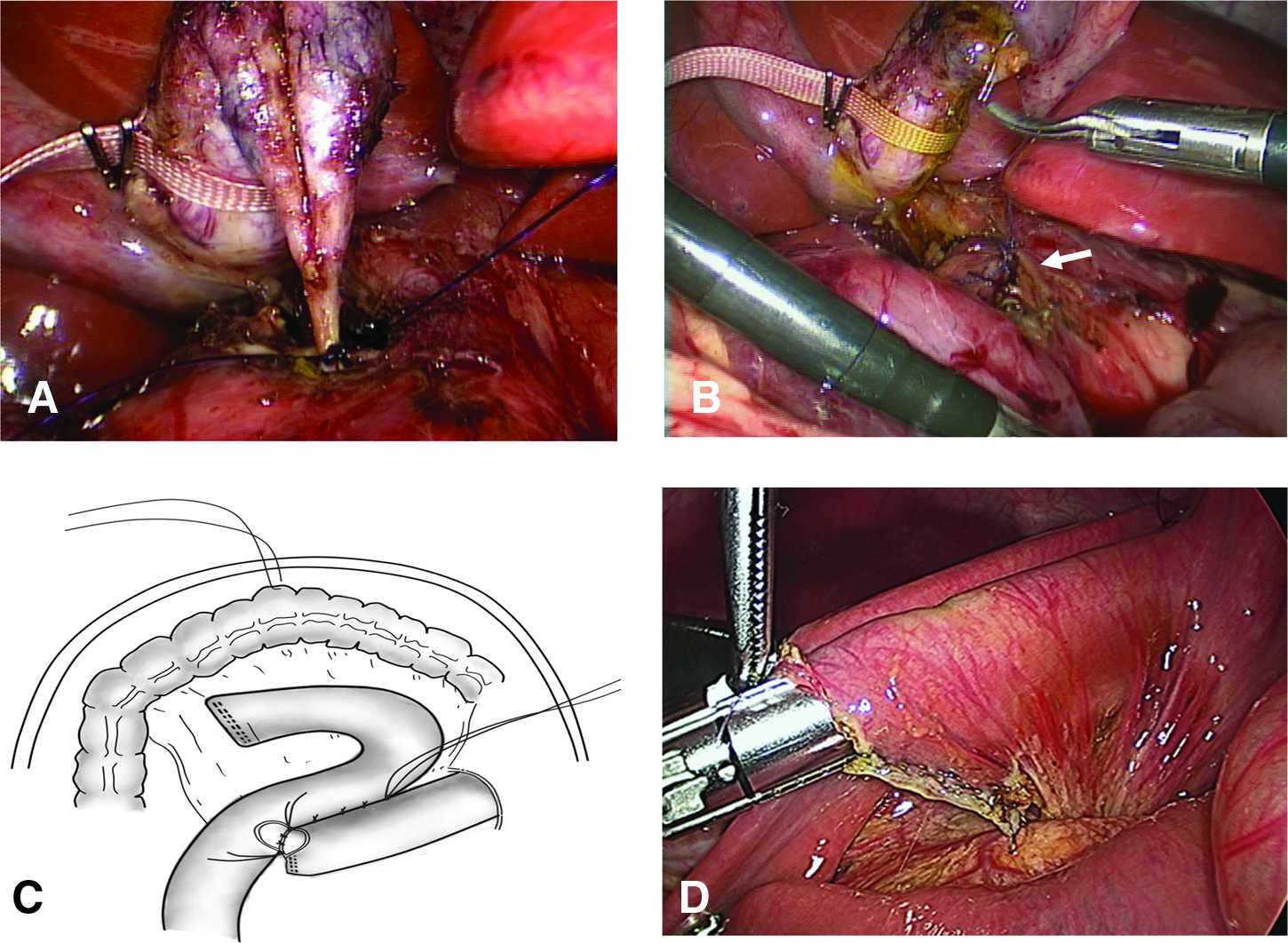
The transverse colon was lifted to the anterior abdominal wall by a percutaneous stay suture, which was passing the abdominal wall, to create a wide working space (Fig. 2C). The Treitz ligament was identified, and the jejunum 20 cm distally was divided by using an Endo-GIA (Covidien). A 20–25 cm Roux-en-Y limb and jejunojejunostomy were created intracorporeally. Stay sutures were placed at both sides of the transected limbs to create traction on the limbs. The stump of the proximal jejunum was excised diagonally so as not to create a blind pouch, and the distal jejunum was minimally incised at the antimesenteric side. After two small enterotomies had been approximated with several sutures, the 45 or 60 mm Endo-GIA was introduced and fired (Fig. 2D). The common enterotomy was closed with Endo-GIA or intracorporeal sutures. During this procedure, there was usually little outflow of intestinal juice to the abdominal cavity. The Roux-en-Y loop was retrocolically pulled up to the hepatic hilum.
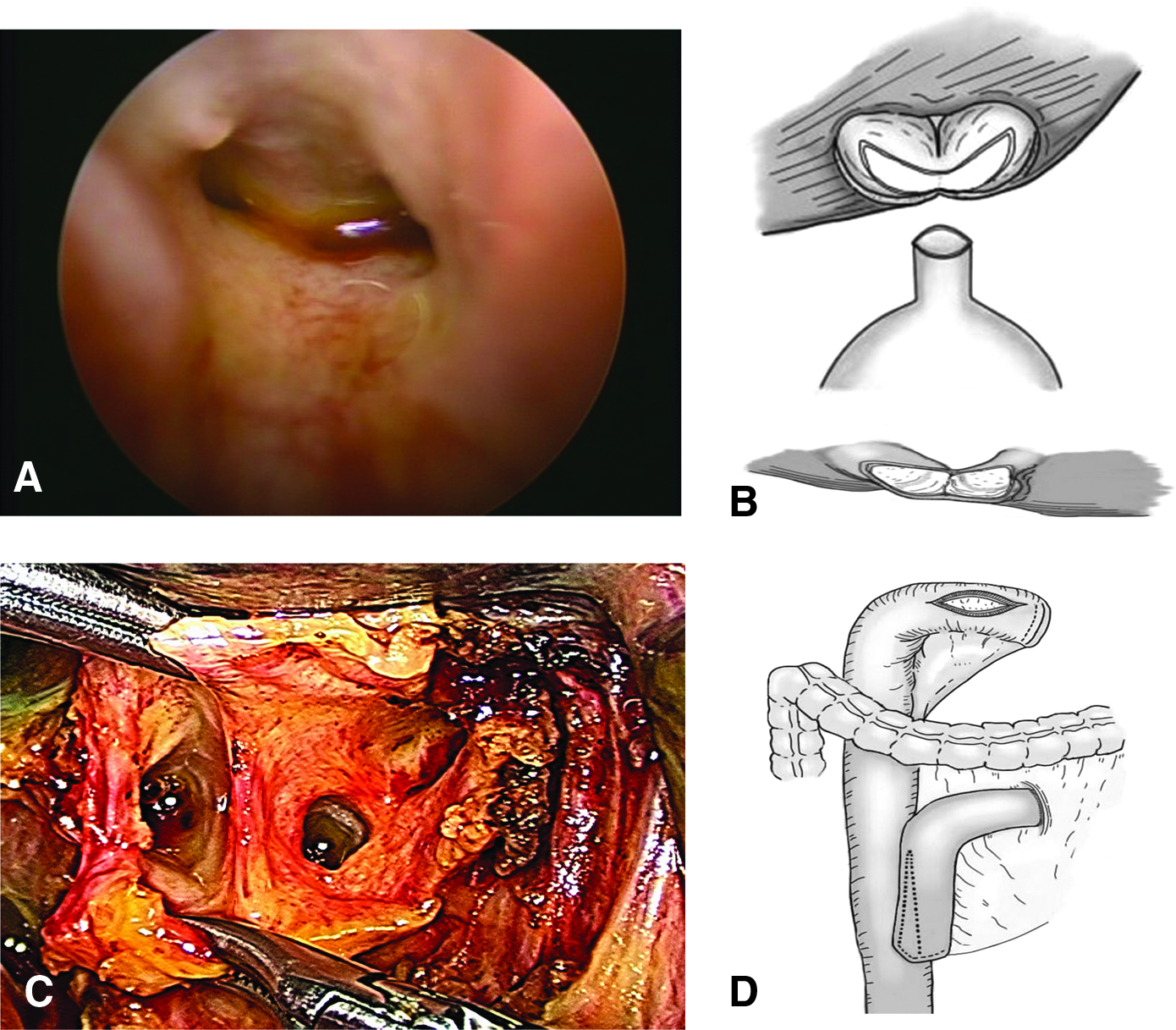
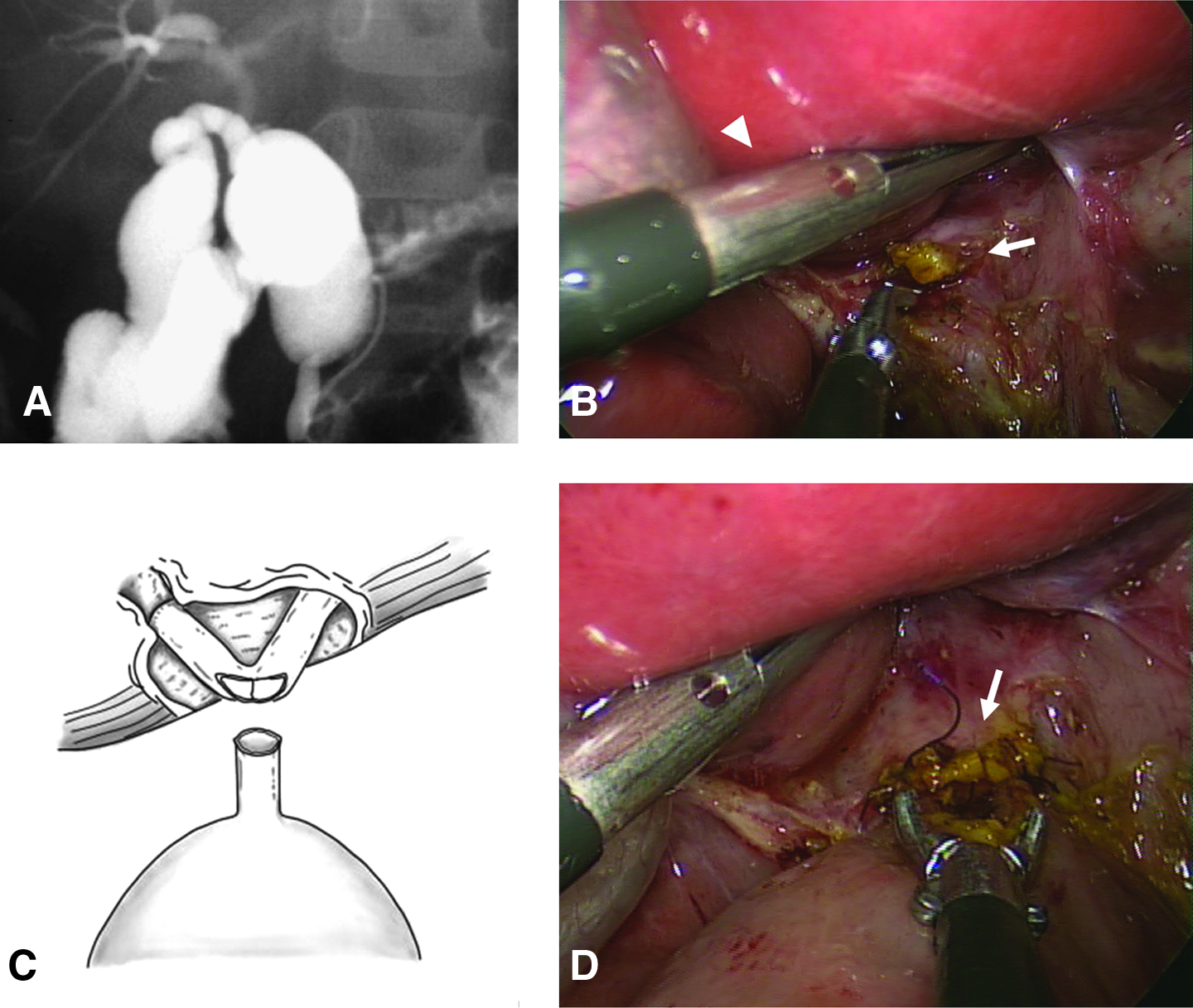
After the creation of the Roux-en-Y limb, the hepatic bile duct was further dissected to the hepatic hilum until the right and left hepatic ducts were exposed, and the common hepatic duct was once divided below the confluence of the hepatic ducts. When necessary, the 3 or 5 mm laparoscope was introduced into the intrahepatic duct through the cut end of the proximal hepatic duct for internal examination. Four patients had a hepatic duct stricture near the confluence of the hepatic ducts (Fig. 3A). In 1 patient with type Ia, the diameter of the common hepatic duct was very small at less than 3 mm, and the laparoscope could not be introduced (Fig. 4A, B). After examination of the proximal hepatic duct, the common hepatic duct was further resected at the confluence of the hepatic ducts, and we made a transverse longitudinal incision along the hepatic duct confluence from the hepatic hilum to the bilateral hepatic bile ducts or a wedge resection of the stenotic segment of the duct by the 3 mm scissors to obtain sufficient bile drainage and large anastomotic stoma (Fig. 3B, C). Bleeding from the ductal wall could be controlled by bipolar bovies and gauze compression. Ductoplasty under the magnified laparoscopic view could be performed more easily than previously thought. After plasty of the hepatic duct, an end-to-side hepaticojejunostomy with large anastomotic stoma was performed at the hilum. An incision a little smaller than the diameter of the hepatic duct was made in the anterior jejunum 1–2 cm distal to the divided end (Fig. 3D). A wide hepaticojejunostomy at the hilum was performed in a single layer by interrupted intracorporeal sutures of 5–0 PDS (Fig. 5A). After hepaticojejunostomy, the defect of the mesentery was repaired with sutures. Finally, the gallbladder was dissected from the liver, and the choledochal cyst and gallbladder were removed en bloc through the right subcostal port. A soft silicone drain was placed near the anastomotic site.
Results
The operation was completed laparoscopically for all 8 patients. The mean operating time was 390 minutes (range, 310–460 minutes). Intraoperative bleeding was minimal. In 1 case, bile leak was observed postoperatively for 5 days, but this then stopped without surgical intervention. The mean postoperative stay was 8.4 days (range, 7–14 days). The mean follow-up was 11.3 months (range, 2–18 months). CT-intravenous cholangiography after surgery revealed that the dilatation of the intrahepatic bile duct was notably reduced in size in all 3 children with type IV-A cyst (Fig. 5B), and all patients are doing well with excellent cosmetic results.
Discussion
Choledochal cyst causes various hepatobiliary and pancreatic disorders, and excision of the extrahepatic bile duct with Roux-en-Y hepaticojejunostomy is the treatment of choice. However, type IV-A cysts occasionally develop intrahepatic stones resulting in cholangitis even after definitive surgery. 1 Intrahepatic stones and cholangitis are mainly due to bile stasis resulting from anastomotic stricture, bile duct stricture, and persistent intrahepatic ductal dilatation.1,2 Todani et al. 1 recommended that wide hepaticoenterostomy be performed for choledochal cyst. Bile duct stricture is frequently observed around the hepatic hilum with a secondary dilatation of the intrahepatic duct, and ductoplasty for ductal stricture is necessary for preventing postoperative intrahepatic stones and cholangitis.1,5–7
In 1995, Farello et al. 8 first described laparoscopic cyst excision and hepaticojejunostomy in a six-year-old child, and reports of laparoscopic management for choledochal cyst are recently increasing in number.9–16 Choledochal cyst is more common in young girls, and laparoscopic surgery provides an attractive form of management with the advantages of cosmetically pleasing results as well as faster recovery compared with conventional laparotomy. However, it requires advanced laparoscopic skills and adequate experience in hepatobiliary surgery. Most reports on laparoscopic management of choledochal cyst have not described bile duct stricture, with only one report of ductoplasty in type IV-A cyst with bile duct stricture, 17 and the Roux-en-Y jejunal limb is usually created extracorporeally in children.
We present here our experience with totally laparoscopic management comprising excision of the extrahepatic duct, Roux-en-Y loop formation, and hilar hepaticojejunostomy combined with ductoplasty for hepatic duct stricture.
In choledochal cyst, a ductal stricture is frequently observed around the hepatic hilum. When there is a stricture near the confluence of the hepatic ducts, laparoscopic ductoplasty appears to be technically possible in experienced hands. We consider that a wide hepaticojejunostomy at the hilum should be performed for choledochal cyst. After surgery, anastomotic stoma would become smaller in size because of inflammation and denuded epithelial mucosa of the bile duct. Moreover, if a hepaticojejunostomy is performed below the confluence, a relative stenosis would occur in type IV-A, in particular. In the cases described here, after examination of the proximal hepatic duct, the common hepatic duct was resected at the confluence of the hepatic ducts, and we made a transverse longitudinal incision along the hepatic duct confluence from the hepatic hilum to both hepatic ducts or a wedge resection of the stenotic segment of the duct by the 3 mm dissector to allow sufficient bile drainage. Bleeding from the ductal wall could be controlled by bipolar bovies and gauze compression comparatively easily. After surgery, intrahepatic ducts were reduced in size in all 3 children with type IV-A cyst. This technique can be used even if the common hepatic duct is extremely narrow, and a large anastomotic stoma can be created (Fig. 4). However, in some cases of type IV-A cyst, laparoscopic ductoplasty may be technically and/or anatomically difficult. When the stricture is located at the more upstream intrahepatic duct, ductoplasty by conventional laparotomy or prophylactic hepatectomy may be necessary.7,18,19
Intracorporeal jejunojejunostomy in the Roux-en-Y limb is usually performed with a blind pouch at the proximal jejunum.15,16 So as not to create a blind pouch, we introduced the Endo-GIA to both enterostomies and fired it as shown in Figure 2D, after the stump of the proximal jejunum had been excised diagonally. Finally, the common enterotomy was closed, and the Roux-en-Y limb with side-to-side jejunojejunostomy was completed without a blind pouch. At this point, a percutaneous stay suture at the transverse colon, which is passing the abdominal wall, is useful to create a wide working space in children (Fig. 2C). This procedure appeared to be easier than previously thought.
Our mean operating time appears to have been much longer than those of other reports. However, ductoplasty for hilar duct stricture is rarely performed, 17 and the Roux-en-Y jejunal limb is usually created extracorporeally. Intraoperative cholangiography and intrahepatic examination are also necessary for accurate depiction of the proximal bile duct anatomy before performing the hepaticojejunostomy. Although further technical refinement may be necessary, intraoperative cholangiography, intracorporeal Roux-en-Y formation, and hilar ductoplasty may have required more time.
Conclusions
Totally laparoscopic management comprising cyst excision, Roux-en-Y jejunal limb formation, and hilar wide hepaticojejunostomy with ductoplasty is obviously less invasive than conventional laparotomy. We believe that wide hepaticojejunostomy at the hilum for sufficient bile drainage of the intrahepatic duct is essential for prevention of postoperative complications. This procedure appears to be feasible for the surgeon with an advanced laparoscopic skill set and an attractive alternative to conventional laparotomy for choledochal cyst.
Footnotes
Disclosure Statement
No competing financial interests exist.