
Abstract
Abstract
Background:
Thyroid surgery has recently emerged as one of the most promising fields for the application of robotic surgery. We report the results of the first year of experience with a gasless transaxillary thyroidectomy.
Subjects and Methods:
From January 2009 to December 2009, 10 consecutive patients (8 women) underwent robotic thyroidectomy through a gasless transaxillary approach. The median age was 44 years (range, 27–42 years). Eight total and two partial thyroidectomies (one left and one right) were performed using the da Vinci® Robotic Surgical System (Intuitive Surgical, Sunnyvale, CA). Preoperative diagnosis included solitary nodules with a median size of 16±11 mm (range, 3–44 mm) at preoperative imaging.
Results:
All procedures were successfully completed robotically, except one that was converted because of difficulty in achieving an optimal exposure. The overall mean operative time was 177.4±40 minutes (range, 120–240 minutes) with minimal blood loss (<10 mL). Pathological diagnoses included papillary carcinoma (n=6), colloid nodule (n=2), and multinodular goiter (n=2). The mean number of lymph nodes harvested in the cases of malignant disease was 4±5 (range, 3–15). The median postoperative length of stay was 1.05 days (range, 1–1.4 days).
Conclusions:
Thyroid surgery using a gasless transaxillary approach can be performed safely for selected benign and malignant pathology. This approach offers superior cosmetic results and a short hospital stay over conventional thyroid surgery. For selected patients, this technique offers a promising scarless option for minimally invasive thyroid surgery.
Introduction
Thyroid disease is more frequent among women than men, and the presence of a scar on the neck is a major concern for this population. As a result, over the last few years the goal of minimally invasive thyroid surgery has been not only to maintain the safety and functional results of conventional thyroidectomy, but also to minimize the length of the scar on the neck. Three different surgical approaches have been described for thyroid surgery: (1) a mini-open lateral approach via a small incision, 3 (2) minimally invasive video-assisted thyroidectomy (MIVAT) via the midline, 4 and (3) an endoscopic technique.5–8
Among the various endoscopic techniques, the transaxillary approach was initially described by Ikeda et al. 8 in 2000. The aim was to completely avoid any presence of a scar on the neck. The cosmetic results are optimal because the scar is normally hidden by the arm in its natural position. Nevertheless, widespread use of this approach has not occurred because of its technical limitations, including the need for CO2 insufflation to create a working space, as well as the technical complexities associated with managing nonflexible endoscopic instruments in a two-dimensional operative view. 9
In order to overcome these limitations, robotic surgery has been used to perform the transaxillary approach to thyroidectomy. In fact, the feasibility and safety of this approach were recently reported in a large series by the Yonsei University group.10,11 In the United States, however, this approach remains scarcely adopted and underreported. 12 Herein, we describe the initial experience with gasless robotic transaxillary thyroidectomy at the University of Illinois at Chicago.
Subjects and Methods
Patients
The data of 10 consecutive patients treated with gasless robotic transaxillary robotic thyroidectomy at the University of Illinois at Chicago from January 2009 to December 2009 were prospectively collected in a dedicated database and retrospectively reviewed for this study. Data collected and analyzed included patient characteristics, operative variables, and postoperative morbidity.
Selection criteria and postoperative care
We used the same selection criteria for gasless transaxillary robotic thyroidectomy as have been previously described by others.10,11,13 In brief, the indications for this approach included (1) benign thyroid tumors with a maximum diameter of less than 5 cm (as estimated by preoperative ultrasonography and preoperative fine-needle cytology) and (2) well-differentiated thyroid carcinoma with size less than 2 cm and without preoperative diagnosis of lymph node metastases. Preoperative diagnosis of thyroid tumors was based on the results of fine-needle aspiration cytology and ultrasonography. Exclusion criteria included (1) severe thyroiditis, (2) malignant tumor with extrathyroidal tumor invasion, multiple lateral neck node metastases, or distant metastasis, and (3) history of previous neck irradiation. The presence of previous thyroid surgery did not constitute a contraindication. Preoperatively and every day after surgery the total fasting blood calcium was monitored until discharge.
Surgical technique
The technique of robotic total thyroidectomy has been previously described by Yoon et al. 13 and Kang et al. 10 After undergoing general anesthesia with orotracheal intubation, the patient is placed on the table in a supine position with the neck extended, and the ipsilateral arm is placed on an arm board and extended cephalad to exposed the axilla.
A 5–6-cm vertical incision is then performed in the axilla, and a plane is created between the subcutaneous tissues and the pectoralis major muscle fascia using a combination of monopolar coagulation and blunt dissection toward the clavicle (Fig. 1). Once the medial border of the sternocleidomastoid muscle is exposed, the dissection begins through the avascular space between the clavicular and sternal heads of the sternocleidomastoid muscle, and the sternal head is elevated and retracted, exposing the strap muscles. The latter are then elevated off of the thyroid gland, providing a complete exposure of the thyroid lobe from the sternal notch to the upper thyroid pole and the midline. Next, in order to maintain an adequate working space, a personally specially designed retractor is inserted through the skin incision in the axilla and raised up using a lifting device being attached to the operative bed in order to maintain an optimal working space (Fig. 2). The retractor is then inserted through the axillary skin incision and placed between the anterior surface of the thyroid and the strap muscle. The retractor is used to raise and tent a skin flap at the anterior chest wall, the sternal head of the sternocleidomastoid muscle, and the strap muscles in order to create the working space.

Creation of the subcutaneous tunnel.

Placement of the retractor.
An additional 8-mm incision for the robotic fourth arm is then made on the medial side of the anterior chest wall, 2 cm superiorly and 6–8 cm medially from the nipple.
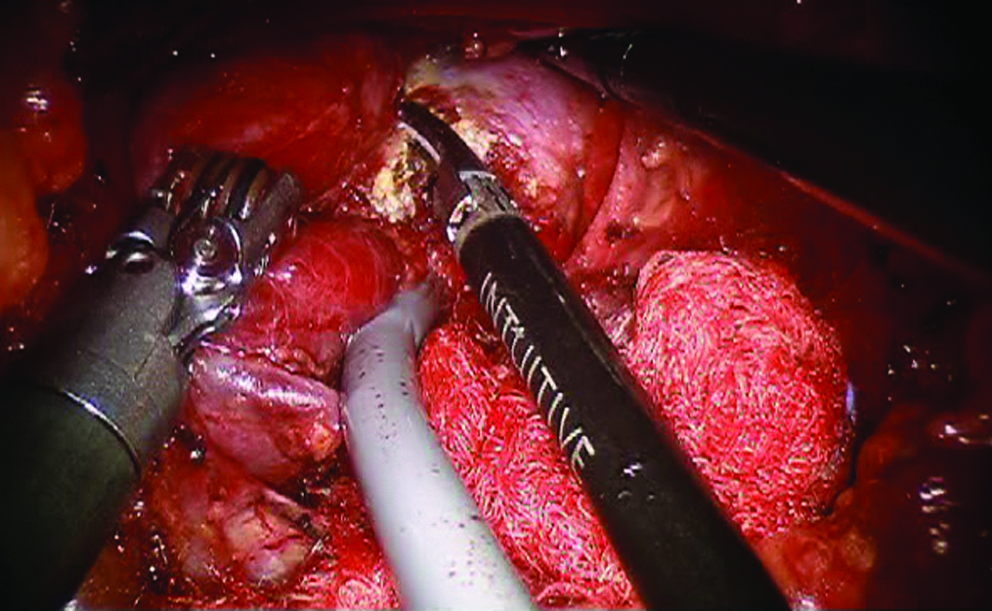
All four robotic arms are used for this operation. Three arms are inserted through the axillary incision, including the 30° camera placed on the central camera arm, the Harmonic® shears (Ethicon Endo-Surgery) placed on the right arm, and the Maryland dissector placed on the left side arm (Fig. 3). A Prograsp® forceps (Intuitive Surgical, Sunnyvale, CA) is placed on the fourth arm and inserted through the 8-mm anterior chest trocar. The robotic cart is placed from the opposite direction of the operative field. The operation proceeds in the same manner as a conventional open thyroidectomy.

Trocar positioning through the axillary incision.
The upper pole of the thyroid is retracted downward and medially using the Prograsp forceps, and the superior thyroid vessels are identified and sealed close to the thyroid gland. This is done using the Harmonic shears in order to avoid injury to the external branch of the superior laryngeal nerve, which is clearly identified thanks to the magnified vision provided by the robotic system. The upper pole of the thyroid gland is then detached from the cricopharyngeal and cricothyroid muscles until the superior parathyroid gland is identified and preserved. The inferior pole is then dissected free from the surrounding tissues, and the mediastinal and inferior thyroid veins are divided close to the gland. Continuous care is taken in order to avoid contact between the active blade of the Harmonic shears and critical structures. The thyroid lobe is then retracted medially using the Prograsp forceps and suspended, and the inferior thyroid artery and recurrent laryngeal nerve (RLN) are identified (Fig. 4). Once the course of the RLN has been identified, the middle thyroid vein is divided. As dissection continues medially, Berry's ligament is then divided. Lastly, the isthmus is divided, and the specimen was extracted through the axilla (Fig. 5).
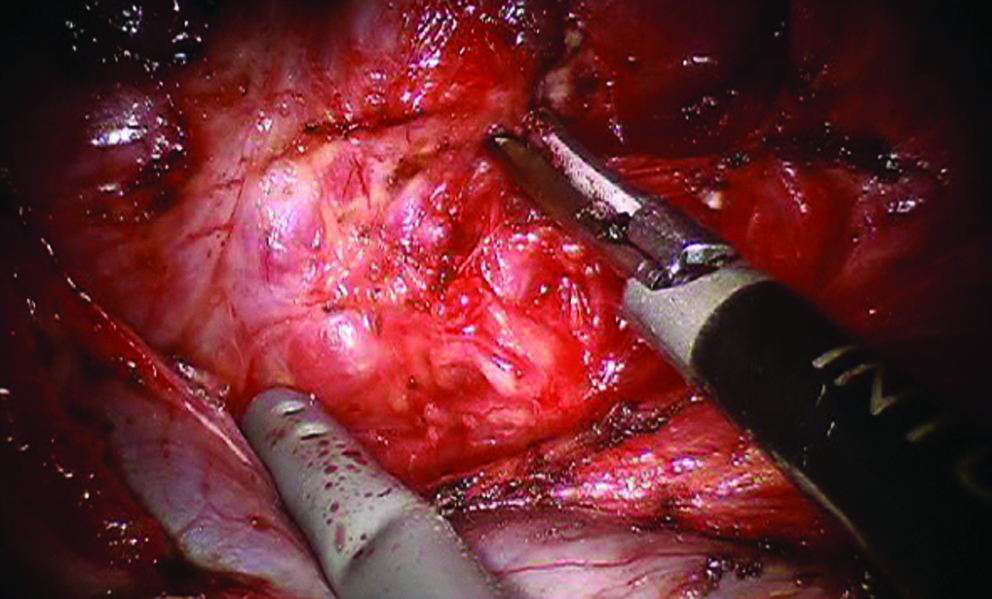
Lateral dissection of the thyroid gland.
Sectioning of the thyroid's isthmus.
In the case of total thyroidectomies, the dissection, performed through the same axillary incision with the same robotic cart configuration, begins with the transection of the contralateral superior pole. A subcapsular dissection is then performed between the thyroid medially and the trachea. After the RLN is identified the thyroid is carefully dissected off the nerve and removed. The resected specimen is extracted through the axilla. A closed suction drain is inserted through the same orifice used for the fourth robotic arm.
Results
All transaxillary thyroidectomies were completed robotically, with the exception of one (10%) that required conversion to open surgery because of difficulties in achieving the appropriate exposure. Patient characteristics and surgical outcomes are reported in Table 1. The mean operating time was 177.4±40 minutes (range, 120–240 minutes) with minimal blood loss (<10 mL). Eight total thyroidectomies and two partial thyroidectomies (one left and one right) were performed. The malignant disease pathology revealed five papillary carcinomas and one follicular variant of papillary carcinoma. Two of the lesions were papillary microcarcinoma. The pathological stage was T1 N0 (n=3), T1 N1 (n=2), and T2N1 (n=1). The mean tumor size was 12±8 mm (range, 3–21 mm), and the mean number of lymph nodes harvested was 4±5 (range, 3–15).
Benign pathology consisted of multiple colloid nodules (n=2) and multinodular goiters (n=2). One patient developed a transitory inferior recurrent nerve dysfunction that resolved in the 2 months after the operation. No patients developed a postoperative hypocalcemia. The mean postoperative length of stay was 1.05 days (range, 1–1.4 days). There were no postoperative hematomas or seromas, and all patients showed normal arm function after the operation. All patients were subjectively pleased with the cosmetic results on the short- and long-term interval. Of the 6 patients who underwent total thyroidectomy for papillary cancer, 3 were high risk and underwent radioactive iodine treatment. All patients were followed up with neck ultrasonography at 3 and 6 months and serum thyroglobulin level determination, during which time there was no recurrent disease.
Discussion
Minimally invasive thyroid surgery has seen an exponential growth over the last 10 years. The advantages of endoscopic thyroidectomy over conventional open thyroidectomy include better cosmetic appearance, minimal pain, shorter hospital stay, lower incidence of postoperative hyperesthesia or paresthesia in the neck, and less discomfort while swallowing. 14
The most common approaches include a video-assisted technique with a minimal incision on the neck.9,15 The adoption of the MIVAT, however, has been slow because of the increased operative time and longer learning curve required. 15 MIVAT was described by Miccoli et al. 16 in 1999, and its safety and feasibility have been reported in patients with malignant and benign disease. 15 Still, the technique does create a scar, although minimal, on the neck.
Postoperative cosmetic appearance following thyroid surgery remains a major concern for patients, in particular for young women. Several remote approaches to the thyroid gland have been developed to totally avoid the presence of a skin incision on the neck. The remote technique can be applied to endoscopic thyroidectomy using the breast, 17 anterior chest, 18 or axillary approaches. 9
The transaxillary endoscopic approach to the neck has been proposed as an esthetic solution for patients who do not wish to have a scar on their neck. The cosmetic results of this approach are superior when compared with conventional endoscopic thyroidectomy because the surgical scar, even if hypertrophic, is completely covered by the arm in its natural position. 19 From a technical point of view, this approach offers a lateral view of the thyroid gland, thereby providing an operative field that is equivalent to the view obtained during open conventional thyroidectomy. 13 This approach also offers easy identification of the thyroid gland, laryngeal nerves, and parathyroid glands.
Still, this approach does require extensive dissection in the anterior thoracic region, which can cause postoperative prolonged discomfort. In addition, adequate exposure of the operative field can require CO2 insufflation, which can also cause complications. 19 Finally, the conventional video-endoscopic technique remains limited by technical challenges such as an unstable video camera platform, limited motion of rigid instruments, and unsatisfactory operator ergonomics.
Recently, the da Vinci® Robotic Surgical System (Intuitive Surgical) has been used for this approach in order to maximize the cosmetic benefits of the transaxillary approach while overcoming the technical limitations of conventional endoscopic instrumentation.10,11,20 The results of our preliminary experience confirm the safety, feasibility, and good short-term outcomes of this approach. The robot offers improved three-dimensional vision, use of EndoWrist® (Intuitive Surgical) instruments, and improved ergonomics for surgeons. 21 The technical abilities of the system, including its three-dimensional vision, help to magnify the target structures, which can allow for easier identification and preservation of the parathyroid and recurrent laryngeal nerves. Additionally, the technical abilities of the wristed instruments allow for lymph node dissection in a narrow, deep working space.
To the best of our knowledge, only a few centers are currently using a transaxillary approach for robotic thyroidectomy.12,22,23 Kang et al. 20 described a series of 100 consecutive robotic transaxillary thyroidectomies, all performed using the da Vinci Robotic Surgical System. In that study, the authors performed 16 total thyroidectomies (16%) and 84 partial thyroidectomies (84%) with a mean operative time of 136.5 minutes and no permanent injury to the RLN. Of note in this study is that they reported significantly decreased transient hypocalcemia when compared with a previous series of open thyroidectomies (16.6% versus 38.5%). The number of lymph nodes harvested in their experience was 5.26±3.9 (range, 1–28). Later, this same group reported the largest series to date of robotic transaxillary thyroidectomies, which included 387 patients and 104 total thyroidectomies (30.76%); in this later experience, the authors reported an overall operative time of 144.0±43.5 minutes, no conversions, and a mean postoperative hospital stay of 3.3 days (range, 2–7 days). 11 In that experience, however, the authors reported 41% of cases developed transient hypocalcemia, and there were 3 cases (1%) of permanent injury to the recurrent laryngeal nerve.
Following an earlier experience in a cadaver lab, we applied the robotic transaxillary technique in our patients. Our selection criteria are similar to those reported by others. In particular, we chose to limit the size of lesions to 5 cm for patients with benign disease and only 2 cm for well-differentiated tumors. Compared with previous series described, we report an increased operative time, likely because of our limited experience. We believe that this will decrease as we gain more experience. Also, in our experience we had to convert 1 patient to open surgery because of difficulty in achieving an optimal exposure. Correct exposure of the contralateral upper lobe in total thyroidectomy by a transaxillary approach has been reported by others to be difficult as well.8,13,19
One could argue about the safety of removing the entire contralateral lobe during a total thyroidectomy via an ipsilateral incision and the ability to visualize the contralateral RLN and parathyroid. We do recognize that, even if we did not have any permanent RLN injury, we felt it is more difficult to dissect the contralateral lobe by the same transaxillary access, and we, like others, 23 do not recommend performing this kind of operation through an ipsilateral approach by surgeons not proficient in robotic thyroid lobectomy. Moreover, in our experience, this limitation has been resolved by using the fourth robotic arm to perform the appropriate retraction with the use of a 30° scope. Doing so provided good results regarding short-term outcomes, morbidity, and oncologic clearance. Still, a long-term prospective study is needed in order to validate the initial results of this approach for malignant disease. Again, the cosmetic results appear superior when compared with the open approach.
Conclusions
This preliminary small series from a medical center in the United States confirms the safety of robot-assisted total and partial thyroidectomy using an axillary approach. The advantages provided by the robotic system make minimally invasive thyroidectomy by a remote transaxillary approach more feasible. As a result, this technique has the potential to become a desirable cosmetic approach for minimally invasive surgery of the thyroid.
Footnotes
Disclosure Statement
No competing financial interests exist.