
Abstract
Abstract
Introduction:
The aim of this study was to review our experience with the hand-assisted laparoscopic management of duodenal tumors with no or low malignant potential and to compare this approach with published case reports of purely laparoscopic local duodenal resection.
Patients and Methods:
Eight cases of hand-assisted laparoscopic local duodenal resection performed from 2000 to 2008 were retrospectively reviewed. Hand-assistance was utilized for complete duodenal mobilization, and local duodenal resection was accomplished extracorporeally through the hand-access incision. Patient and tumor characteristics, operative time, length of stay, and complications were compared with 18 cases of totally laparoscopic local excision of duodenal tumors published since 1997. Patients with ampullary tumors were excluded.
Results:
Compared with the purely laparoscopic approach, the hand-assisted technique was associated with shorter operative time (179 versus 131 minutes, P=.03) and was more commonly used for lesions located in the third portion of the duodenum (0% versus 37.5%, P=.02). Tumor size (2.9 cm versus 3.2 cm, P=.61) and length of hospital stay (5.9 versus 5.9 days, P=.96) were similar between the two groups. The rate of complications was also comparable (0% versus 12.5%, P=.31); 1 of 8 patients in the hand-assisted group developed an incisional hernia at the hand-access site.
Conclusion:
Hand-assisted laparoscopic local duodenal resection is a feasible, safe, and effective alternative to the totally laparoscopic approach. In addition to being associated with comparable length of hospital stay, hand-assistance can shorten operative time by facilitating duodenal mobilization as well as extracorporeal duodenal resection and closure.
Introduction
Laparoscopy in the management of such lesions has been adopted with gradually increasing frequency in recent times. Since 1997, about 18 cases of entirely laparoscopic local resection of a duodenal tumor have been reported.6–20 In addition, several authors have reported totally laparoscopic transduodenal ampullectomies for lesions arising from the ampulla of Vater.21,22 The aim of this study was to present our experience with the hybrid resection (hand-assisted laparoscopic duodenal mobilization and open local excision) of duodenal tumors with no or low malignant potential, and to compare the outcomes of this approach with previously published cases of purely laparoscopic local duodenal resection.
Materials and Methods
Hybrid duodenal resection
From 2000 to 2008, eight patients underwent hybrid resection of a duodenal tumor at Hartford Hospital, Hartford, CT. All resections were performed by the 2 senior authors (R.O. and G.P.B.) of this report. Patients were evaluated preoperatively with upper endoscopy (Fig. 1) and endoscopic ultrasonography (Fig. 2) to establish the pathologic diagnosis and delineate the exact location, size, and depth of the lesion. Endoscopic snare polypectomy was selectively considered or attempted, but these 8 patients had tumors not amenable to endoscopic excision because of size, sessile configuration, or depth of invasion. Patients with body mass index (BMI) >30, ampullary tumors, or adenocarcinoma of the duodenum underwent open resection and were not included in this cohort.

Endoscopic appearance of a 2.6-cm tubular adenoma in the duodenal bulb. The sessile configuration of the lesion (wide base is marked by the arrows) precluded endoscopic polypectomy, and the patient underwent hand-assisted laparoscopic resection with an operative time of 90 minutes and a hospital stay of 5 days.
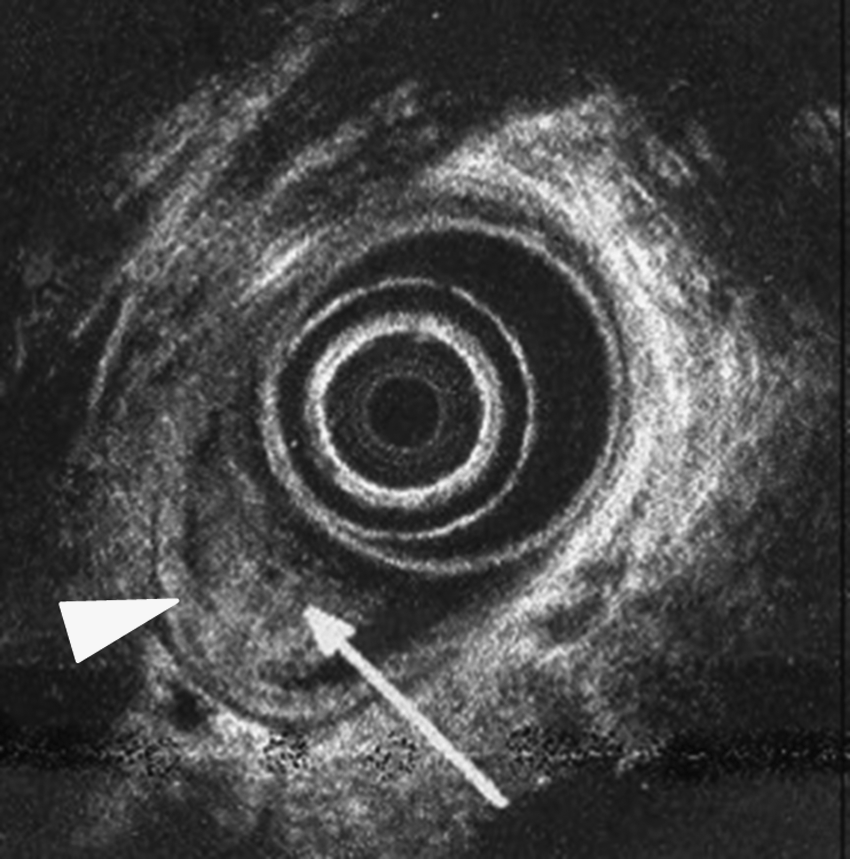
Endoscopic ultrasonography shows the lesion illustrated in Figure 1 (arrow) to originate from the mucosa without invasion into the submucosa (second hyperechoic layer, arrowhead).
With the patient in the supine position and the surgeon standing on the left side of the patient, umbilical Hasson cannulation of the abdomen was performed. A 7.5-cm right-upper-quadrant paramedian incision was made for the hand-assistance device. Working ports were placed in the left upper quadrant (Fig. 3). Initially the Pneumosleeve (Dexterity Surgical, Inc., Houston, TX) and subsequently the Gelport (Applied Medical, Inc., Rancho Santa Margarita, CA) hand-access devices were used. Hand-assistance facilitated expeditious hepatic flexure takedown, and wide Kocher maneuver (Fig. 4), as well as tumor localization and examination by palpation (Fig. 5). Intraoperative endoscopy was required to localize nonpalpable tumors in 4 (50%) cases. The hand-port was then removed and the fully mobilized duodenum was approached extracorporeally through the right paramedian incision. Abdominal wall retraction was provided by the inner sheath of the hand-assistance device or a table-mount pediatric laparotomy retractor. Local excision of the lesion was carried out in a standard fashion; a transduodenal approach was carried out for lesions located at the medial wall of the duodenum toward the pancreatic head. The plane of resection was submucosal when feasible (4 patients) and full-thickness in the remaining 4 cases. The duodenotomy was closed transversely to preserve the lumen of the duodenum, using 3-0 silk Gambee sutures. Drains were not used. Postoperative recovery pathways were not standardized, but left to the discretion of the individual surgeon. Medical records were reviewed retrospectively to define patient and tumor characteristics, operative time, length of hospital stay, complications, and disease recurrence.
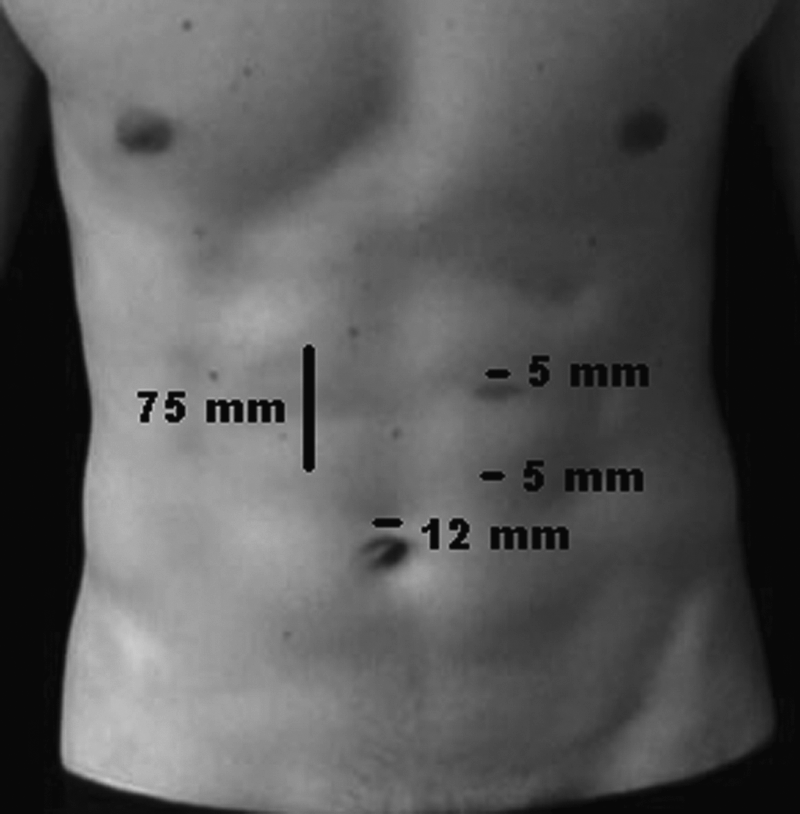
Suggested port site placement for hand-assisted laparoscopic local duodenal resection.

Hand-assistance provides versatile retraction for wide and expeditious duodenal kocherization.

Hand-assisted palpation of the duodenum facilitates tumor localization as well as assessment of the tumor's mobility or fixation to adjacent structures.
Laparoscopic local duodenal resection
The first two reports of a totally laparoscopic local excision of a benign duodenal neoplasm were published in 1997.6,7 Since then, a total of 18 cases of purely laparoscopic local resection for benign or indolent duodenal tumors have been reported in the English literature.8–20 These reports were reviewed and corresponding authors personally contacted when necessary to collect patient and tumor characteristics, operative time, length of stay, and incidence of complications.
Statistical analysis
The two groups of patients—our series of hybrid resections and the previously published purely laparoscopic cases—were subjected to univariate statistical comparisons. Patient characteristics and outcomes were compared using the Fisher's exact test for categorical variables and the Mann–Whitney U-test for numerical variables. Results are presented as frequencies (percentages) for categorical variables and as mean (standard deviation) for numerical variables. Statistical analysis was performed using the SPSS statistical software package (version 16.0, Chicago, IL). A two-tailed P value of <.05 was considered statistically significant.
Results
Patient characteristics and outcomes of our series of hybrid duodenal resections are shown in Table 1. Final pathologic diagnoses were tubular adenoma (n=4), carcinoid (n=1), GIST (n=1), lipoma (n=1), and Brunner's gland hyperplasia (n=1). Three tumors were located in the third portion of the duodenum (D3), three in the second (D2), and two in the duodenal bulb (D1). Mean BMI was 23 (range 21–25). Estimated blood loss was minimal in all cases. All margins of resection were microscopically negative, except for one 85-year-old patient with a 2-cm carcinoid tumor, located 2 cm from the ampulla of Vater (patient 7). Pancreaticoduodenectomy was offered to treat the positive margin and potential lymph node involvement, but the patient eventually refused. He is alive with no evidence of disease recurrence 7 years from his initial hand-assisted laparoscopic local resection. Conversion to an open procedure by extending the incision for 3 cm was necessary during resection of a D3 adenoma in one patient (patient 6). An incisional hernia at the hand-port site developed in another patent. Adenoma recurrence has been observed in 1 of 4 patients on routine endoscopic surveillance at mean follow-up of 33 months (range 6–84). This patient (patient 8) was 87 years old at the time of recurrence, which was managed with endoscopic Yttrium Aluminium Garnet laser photoablation with a durable result at 12-month follow-up.
D1, first; D2, second; D3, third portion of duodenum.
GIST, gastrointestinal stromal tumor.
Patient characteristics and outcomes for the 18 reported cases of totally laparoscopic local excision of duodenal neoplasms are shown in Table 2. Estimated blood loss was minimal and resection margins were negative in all cases. All lesions were located in the first or second portions of the duodenum. No lesion in the third portion of the duodenum has been reported to have been treated in a totally laparoscopic fashion. Patients with ampullary lesions were not included in this cohort.21,22 No complications were encountered in this group.
D1, first; D2, second; D3, third portion of duodenum.
N/A, not available.
Descriptive statistics were used to compare the two groups of patients in terms of patient and tumor characteristics, as well as operative and postoperative outcomes (Table 3). Tumor size was similar between the two groups. Compared with the totally laparoscopic approach, the hybrid technique was associated with shorter operative time (179 versus 131 minutes, P=.03) and was also more commonly utilized for lesions located in the third portion of the duodenum (0% versus 37.5%, P=.02). A purely laparoscopic resection of a tumor located in the third portion of the duodenum has never been reported to our knowledge. Despite that the hybrid approach was applied to older patients (50 versus 67 years, P=.01), both groups had similar lengths of hospital stay (5.9 versus 5.9 days, P=.96), underscoring that this approach maintains the advantages of laparoscopy in terms of shorter hospitalization and faster recovery. The rate of complications was similar between the two groups (0% versus 12.5%, P=.31); however, in the hybrid group, 1 out of 8 patients developed an incisional hernia at the hand-port site, a complication that was not encountered in the laparoscopic cohort.
Results are presented as frequencies (percentages) for categorical variables and as mean (standard deviation) for numerical variables.
No. of lesions located in the third portion of duodenum.
Lap, laparoscopic.
Discussion
In this study we present our experience with 8 patients who underwent a hybrid approach for local duodenal resection (laparoscopic hand-assisted duodenal mobilization followed by open local resection and reconstruction through the hand-access incision) in comparison with 18 cases of totally laparoscopic resection of duodenal tumors previously reported in the English literature. Despite the fact that the hybrid approach was generally performed on older patients, both groups had similar lengths of hospital stay and complication rates, suggesting that the hybrid approach in this clinical situation is a feasible, safe, and effective alternative to totally laparoscopic resection. In addition, the hybrid approach was associated with shorter operating times and was also applied for lesions located in the third portion of the duodenum.
Approximately 3% of all gastrointestinal neoplasms are found in the small intestine, with duodenal neoplasms accounting for 35% of all benign and 17% of all malignant small-bowel tumors. 23 The therapeutic approach to duodenal tumors (endoscopic removal, local resection, formal segmental resection, or pancreaticoduodenectomy) remains unsettled because of the complexity of the relevant anatomy, the rarity of these tumors, and the wide spectrum of histologies that can be encountered. Endoscopic resection is increasingly being utilized, but proper patient selection is important. There is no definite guideline as to the size of benign nonampullary duodenal neoplasms above which surgical rather than endoscopic resection should be considered. Some authors recommend that lesions larger than 2 cm, extending to the submucosa, or involving more than a third of the circumference of the duodenal lumen should be considered for surgical resection,5,24 although successful endoscopic resection of benign lesions up to 5 cm has been reported. 25 Since the most important complication of endoscopic resection of large submucosal lesions is unrecognized perforation, our current anecdotal approach for such lesions is to attempt endoscopic resection in the operating room under laparoscopy, which can enable prompt identification and repair a transmural duodenal wall defect.
GISTs and carcinoids (neuroendocrine tumors) represent gastrointestinal malignancies with overall low metastatic potential. Local (wedge) resection with negative margins is appropriate surgical therapy for GISTs as they represent visceral sarcomas of the gastrointestinal tract that do not generally metastasize to regional lymph nodes. 26 However, the extent of resection (local/wedge resection versus segmental resection/pancreaticoduodenectomy) necessary for carcinoid tumors of the duodenum remains controversial. A previous pathologic study of 99 duodenal carcinoids reported features associated with metastatic risk to be involvement of the muscularis propria, >2 cm, and the presence of mitotic figures. 27 It is now established that carcinoid tumors arising from the ampulla of Vater exhibit considerably more aggressive behavior, with a strong tendency to develop nodal metastasis even at a small size (<2 cm) and pancreaticoduodenectomy is recommended irrespective of tumor size. 28 In addition, a recent surgical series of 24 patients with duodenal carcinoid tumors (gastrinomas and ampullary carcinoids were excluded) reported that although the majority (89%) of tumors measured <2 cm, and most (85%) were limited to the mucosa or submucosa, lymph node metastases were identified in the surgical specimen in 7 (54%) of 13 patients in whom lymph nodes were examined, including 2 patients with tumors smaller than 1 cm and limited to the submucosa. Therefore, the authors concluded that the presence of regional lymph node metastasis cannot be predicted reliably on the basis of tumor size or depth of invasion. 29
Several studies have evaluated the utility and benefits of hand-assistance in laparoscopic abdominal surgery. Hand-assisted laparoscopy has gained wide clinical acceptance as a practical alternative to totally laparoscopic surgery for various surgical procedures, including colectomy, splenectomy, liver resection, and nephrectomy. A recent systematic review of hand-assisted versus laparoscopic-assisted colectomy showed the former to be a valid alternative to the later particularly in the management of complex diverticular disease or when total (procto)colectomy is required, reducing conversion rates and operative times, whereas morbidity and length of stay did not differ. 30 Hand-assistance is a minimally invasive technique that provides tactile feedback and a more acceptable learning curve, eliminating some of the technical challenges of conventional laparoscopy. Another systematic review demonstrated that hand-assistance in colorectal surgery is advantageous compared with open surgery (shorter operative time and lower conversion rate). 31 Especially for indications in which an incision to extract the resection specimen is required, hand-assistance provides an excellent treatment option. For example, in the setting of splenomegaly, the three largest retrospective series to date suggest similar postoperative results between hand-assisted and purely laparoscopic splenectomy.32–34 Moreover, a recent prospective study found hand-assisted laparoscopic splenectomy superior to open splenectomy in terms of incision length, postoperative pain score, postoperative drain output and duration, as well as hospital stay, maintaining the advantages of tactile sense and atraumatic specimen manipulation. 35 Overall, the bulk of evidence suggests that hand-assistance maintains the benefits of minimally invasive surgery, whereas affording the surgeon the ability to carry out complex cases in a time-efficient fashion.
Herein, we report a case-controlled analysis of hybrid versus totally laparoscopic resection of duodenal tumors. Several limitations must be considered when interpreting the results of a study of this kind. First, the study is retrospective and obviously selection bias is introduced when the decision was made as to which patient received what treatment. Moreover, the control group for this study consisted of several, mostly single case reports of laparoscopic resection of duodenal tumors published separately from a variety of different institutions and likely represented the initial procedure in each author's learning curve. Realizing the limitations of cross-study comparisons, our goal was not to establish the noninferiority of the hand-assisted in relation to the totally laparoscopic approach. When the skill set is available, a totally laparoscopic approach is certainly preferable. Nonetheless, since these types of tumors are rare, and most surgeons will likely be early in the learning curve of their laparoscopic management, the purpose of our study was to present our experience with this hybrid approach as a feasible, safe, and effective tool in this clinical situation.
In conclusion, our findings suggest that in appropriately selected patients, the addition of hand-assistance can safely facilitate the laparoscopic local excision of duodenal tumors by expediting tumor localization, duodenal kocherization, and extracorporeal duodenal resection and closure. This approach appears to be associated with a shorter operative time than the totally laparoscopic procedure, and an equally short hospital stay, maintaining some of the advantages of laparoscopic surgery. In addition, this approach can be potentially used in the minimally invasive treatment of lesions in the third portion of the duodenum, an area that has been traditionally considered inaccessible to conventional laparoscopy.
Footnotes
Disclosure Statement
No competing financial interests exist.