
Abstract
Abstract
Wandering spleen (WS) is an uncommon condition, usually asymptomatic, often recognized as an incidental finding. When symptoms occur, they can vary, although acute abdominal pain is the most common presentation in the pediatric population. In some cases, WS can become a dangerous condition because of the risk of splenic ischemia from persistent pedicle torsion. We describe a case of WS in a 3-year-old boy presenting with vomiting, abdominal swelling, and acute pancreatitis; the diagnosis was obtained by ultrasound and computed tomography. Laparoscopic splenopexy was successfully performed through an extraperitoneal pocket and a Vicryl mesh. To the best of our knowledge, the combination of gastric outlet obstruction and acute pancreatitis has never been reported as presenting symptoms of WS.
Introduction
The condition predisposes the spleen not only to twist around its pedicle, but also to an increased risk of traumatic injury owing to its more superficial location. Therefore, once the diagnosis is made, surgery is suggested, even in asymptomatic patients.
Although splenectomy has been traditionally the preferred treatment, preservation of the viable spleen has been recommended more recently and various techniques for splenopexy have been described either through laparotomy or a laparoscopic approach.
Case Report
A 3-year-old boy presented with a 2-day history of persistent vomiting and upper abdominal swelling. He had never suffered from such a condition before; the parents referred chronic constipation and occasional enlargement of the abdomen without tenderness.
Physical examination revealed abdominal distension without a clearly palpable mass. Blood tests showed an increase in pancreatitis markers (amylases 967 UI/L, lipases 823 UI/L), and ultrasonography and computed tomography (CT) scans demonstrated a massively distended stomach with an air–fluid level and an abnormal right-sided spleen without any sign of ischemia (Fig. 1).
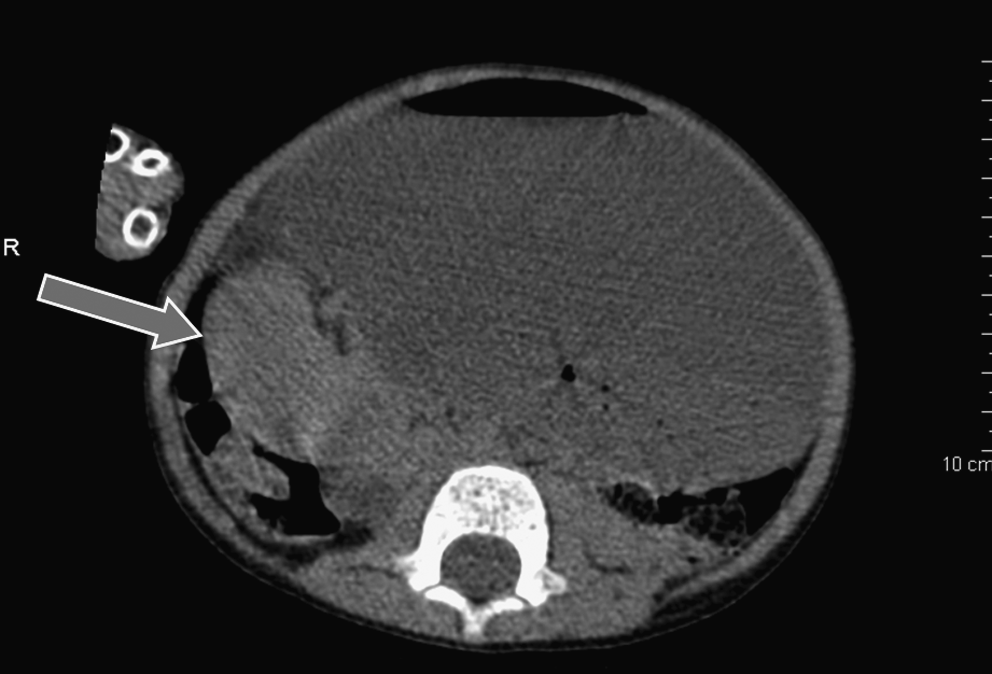
Computed tomography scan: the massively distended stomach is filled with fluid and occupies the upper abdomen almost entirely. The spleen (indicated by arrow) lies in the right hypochondrium.
A nasogastric tube was inserted, draining 1200 cc of clear fluid. An ultrasound (US) examination performed a few days later showed moderate swelling of the pancreas and a normally located spleen with a long pedicle; moderate splenomegaly was noticed (transverse diameter: 8.5 cm), probably because of a chronic vascular congestion. WS was thus suspected and the diagnosis was confirmed by a dynamic US test performed with the patient lying on the bed and then moving to the upright position; during this maneuver, the position of the spleen changed from its normal position toward the left lower quadrant; no changes in the blood flow through the splenic vessels could be documented during the examination. Elective laparoscopic splenopexy was then planned.
At readmission after 2 weeks, blood tests were normal and an US performed the day before surgery showed a normally located spleen. The night before surgery, vomiting and mild abdominal tenderness reappeared in a previously completely asymptomatic patient.
Surgical Procedure
A 5-mm trocar was inserted through an umbilical access for the scope and pneumoperitoneum was established. At laparoscopic exploration the spleen was found in the right flank, under the liver; it was attached to a stretched vascular pedicle that encircled the gastric antrum, thus causing a severe obstruction and distension of the stomach. No twisting of the pedicle was seen; the spleen was mildly enlarged without signs of vascular compromise. Three additional 5-mm working ports were inserted under endoscopic control into the epigastric, right flank, and right hypogastric regions.
Once the spleen was repositioned back to the left subphrenic space, a small skin incision was made in the 10th intercostal area, and a space between the posterolateral peritoneum and the underlying muscles and diaphragm was developed through blunt dissection with the aid of a clamp; a balloon catheter was introduced through the incision and a large extraperitoneal pocket was gradually created by filling the balloon with up to 350 cc of saline, to allow introduction of the spleen. A linear incision was then made on the peritoneal surface and the spleen was carefully placed into the newly created pocket.
The peritoneal incision was partially approximated with two absorbable sutures, and to prevent a tight closure of the pocket, a Vicryl mesh was fixed to the peritoneal edges with 2/0 Vicryl sutures, taking special care not to impair splenic perfusion. No drain was inserted (Figs. 2 and 3).
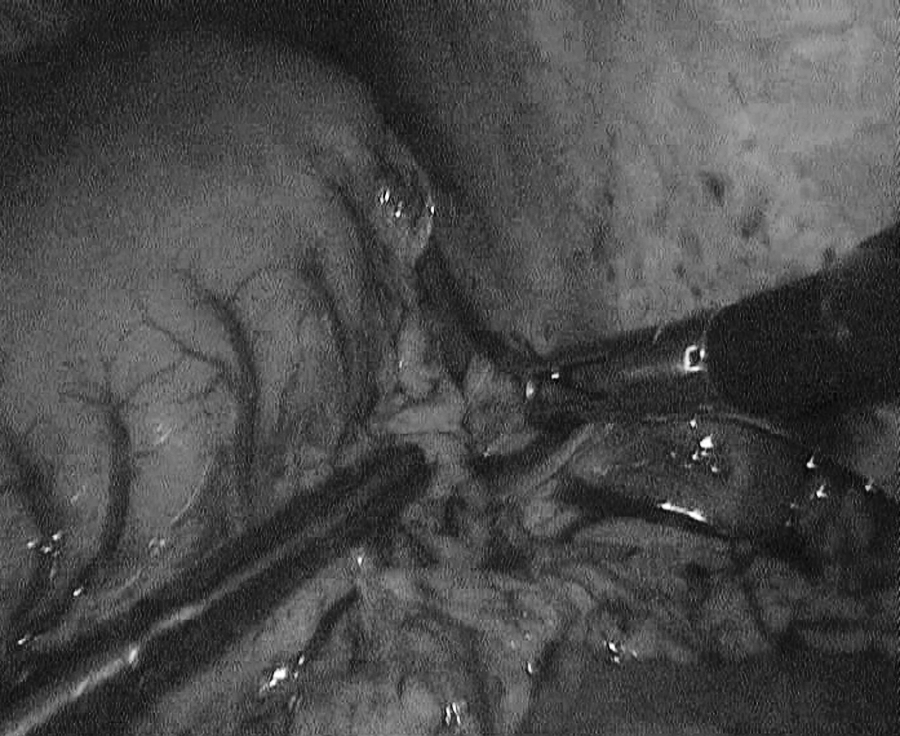
The spleen has been encased in the newly created extraperitoneal pocket whose margins have been partially approximated.

A Vicryl mesh is fixed to the peritoneal margins of the pocket to avoid excessive compression of the spleen or possible vascular impairment.
The total operating time was 190 minutes. Intraoperative blood loss was minimal. A Doppler US examination performed at 2 days postoperatively revealed that the spleen rested in a normal position and showed good perfusion. After an uncomplicated recovery, the patient was discharged on the third postoperative day.
At 9 months follow-up, the patient is doing well; he has no recurrent abdominal pain or gastric distention. An US performed at 4 months postoperatively showed no change in splenic position or perfusion.
Discussion
WS is a rare condition that is difficult to diagnose because of its nonspecific symptoms; a heightened awareness of the condition is therefore required for accurate diagnosis and appropriate management. Recurrent abdominal pain, caused by intermittent torsion or vascular kinking, is a frequent complaint, often associated with a mass, either in the left flank or in the pelvis. Unfortunately, many of these patients undergo several hospital admissions and repeated inconclusive workups for recurrent abdominal pain, before a correct diagnosis is achieved. Patients may also present with occasional nausea and emesis, but in most of the cases WS is found incidentally during a routine physical examination or imaging investigation. 1 Acute abdominal pain due to splenic torsion may be the first presentation of the disease; its early identification is challenging, especially in children. Association of WS with recurrent acute pancreatitis or urinary symptoms (enuresis and hydronephrosis) or gastric volvulus and duodenal obstruction have also been described.2,3 The mechanism by which pancreatitis is determined is difficult to demonstrate; it could be secondary to compression from either the splenic vessels or the stomach.
Although WS usually presents between the ages of 20 and 40 years, children account for one-third of all cases, especially below 1 year of age; after age 10, this condition is seven times more common in females than in males.
There has been an attempt to categorize WS into a congenital and an acquired form. The former results from a lack of development of the primary ligamentous attachments of the spleen; the association with additional congenital abnormalities such as renal agenesis, gastric volvulus, congenital diaphragmatic hernia, and Gaucher's disease suggests a related etiology between WS and these other abnormalities.3,4
The acquired form is typically diagnosed in adult women in the childbearing age and is thought to be caused by a laxity of these ligaments secondary to hormonal changes related to multiparity; this hormonal influence would explain the predominance of female cases in adults.
A triad of classic physical findings is traditionally associated with WS: palpation of a hard ovoid abdominal mass; painless movement of this mass toward the left hypochondrium, but limited in every other direction; and resonance to percussion in the left upper quadrant.
Laboratory tests are nonspecific, but may occasionally reveal evidence of hypersplenism or functional asplenia by the finding of Howell–Jolly bodies in peripheral blood smear. 5 Imaging findings are not unequivocal; owing to the abnormal mobility of the spleen, US or CT scans may fail the diagnosis when the spleen is found in its normal position. Abdominal US and Doppler sonography may rule out splenic torsion or ischemia by the finding of twisted vessels or absence of flow in the spleen; splenomegaly is a nonspecific sign and may occur secondary to congestion caused by kinking or torsion of the splenic vein. Eventually, the twisted splenic pedicle can mimic a bowel intussusception on CT scans. 6
Because of the threat of complications associated with a conservative treatment of WS, elective surgery should be considered strongly advisable, even for asymptomatic patients, once a diagnosis has been made. Although a splenectomy has been traditionally the preferred treatment and remains the most frequent option chosen in emergency, many surgeons now recommend preservation of the viable spleen, to avoid the septic and immunologic risks of splenectomy. Detorsion and splenopexy may be considered a reasonable surgical option even in patients presenting with acute abdominal pain, when there is no evidence of infarction or thrombosis. The recovery of splenic function in patients with evidence of significant ischemia supports aggressive salvage efforts.7,8
Several options for splenopexy through open surgery have been described in the literature; they include simple sutures between the splenic pedicle and diaphragm, colonic displacement, the use of an absorbable mesh wrapped around the spleen, and fixation of the spleen in a posterolateral extraperitoneal pocket. 9 In 1998, Hirose et al. reported the first case of pediatric laparoscopic splenopexy in a 2-year-old girl, in which the spleen was inserted into a mesh bag, which was then fixed to the left diaphragm. 10 Schmidt et al. reported that adhesion formation during mesh dissolution could be maintained long term (4-year follow-up). 11 In 2005, three different papers appeared in which splenopexy was obtained by creation of an extraperitoneal pocket either through blunt intraabdominal dissection 12 or via a balloon inserted through the 10th left intercostal space and filled with normal saline so that the left lateral peritoneum was dissected to create an appropriate pocket to accommodate the spleen.9,13
It is our feeling that creating a natural space into which the spleen can be accommodated is the best way to treat WS in the pediatric patient. The extraperitoneal pocket allows a definitive fixation of the spleen, avoiding the placement of a permanent mesh and the possible complications related to its use. Concerning the route through which the pocket is created, we believe that an expanding balloon inserted through the 10th intercostal space allows a safer and more expedite manoeuver, prevents possible tearing of the peritoneal edges, and is less prone to oozing from the diaphragmatic surface. Moreover, creating the pocket from the external surface of the body allows an immediate evaluation of the appropriateness of its diameters compared with those of the spleen. Nevertheless, even an accurately created pocket may prove inadequate to contain the spleen if splenomegaly is present because of the engorgement caused by its abnormal mobility and partial torsion of its pedicle. In those cases in which the spleen does not fit into the pocket, the addition of an absorbable mesh to the extraperitoneal pocket may be a simple trick to overcome the anatomic discrepancy.
Overall, patients undergoing splenopexy in the various series do very well with only 5% morbidity and no mortality. 14 The potential complications that occurred during or after surgery include splenic injury or infarction, recurrent torsions, and pneumothorax.
The combination of acute pancreatitits and gastric outlet obstruction as presenting symptoms of
Footnotes
Disclosure Statement
No competing financial interests exist.