
Abstract
Abstract
Introduction:
Although specimen extraction site selection for laparoscopic donor nephrectomy (LDN) is relatively flexible and is mostly selected by surgeons from the patient's standpoint, the patient's request may differ from the medical worker's recommendation. The cosmetic aspect may also differ with age, gender, and the extent of medical knowledge. We performed an unsigned questionnaire assessment of individual preferences for LDN wound sites.
Materials and Methods:
Between August 2007 and October 2008, we surveyed LDN wound site preferences among 148 physicians, 263 nurses, and 266 outpatients of urology at Akita University Hospital. They were questioned for their age, gender, occupation (medical worker or not), and for the most preferred surgical wound site among the following: A, lower vertical midline: B, upper vertical midline: C, anterior subcostal: D, Pfannenstiel: E, Gibson: and F, subcostal flank. The valid response rate was 93.5% (677/724).
Results:
Wound sites preferred (ranked in descending order) were F (48.3%), D (25.6%), E (10.5%), A (9.0%), C (5.2%), and B (1.4%). The subcostal flank incision was the most preferred in almost all the categories. Second preferences were Pfannenstiel incisions in women and incisions on the lower abdomen in men. Overall, flank and lower abdominal incisions tended to be preferred, and mid and upper abdominal incisions tended to be avoided. Medical workers selected the subcostal flank and Pfannenstiel incisions more frequently than outpatients. With increasing age, the selection rates of the Gibson and the lower vertical midline incisions increased, whereas the subcostal flank and the Pfannenstiel incisions decreased.
Conclusions:
The subcostal flank was the most preferred LDN sites. Age, gender, and the extent of medical knowledge may influence the individual preferences for LDN wound sites.
Introduction
Materials and Methods
Between August 2007 and October 2008, we surveyed of relative LDN wound site preferences among 148 physicians and 263 nurses working at Akita University Hospital, and 266 outpatients who visited urology clinics in the hospital. The subjects were aged between 18 and 75 years (mean 43.0±16.5). They were questioned for their age, gender, occupation (medical worker or not), and for the most preferred surgical wound site among the following: A, lower vertical midline incision: B, upper vertical midline incision: C, anterior subcostal incision: D, Pfannenstiel incision: E, Gibson incision: and F, subcostal flank incision (Fig. 1). The questionnaire in this study did not include the contents regarding the past history of abdominal surgery. We analyzed the questionnaire results according to gender, occupation, and generation (young, 18–35 years: middle, 36–55 years: and senior, 56–75 years). The valid response rate to the questionnaire was 93.5% (677/724). The mean ages of all subjects, medical workers (physicians and nurses), and outpatients were 44.8±18.3, 35.4±10.9, and 54.8±16.8 years, respectively. The ratios of man to woman in all subjects, medical workers, and outpatients were 276:401, 120:291, and 156:110, respectively. The protocol for the present study was approved by the Research Committee at our institute.

Scheme of the specimen extraction sites for living donor nephrectomy. The questionnaire including questions pertaining to age, gender, occupation (medical worker or not), and the most preferable surgical wound site among the followings:
Results
The most preferred wound sites were ranked in descending order as follows: F, subcostal flank incision (48.3%): D, Pfannenstiel incision (25.6%): E, Gibson incision (10.5%): A, lower vertical midline incision (9.0%): C, anterior subcostal incision (5.2%): and B, upper vertical midline incision (1.4%) (Fig. 2a-1). Overall, surgical wound sites on the flank and lower abdomen tended to be preferred, and those on the mid and upper abdomen tended to be avoided. The subcostal flank incision was the most preferred site in almost all categories (men, women, medical workers, and outpatients) (Fig. 2). The second preference sites were Pfannenstiel incisions in women and incisions on the lower abdomen in men (Fig. 2a-2, 3). Most medical workers selected the subcostal flank and the Pfannenstiel incisions, and most men preferentially selected the subcostal flank incision, whereas an equal number of women selected the subcostal flank and the Pfannenstiel incisions (Fig. 2b). Female outpatients preferred the Pfannenstiel incision next to the subcostal flank incision, whereas male outpatients selected various surgical wound sites (Fig. 2c-2, 3).
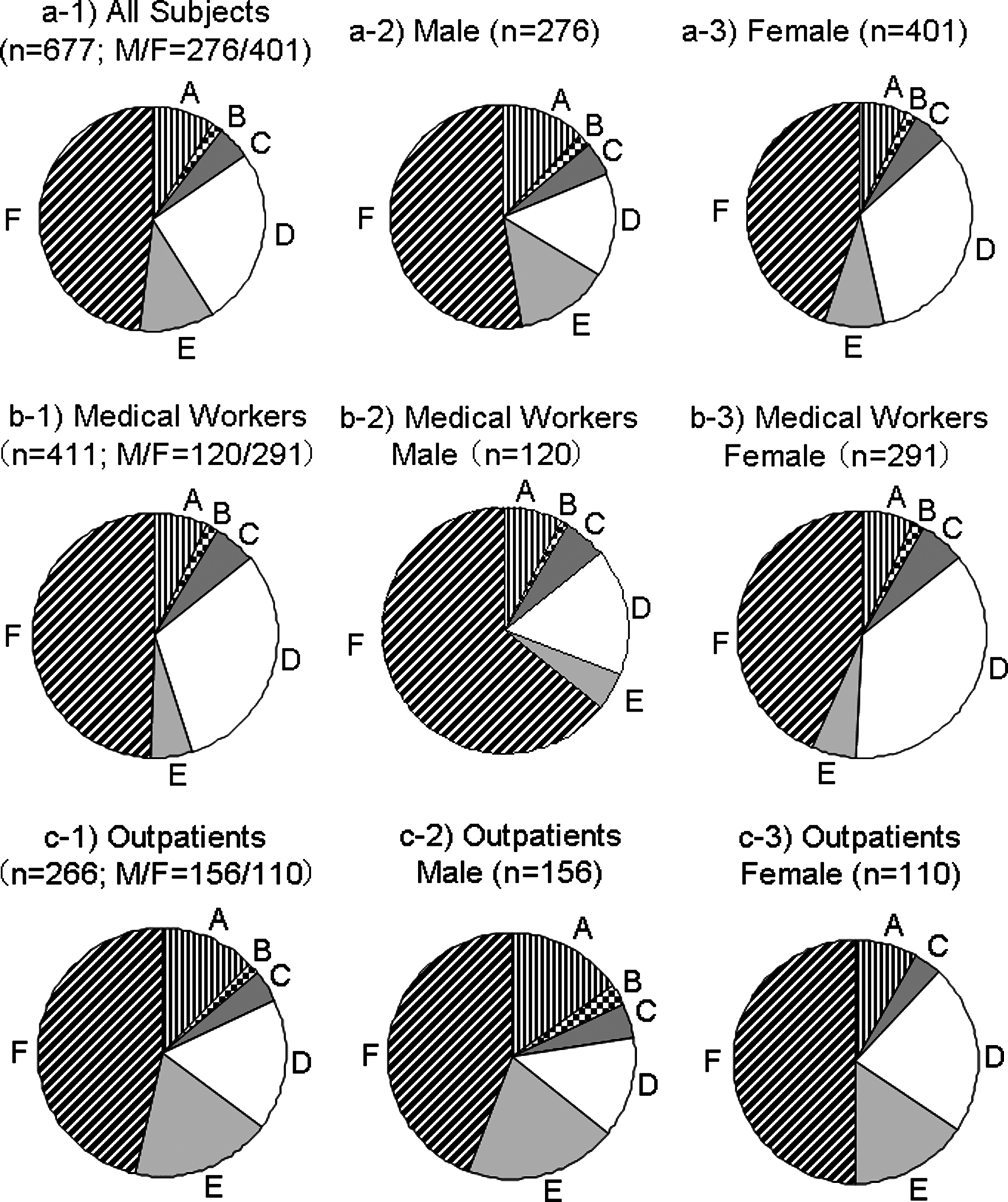
Preferable wound site ranking for living donor nephrectomy.
Comparing generations, the subcostal flank and the Pfannenstiel incisions were preferentially selected by the young generation (Fig. 3a-1). The selection rates of Gibson and the lower vertical midline incisions increased with age, whereas those of the subcostal flank and the Pfannenstiel incisions decreased (Fig 3a-1). In young and middle generations of overall and medical workers, a large number of women selected the Pfannenstiel incision as the most preferred site, whereas most men selected the subcostal flank incision (Fig. 3a-2, 3, 3b-2, 3). The selection rates of lower vertical midline and Gibson incisions in male and female outpatients, respectively, increased with age.
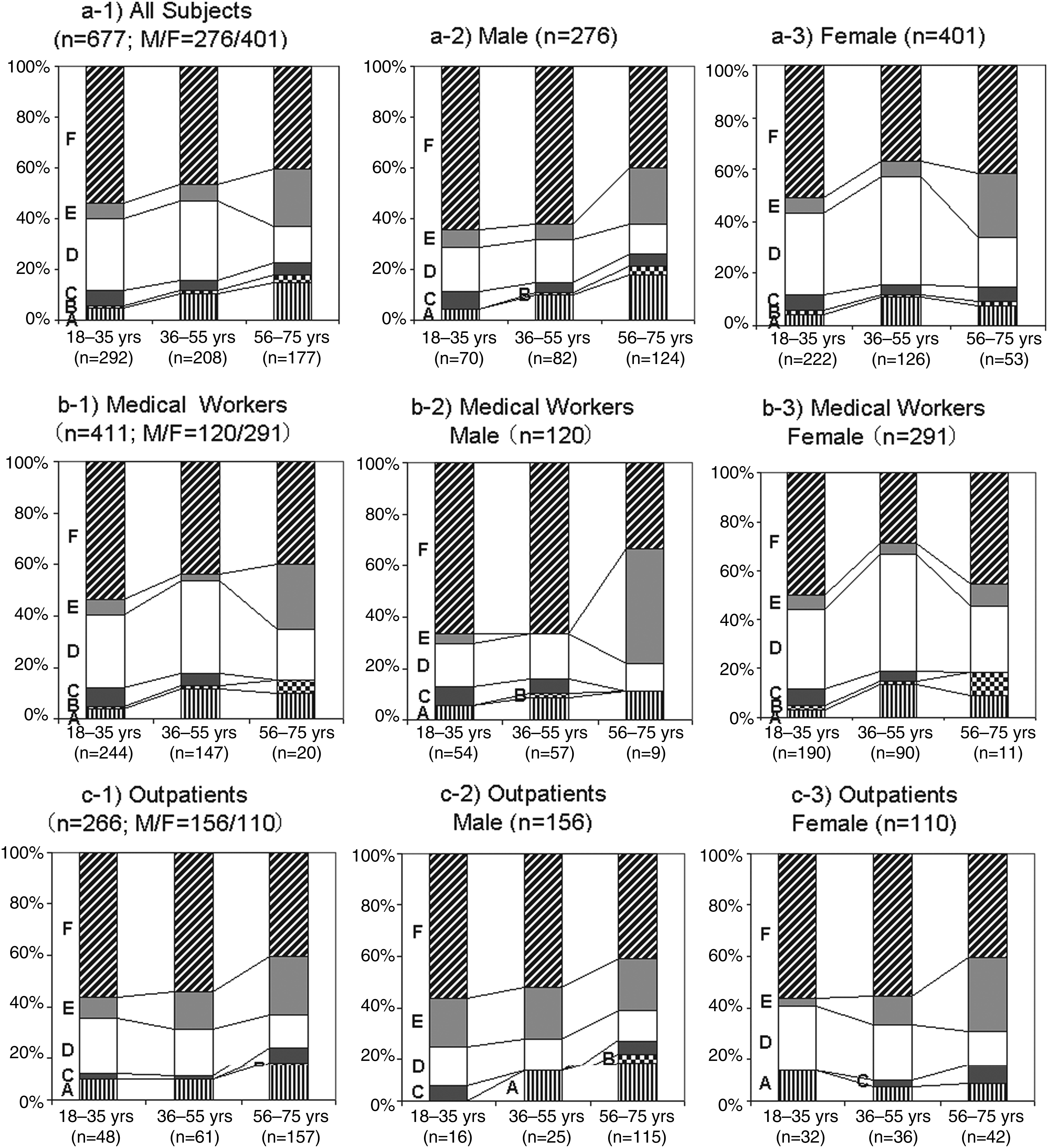
Preferable wound site ranking in different generations. Subjects were divided into three generations (young, 18–35 years: middle, 36–55 years: senior, 56–75 years). The type of the wound site is as described in Figure 1.
Discussion
Recently, LDN has been widely accepted for many kidney transplant protocols because of its minimal invasiveness and cosmetic perspective compared with open donor nephrectomy.4–7 The quality of life of the LDN donor is better than that of the open donor nephrectomy donor.7,8 In addition, in donor nephrectomy, an anterior vertical mini-incision is more preferred due to probable cosmetic satisfaction, reduced pain, and complications compared with an open flank incision.9,10 For these reasons, surgeons with sufficient laparoscopic or mini-incisional (endoscopic minilaparotomy) surgical skill should adapt their operative procedure to living donors. On the other hand, the specimen extraction site for LDN is relatively flexible. However, no discussion has been made regarding the most preferred LDN wound site for living donors.
In general, we recognize that patients, especially young women, prefer the Pfannenstiel incision also called the “bikini cut” when they undergo an abdominal operation. In this study, however, the subcostal flank incision was most preferentially selected in almost all categories, including young women. Overall, surgical wound sites on the flank and lower abdomen tended to be preferred, and those on the mid and upper abdomen tended to be avoided. We demonstrate a case of hand-assisted LDN at our institute in which the surgical wound scar on the lateral abdomen was almost invisible from the front (Fig. 4). The front view of the surgical wound scar may have strongly impacted the cosmetic aspect in this study. It remains unknown whether the preference for the subcostal flank incision in Japanese population holds true for Western or other ethnic populations.
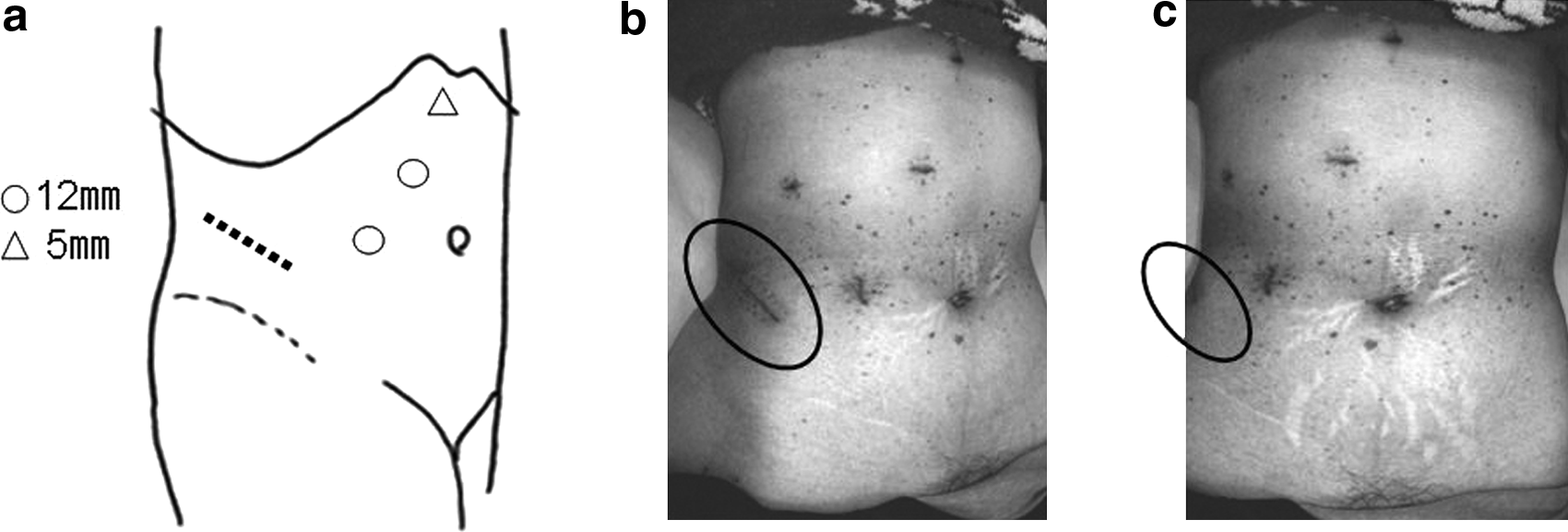
Scheme of port and extraction sites in laparoscopic right hand-assisted donor nephrectomy at our institute
The selection rate of the Pfannenstiel incision was about one-quarter, that is, second in the rank. Women selected the Pfannenstiel incision more often than men, and this incision was most supported by women in the middle generation. Most of the young generation selected the subcostal flank and the Pfannenstiel incisions, and the selection rates of surgical wound sites on the lower abdomen increased with age. Although medical workers selected the Pfannenstiel incision as the second preference, outpatients preferred surgical wound sites on the lower abdomen. The reasons why female medical workers selected the Pfannenstiel incision more preferentially than outpatient women are not clear. However, medical workers might know that the Pfannenstiel incision is generally associated with superior cosmesis and less pain. Generally, subjects in the general population do not have such knowledge regarding the superiority of the Pfannenstiel incision. In addition, senior people have a tendency to select a familiar surgical wound site, such as the Gibson and/or the lower vertical midline incisions. The difference observed in terms of wound site selection between male medical workers and outpatient men was influenced strongly by the age gap. Age, gender, and extent of medical knowledge influenced the selection of LDN wound sites.
Whether complication rates differ among surgical wound sites is controversial. Tisdale et al. compared the Pfannenstiel incision to expanded port site incisions (extending the inferior working 10-mm port sites lateral to the rectus abdominis muscle, transversely) as intact specimen extraction site during laparoscopic nephrectomy procedures. 11 They reported that the Pfannenstiel incision was less morbidity, because only one patient in the Pfannenstiel incision group developed cellulitis at the extraction site, whereas three patients in the expanded port site group developed incisional hernia. 11 However, it should be taken into consideration that all body mass indexes of these three patients were over 35. Bird et al. reported that in patients with a high body mass index using a paramedian extraction site at laparoscopic radical nephrectomy is a significant risk factor for incisional hernia formation. 12 Obesity may be a stronger factor of incisional hernia than the wound sites. Meanwhile, Gupta et al. reported that the iliac fossa incision (extending the spinoumblical port incision, close to Gibson incision) had less morbidity than the Pfannenstiel incision. 13 Gill et al. reported no difference in morbidity or recovery between the Gibson and the flank incisions for intact specimen extraction during laparoscopic nephrectomy procedures. 14 In a randomized study, surgical wound complication rates among midline, para-midline vertical, and transverse incisions were not different. 15 In addition, no randomized trial has been performed to investigate the difference in wound pain among surgical wound sites, and, therefore, further investigation will be needed. Although the subcostal flank incision may be associated with strong wound pain if the three muscle layers are divided, the muscle splitting technique will reduce wound pain and the wound hernia rate. 16
This study has the limitations that the results for outpatients who visited urology clinics in our hospital were regarded as general outpatient data, and subjects may feel less reality from the schemas of the wound position. In addition, subjects' responses may be affected by information about the degree of postoperative pain and the occurrence rates of nerve injury, muscle atrophy, and abdominal incisional hernia for each surgical wound site. Since this questionnaire provided no information regarding pain and complication rates for the different surgical wound sites, our questionnaire may be regarded as unbiased, and the subjects other than medical workers might have chosen the site of incision from the standpoint of pure cosmetic preference. As noted above, differences in complication rates among surgical wound sites have not been clarified.11–15 Although the present study indicated that the subcostal flank incision may be superior from the standpoint of cosmesis and patient preference, further randomized clinical study on a large scale is required to establish whether an incision made with a meticulous muscle splitting technique is associated with a lower complication rate and less wound pain than other incisions.
The quality of life of living donors may improve if they can select the surgical wound site themselves. A pure laparoscopic procedure does not limit the specimen extraction site, whereas hand-assisted LDN and/or mini-incision donor nephrectomy (endoscopic minilaparotomy) is comparatively limiting.
Conclusion
The subcostal flank incision was more preferred over the Pfannenstiel or other incisions as the specimen extraction site for LDN. Age, gender, and extent of medical knowledge influenced the selection of LDN wound sites. Further study is needed to establish whether subcostal incisions are associated with less morbidity, wound pain, good cosmesis, and patient preference.
Footnotes
Disclosure Statement
No competing financial interests exist.