
Abstract
Abstract
Background:
Sliding hernias are an uncommon type of inguinal hernia. Very little is published in the literature regarding the outcome of laparoscopic repair of sliding hernia. The present series evaluates the feasibility and outcome of laparoscopic repair of these hernias.
Methods:
Retrospective analysis of prospectively maintained data of patients with sliding inguinal hernia undergoing laparoscopic repair from January 2003 to July 2010 was done. The patient demographics, clinical presentations, operative details, and complications were studied. Related literature was reviewed.
Results:
A total of 1136 patients underwent laparoscopic repair of inguinal hernia, of which 54 patients had sliding inguinal hernia (4.7%). Forty-one patients (76%) had left-sided hernia and 13 patients (24%) had right-sided hernias. Mean age of presentation was 63.5 years. Thirty-five patients (64.8%) presented as complicated hernias (27 irreducible, 7 obstructed, and 1 strangulated). Thirty-nine patients had sigmoid colon, 9 patients had cecum, 3 patients had ascending colon, and 3 patients had urinary bladder as the sliding component. Eight patients underwent Lichtenstein repair, 27 patients transabdominal preperitoneal repair, and 19 patients total extraperitoneal repair. Mean operating time of laparoscopic repair was 53 minutes (40–105 minutes). Five procedures (10.8%) were converted to open repair. Overall morbidity was 44.4%. Median hospital stay was 1.5 days (1–14 days). There were no recurrences in up to 7 years follow-up.
Conclusion:
Laparoscopic repair of sliding inguinal hernia is feasible and safe with good outcome. Laparoscopic transabdominal preperitoneal approach is the preferable method.
Introduction
Materials and Methods
This study is a retrospective review of prospectively collected data of patients with sliding inguinal hernia who were operated during the period from January 2003 to July 2010 at ILS Hospital, Kolkata. The permission of the study was obtained by the head of the institute. All the procedures were performed by a single surgical team headed by the second author. The data maintained on Microsoft Office Excel were retrieved. The recorded parameters included patient demographics, operative details, and follow-up. Literature was searched using Medline with PubMed as search engine.
Patients undergoing laparoscopic repair were operated under general anesthesia (GA) after detailed preoperative workup to assess their fitness. The patients were put in supine reverse Trendelenberg position. Foley's catheter was inserted after induction of anesthesia. Reducibility of hernia was confirmed on operation table after induction of GA. Irreducible hernias were operated by transabdominal preperitoneal (TAPP) method, whereas reducible hernias were operated by total extraperitoneal (TEP) method. Third-generation injectable cephalosporin was given at induction of GA.
Technique of TAPP repair
The surgeon stood on right side of the patient irrespective of the side of hernia and the camera assistant at the head end. Monitor was kept at the foot end (Fig. 1). Pneumoperitoneum was created by a Veress needle puncture at the umbilicus. Insufflator pressure was set at 13 mmHg. A 10-mm optical trocar was inserted at the umbilicus and a 30° telescope was introduced. Right- and left-hand 5-mm working ports were inserted in midclavicular lines just below the level of the umbilicus on either side. The working port on the side of the hernia was at a higher position than the contralateral working port. The peritoneal cavity was inspected and the diagnosis of hernia was confirmed. Before labeling a hernia as sliding, it was confirmed that the content of the sac was actually forming a wall of the hernial sac and not merely adherent to it (Fig. 2).
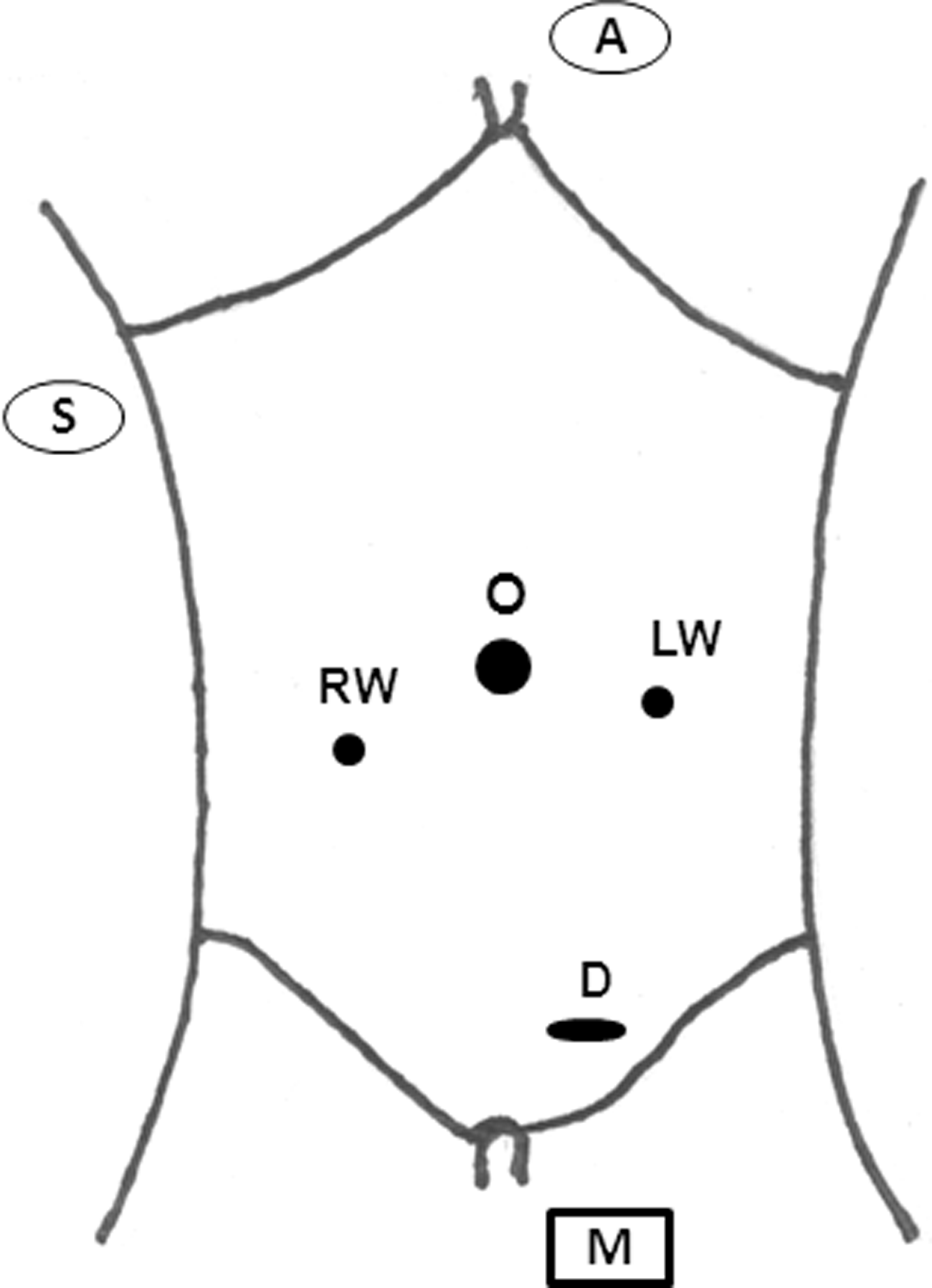
Port position and operation theatre setup. S, surgeon; A, camera assistant; M, monitor; D, defect; O, 10-mm optical port; RW, 5-mm right-hand working port; LW, 5-mm left-hand working port.
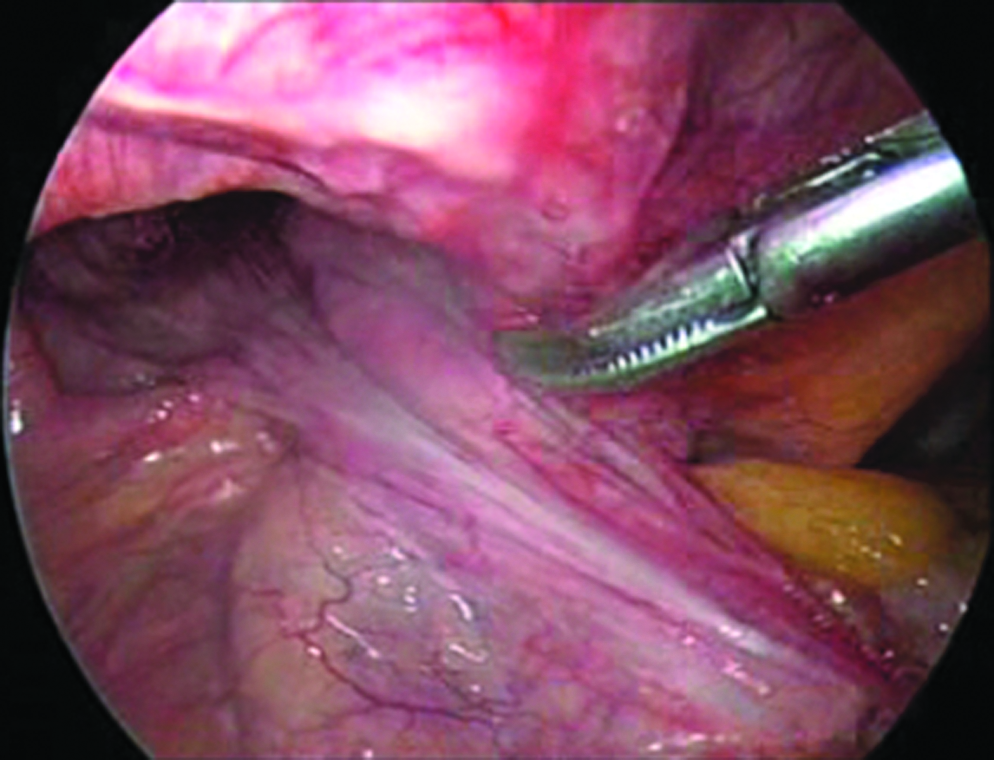
Transabdominal preperitoneal view of left sliding inguinal hernia.
The peritoneal flap was raised from anterior superior iliac spine up to the medial umbilical ligament about 2 cm above the deep inguinal ring using scissor with monopolar cautery. The medial fossa dissection was made across the midline to the opposite side and posterolaterally up to the obturator foramen. The lateral fossa was dissected up to the psoas muscle posteriorly. The hernia sac along with its contents was reduced and no attempt was made to free the sac from the sliding component. In case of difficulty in complete reduction of sac, it was divided beyond the level of its content. The deep inguinal ring was cut on the superolateral aspect using Ultracision to facilitate reduction of the contents. Complete parietalization of cord structures was done. Finally the superior peritoneal flap was raised. A 15 × 12 cm size polypropylene mesh was introduced and fixed with the help of helical tacks (Protack; Autosuture, Tyco Healthcare, United States Surgical, Norwalk, Connecticut) at Cooper's ligament and conjoined tendon making sure that the mesh was laid flat without folding. Reperitonealization was done using 2-0 polyglactin suture. The 10-mm port was closed with 1-0 polyglactin fascial sutures.
Technique of TEP repair
The access to the preperitoneal space was achieved via an infraumbilical vertical 11-mm incision just to the left of midline. The anterior rectus sheath was incised and the rectus muscle retracted laterally to expose the posterior rectus sheath. A bevelled tip 10-mm metallic cannula was inserted anterior to the posterior rectus sheath toward the symphysis pubis. The cannula was fixed to the skin using 1-0 mer silk suture after inserting a wet gauze piece into the wound to prevent leaking of CO2. The preperitoneal space was then insufflated with CO2 at 15 mm Hg pressure through the 10-mm cannula. A 10-mm zero-degree telescope was inserted and midline space dissected with the telescope. Right- and left-hand 5-mm working ports were introduced in para-rectal position in spino-umbilical line so as to achieve triangulation at the hernial site. Now, the telescope was replaced with 10-mm 30-degree telescope for the remaining procedure. After medial and lateral fossa dissection, the sac was opened in cases when it was found to be thick, either to confirm or exclude the sliding nature of hernia (Fig. 3). After complete reduction of the hernial sac, the opening was closed with 2-0 polyglactin sutures. The remaining steps were similar to the TAPP repair.
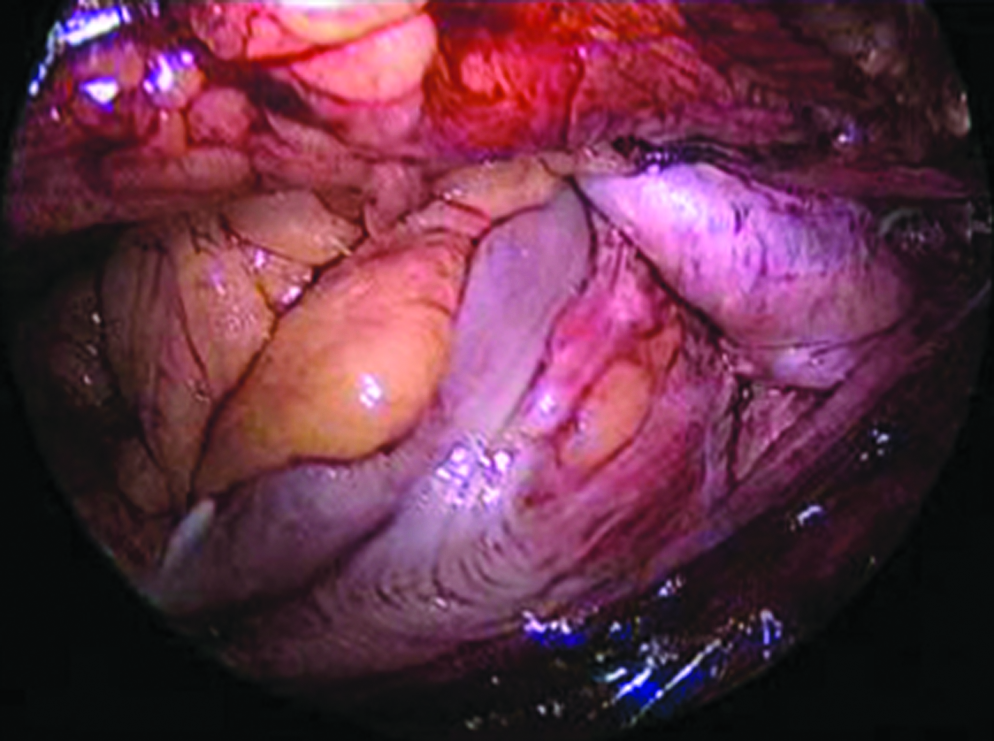
Total extraperitoneal view of sigmoid colon as sliding component.
After the procedure, compression dressing was applied for 3 days. Foley's catheter was removed on the next morning and the patient discharged after voluntary voiding of urine. The patients were followed up at 1 week, 6 months, 1 year, and 2 years as per routine protocol. Patients were again contacted at the time of study. The last three follow-ups were made by telephonic conversation.
Results
From January 2003 to July 2010, 1136 patients of inguinal hernias were operated at ILS Hospital, Kolkata. Of these, 54 patients (4.7%) had sliding inguinal hernia. All the patients with sliding hernia were male. The mean age of the entire hernia group was 54.7 years, whereas the mean age of patients with sliding hernia was 63.5 years (range: 38–86 years). Of 54 sliding hernias, 41 hernias were on left side (76%), 13 hernias were on right side (24%), and 5 sliding hernias were part of bilateral hernias. The most common presentation was swelling with or without pain in the groin. The mean duration of symptoms was 6.5 months. Seven patients presented with intestinal obstruction and 1 patient had strangulated hernia. Twenty-seven patients had irreducible or partially reducible hernias (Table 1). Thus, only 19 patients (35%) presented with reducible hernias. Four patients (7.4%) presented as recurrent hernias. Patients with intestinal obstruction and strangulation (n = 8) were operated in emergency by anterior approach, whereas the remaining 46 hernias (85%) were repaired laparoscopically. Of these, 27 hernias were repaired by TAPP method and 19 hernias by TEP method. The laparoscopic procedure was completed in 41 patients, whereas five procedures (three TAPP, two TEP) were converted to anterior Lichtenstein repair because of difficulty in reducing the sac in complete inguinoscrotal sliding hernias. The conversion rate was thus 10.8%.
Of 54 sliding hernias, 39 hernias had sigmoid colon, 9 hernias had cecum, 3 hernias contained ascending colon, and 3 hernias had urinary bladder as the sliding component. Fifty-three patients had indirect hernias and 1 patient had direct hernia with urinary bladder as the sliding component. There were no patients with bilateral sliding hernias. Five patients had bilateral inguinal hernias with sliding hernia on one side and nonsliding hernia on the opposite side. The mean operating time was 53 minutes (range: 40–105 minutes). Six patients (12.2%) had minor bleeding from cord vessels or branches of inferior epigastric vessels. There were no access related injuries, viscus injuries, or injuries to great vessels. Thirteen patients (24%) had urine retention and 5 patients (9.2%) had seroma formation. None of the patients had port-site infection or chronic groin pain. The median hospital stay was 1.5 days (range: 1–14 days) (Table 2).
All the patients had 1 week and 6 months follow-up. Forty-eight patients (88.8%) had 1-year follow-up and 45 patients (83.3%) had 2-year follow-up. Thirty-eight patients (70.3%) were followed up at the time of study. There were no recurrences in the maximum follow-up period of 7 years.
Discussion
Although the literature is replete with volumes of articles on inguinal hernia, very little has been published on sliding hernias. The open techniques for inguinal hernia repair were first described by Bassini 3 and later modified by Halsted 4 and others. Cheatle first introduced the concept of preperitoneal placement of mesh for inguinal hernia repair. 5 Lichtenstein in 1989 described the tension-free hernioplasty using prosthetic mesh via anterior approach. 6 The earliest report of endoscopic hernia repair came in 1982 when Ger described a series of 12 cases of laparoscopic application of metal clips at the hernia neck. 7 However, it was not until 1991, when Arregui reported TAPP technique for inguinal hernia repair that the laparoscopic technique got acceptance. 8 McKernan and Dulucq9,10 are credited with first TEP repair. Throughout this magnificent saga of advancement of the hernia repair techniques, sliding inguinal hernias have puzzled the surgeons of all times. This is due to the fact that very little is known about their pathogenesis, they pose great peroperative difficulties, and they are associated with higher recurrence rates. 11
Bendavid 1 classified sliding hernias into three types. Type I (95%) is the commonest, where a part of sac is formed by the wall of viscus. In type II (5%), mesentery of the viscus forms a part of the peritoneal sac. Type III is extremely rare and occurs when the viscus itself protrudes without a peritoneal sac. The pathophysiology and the mechanism of “sliding” of viscus have not been clearly explained. However, as described by Bendavid, the common initial factor is always the widened deep inguinal ring.
In our series, of 1136 patients of inguinal hernia, 54 patients had sliding hernias, with incidence being 4.7%. This is less than the 8% reported by Ryan 12 and Welsh 13 and more than the recent series by Adams, who reported the incidence to be 2.9%. 11 Left-sided hernias were 3.1 times more common than right-sided hernias. Ryan reported that 8% patients had bilateral sliding hernias. However, our series has 5 patients of bilateral hernia who had sliding hernia on one side and nonsliding hernia on the opposite side. There were no patients with bilateral sliding hernias.
Bendavid 1 in his review article on sliding hernias pointed out that the incidence increases with age. This is substantiated in our study where the mean age of patients is 63.5 years. The report also indicated that 94% of sliders are easily reducible preoperatively. In striking contrast, 35 patients in our series (64.8%) had complicated hernias (27 irreducible, 7 obstructed, and 1 strangulated) and only 19 patients (35.1%) had reducible hernias. This may be due to higher referral of complicated cases to the institute and a fair possibility of missing unsuspected reducible sliding hernias where the peritoneal sac was not opened during TEP repair. However, this finding is still comparable to the study by Gasper et al. 14 of 52 sliding hernias, where 46.2% of hernias were reducible.
The repair of sliding hernias has been challenging because of difficulty in reducing the sliding component, and hence, various types of repairs have been reported. Last century witnessed the division of surgeons into two groups. One group was proponent of the inguinal approach and the other group advocated a combined “inguino-abdominal” approach.
The abdominal approach for the repair of sliding inguinal hernia was first reported by Fiaschi in 1907 as reported by Koontz. 15 In 1932, La Rouque described muscle splitting incision above the deep inguinal ring for sliding hernias. 16 This technique got a wide acceptance in the surgical fraternity. The inguinal approach included the “high purse-string” closure of the sac described by Sensenig and Nichols. 17 Bevan 18 in 1930 also suggested the idea of reperitonealization of the viscus of sliding hernia. However, these techniques were associated with high recurrence rates. In the landmark report on 313 patients of sliding inguinal hernia, Ryan in 1956 reported only four recurrences by inguinal approach. 12
In the 21st century, it appears that combined “inguino-abdominal” technique is considered unnecessary as mentioned by Bendavid. 1 He opines that the reports of Ryan are convincing enough to establish the inguinal approach as the standard technique. However, despite being published in 2002, Bendavid's report did not discuss the scope of laparoscopic repair of inguinal hernia, which was well described then.
There are innumerable references on the techniques of laparoscopic repair of inguinal hernia. Surprisingly, however, very little has been written on the feasibility and fate of laparoscopic repair of, not so rare sliding hernias. The present series is perhaps the only study committed to assess the outcome of laparoscopic repair of sliding inguinal hernia.
As well documented, two techniques are described for laparoscopic repair of inguinal hernias. Overall, TEP technique is the favored approach as it avoids the violation of peritoneal cavity, thereby reducing the incidence of access related and viscus injuries. With reference to sliding hernia, however, the authors are of the opinion that TAPP approach is more appropriate. The reason is because the diagnosis of sliding hernia is possible only after opening the peritoneal sac and confirming that the viscus actually forms the wall of the sac. Hence, sliding hernias may be missed during TEP repair as the sac is not opened routinely. Second, sliding hernias more frequently present with irreducibility and pose great difficulty in reduction of the sac. The reduction of the sac is easier by TAPP approach than TEP. Dulucq in 2009 mentioned that TAPP has been advocated for complicated hernias including sliding or incarcerated inguinal hernias. 2
Of late, there have been case reports of laparoscopic repair of irreducible sliding hernias.19,20 A recent study by Roy and De 21 described the technique of single-incision laparoscopic TAPP mesh hernioplasty in 15 patients for inguinal hernia. Two patients in their study had left-sided sliding hernia with sigmoid colon as the content. No recurrence was reported till 3-month follow-up. These reports support the feasibility of laparoscopic techniques for repair of sliding hernia and indicate towards their ever-increasing scope. Although the repair of sliding hernias has been controversial in the last century, the dawn of 21st century has come with a possible final answer in the form of laparoscopic TAPP technique for the repair of this fascinating surgical entity. More publications are required to further establish this technique as the method of choice for repair of sliding hernias.
Conclusion
Sliding hernias are a “neglected” variety of inguinal hernias with distinct pathophysiology usually affecting elderly males. These hernias are more common on the left side and present with complications of irreducibility, obstruction, and strangulation more frequently. Laparoscopic repair of sliding inguinal hernias is feasible and safe with impressive results. TAPP approach is preferred over TEP approach as it allows better identification of these hernias and offers easier method of sac reduction.
Footnotes
Disclosure Statement
No competing financial interests exist.