
Abstract
Abstract
Objective:
One of the most significant limitations of laparoscopic surgery is the inability to achieve tactile assessment of structures during surgical dissection. Because blood vessels are naturally warmer than their surroundings, infrared (IR) detection can be highly effective in identifying and mapping out their course. In recent years, IR detection has been used successfully for this purpose in open surgery. Nevertheless, this technology has to be yet employed in laparoscopic surgery, where its contribution would be greatest.
Methods:
We performed a feasibility study using this technology on live porcine models. After insertion of IR detectors into the insufflated abdomen, we performed a series of laparoscopic procedures. During these operations we evaluated the ability of the IR detector to identify blood vessels as well as the effects of local and systemic changes in temperature.
Results:
The IR detector successfully identified concealed blood vessels as well as acute bleeding. Cool lavage and insufflation with room-temperature CO2 accentuated IR detection of blood vessels, whereas warm CO2 and systemic temperature changes did not affect detection. Additionally, localized heating of tissue on the operative field using electrocautery did not interfere with IR sensitivity.
Conclusion:
Laparoscopic IR imaging is a feasible method of blood vessel detection in laparoscopic procedures. Use of IR blood vessel detection in laparoscopy has a potential to enable safer surgery and reduce operative time. Fusion of IR imaging with the standard laparoscopic view is currently being developed to allow real-time vessel mapping during laparoscopic procedures.
Introduction
In 2004, the concept of performing abdominal surgery without abdominal wall incision was introduced, an idea to be given later the name “natural orifice transluminal endoscopic surgery” (NOTES). 1 The purpose of NOTES was to maximize the minimal invasiveness of laparoscopic surgery and reduce incision-related complications. 2 After only 5 years since the first publication on the topic, interest in the field has been growing by leaps and bounds. Many surgeons are now gaining experience in performing cholecystectomy, splenectomy, oophorectomy, small bowel resection and anastomosis, and other various operations via NOTES in both human and animal models.3–10 To date, the institutions that have introduced this approach use it mostly to perform cholecystectomy and appendectomy.
Single-incision laparoscopic surgery (SILS) is another technique that has been introduced during the last few years, which has become increasingly popular and represents the further progression of minimally invasive surgery. This progression emphasizes the current technical obstacles in this field, as discussed earlier. To perform SILS and NOTES safely, we must overcome these technical difficulties.
Visible light is an electromagnetic radiation with wavelengths of 0.4–0.7 μm. Infrared (IR) radiation is composed of electromagnetic waves with a lower frequency and longer wavelength (longer than 0.7 μm). 11 Several types of IR light are stratified according to their wavelength range and physical properties. One of these types, long-wave IR (LWIR) has a wavelength range of 8–15 μm and is emitted from warm objects. The intensity of radiation and its wavelength depend on both the object's temperature and its emissivity. 11 For example, the LWIR wavelength emitted from a normal human body is 10 μm. 12 Hence, IR detectors sensitive to LWIR may provide thermal imaging, which is referred to as “thermography.”
The idea to use thermography in surgery is based on the relative warmth of blood vessels, which may provide a real-time vascular map. Such a map, if projected on a visible view of the operative field, may provide improved capability to dissect vessels in a quick and efficient manner. Despite this significant potential advantage, to date the application of thermography in surgery is very limited. Thermography has been used in vascular surgery to corroborate perfusion in coronary bypasses and in intracranial vessels.13,14 It was also used experimentally in laparoscopic surgical procedures, but the inability of IR radiation to penetrate glass lenses and the large size of IR detectors resulted in impaired IR images.15,16 Unfortunately, an IR detector small enough to enter the abdominal cavity through a standard laparoscopy trocar was not yet developed, but with the progress of technology such a development is anticipated. Another uncertainty is whether temperature differences between blood vessels and their surroundings still exist within the closed abdominal cavity, where no heat is lost to ambient temperatures.
Herein, we investigated these uncertainties with the goal of developing a novel IR imaging system.
Methods
The purpose of this study was to evaluate the feasibility of laparoscopic thermography and to define methods for enhancement of the differences between blood vessels and their surroundings as they appear in the IR images.
Following the approval from our Institutional Animal Care and Use Committee, the study was conducted on 3 farm pigs weighing 35–40 kg under the supervision of a qualified veterinarian. Prior to the operation the animals were sedated using intramuscular xylazine (2 mg/kg body weight) and ketamine (15 mg/kg body weight). In the operating room, general anesthesia with intravenous propofol (2–5 mg/kg body weight) was induced and the animals were intubated and mechanically ventilated. Anesthesia was maintained throughout the procedure with inhalational isoflurane (1%–4%). The animals received intravenous isotonic solution throughout the procedure and were monitored with pulse oxymetry, end tidal CO2 measurements, and electrocardiography.
The animal was positioned in a supine position, and a 12-mm skin incision was performed, through which a 12-mm trocar (Excel® trocar; Ethicon Endo-Surgery) was introduced into the abdominal cavity. A CO2 insufflation system (SOB electronic endoflator; Storz Endoscopy) was connected to the trocar and pneumoperitoneum was induced to a pressure of 15 mmHg. Two to three additional trocars were introduced and an additional 7-cm-long abdominal wall incision was performed at the midline. Through this incision, a thermogrphic imaging device (Meron™ thermographic detector; Opgal Optronic Industries) was introduced into the peritoneal cavity (Fig. 1). This device is a passive IR detector with a spectral range of 8–14 μm, a resolution of 384 over 288 pixels, and a rate of 50 frames per second. Its dimensions are 61×61×90 mm. The peritoneal cavity was explored with both a standard laparoscope and the thermographic detector and blood vessels were identified. Various intraperitoneal temperature challenges were performed: (1) insufflation with warm and cool CO2, (2) warm and cool lavage of the operative field, and (3) application of monopolar diathermy to abdominal organs. Systemic temperature changes were attempted using warm and cool intravenous isotonic solutions. Changes in the thermographic images in response to those temperature challenges were recorded. All procedures were terminal and following them the animals were euthanized using intravenous pentothal (130 mg/kg body weight).

The Meron infrared (IR) detector
Results
At the beginning of each procedure, exploration of the peritoneal cavity was performed and abdominal organs were videotaped with a standard laparoscope and the IR detector simultaneously. There were noted differences in the appearance of the liver, spleen, stomach, small and large bowel, and mesentery in IR images. Vascular structures including mesenteric vessels, gastroepiploic artery, short gastric arteries, etc., appeared brighter than their surroundings (Figs. 2 and 3). In one of the operations, an arterial bleeding from the splenic artery was initiated. The IR detector easily pinpointed the exact point of bleeding despite pooling of extravascular blood in its surroundings (Fig. 4).

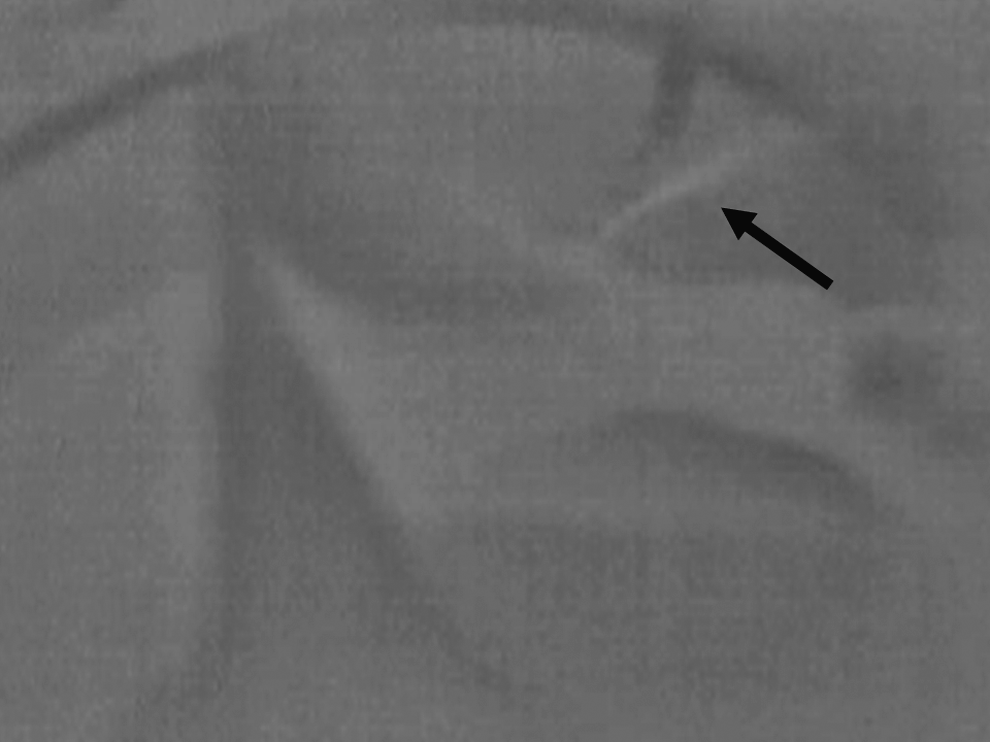
Laparoscopic thermographic view of the stomach. The right gastroepiploic artery is seen brighter than its surroundings (black arrow). The dark area on the upper part of the figure (white arrow) represents a jet cool insuflation gas hitting the tissue.
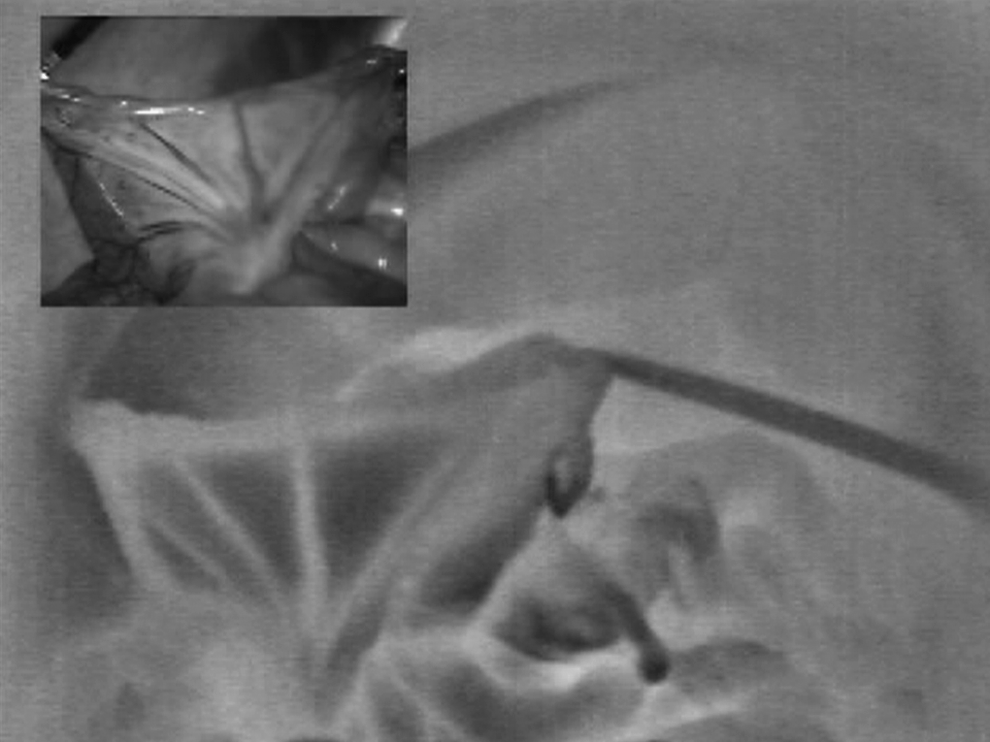
Laparoscopic visible (inset) and IR (large picture) simultaneous views of a small bowel loop. Notice the bright vessels at the mesentery.
Splenic arterial bleeding (arrow) as seen with thermography. The bright area in the middle represents accumulation of blood, which is warmer than the surrounding organs.
Insufflation with warm CO2 was achieved with Storz Endoscopy thermoflator and additional heating of the gas through a hose soaked in 70°C water. Warm insufflation did not result in any change of the thermographic images. Room-temperature CO2 insufflation (which is cooler than the pig's body temperature of 38–39°C), on the other hand, resulted in images containing cooler (darker) zones than their surroundings (Fig. 2).
Room-temperature saline lavage of the operative field resulted in cooling and darkening of the acquired thermographic images. Soon after, vessels in the operative field were accentuated as vascular flow induced their rewarming relatively to their surrounding (Fig. 5). The rest of the dark area cleared much more slowly than the vessels. Warm saline lavage (45°C) of the abdomen resulted in immediate warming and brightening of the operative field, resulting in the obscuring of vessels. Graduate and slow cooling following warm lavage returned the ability to identify vessels after only 30 seconds.
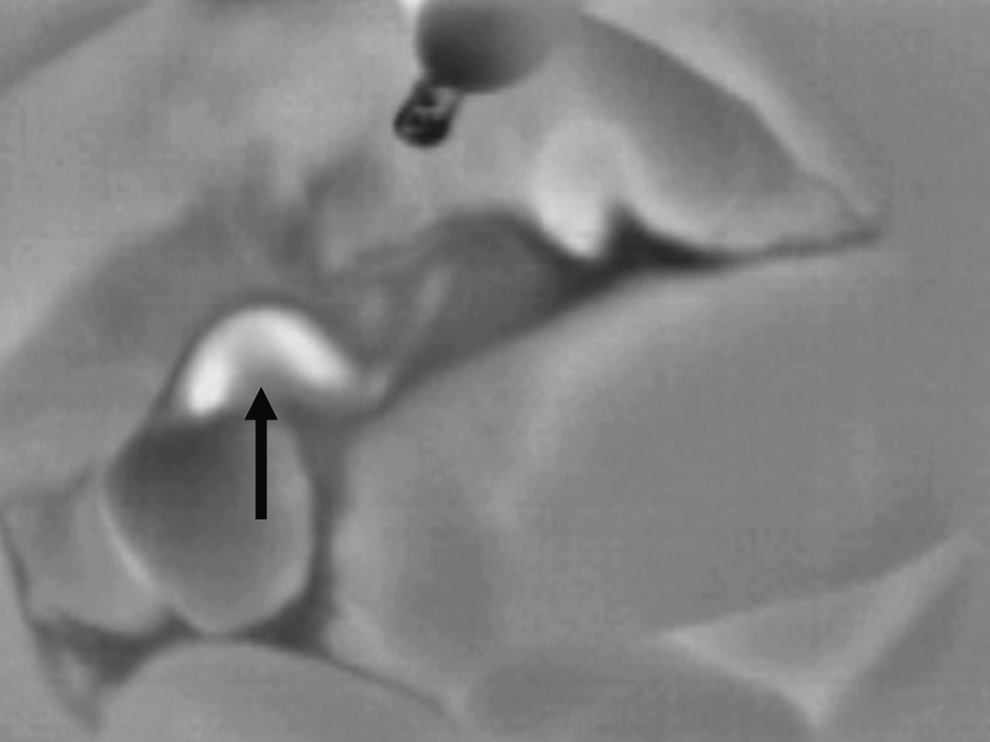
The right gastroepiploic artery (arrow) on the background of room-temperature isotonic saline solution. The cool lavage enhances the thermographic difference between the vessel and its surroundings.
Application of monopolar diathermy on intra-abdominal organs caused immediate appearance of a warm, bright localized area on thermography. This spot did not return to its original brightness for several minutes, including after cool saline lavages (Fig. 6). The area of warming, however, spanned to about 1 cm radius only and did not affect the appearance of nearby structures.
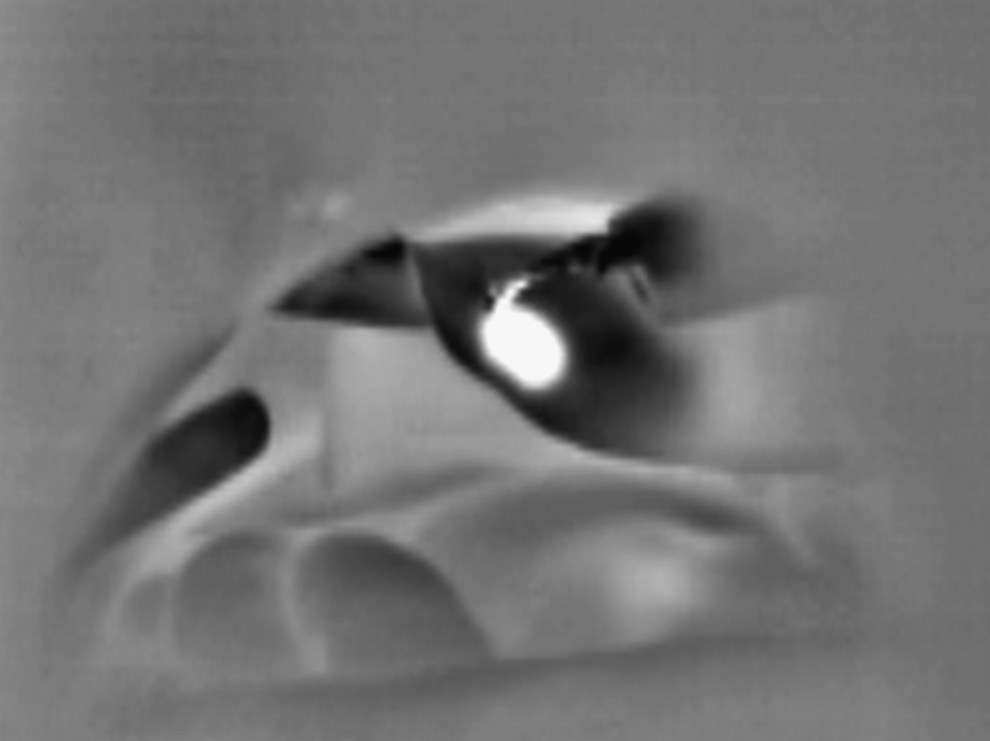
Application of monopolar diathermy on the liver causes a bright, round, well-demarcated area on thermography, which is enhanced by the jet of cool insufflation gas coming from the trocar.
Intravenous administration of cool (4°C) isotonic saline solution did not result in any temperature change, as could be seen on thermography. Each animal received about 500 mL of cool solution until bradyarrhythmia has developed; hence, its administration was stopped. Intravenous administration of 1000 mL of warm (45°C) isotonic saline solution also did not result in any thermographic changes.
Discussion
The expected advantages of thermography use for the detection of blood vessels and other critical structures during laparoscopic surgery are significant. They can be expected to be of extreme importance in laparscoscopic surgery in general and in NOTES and SILS, where the view is compromised, in particular. Nevertheless, this technique has two major pitfalls that have prevented its wide application in clinical practice. The first pitfall is the inability of IR waves to pass through glass lenses together with the large-diameter IR detectors. Under these conditions, laparoscopic use of IR detectors is not feasible. The second pitfall is the inability to perform surgery based solely on IR imaging. A computer-based real-time merging of the IR and visible views is necessary. This study represents a feasibility study for the use of thermography in laparoscopy. It was performed as a preliminary step for the development of system, which will enable improved real-time laparoscopic IR view. We have shown that laparoscopic IR imaging is feasible and of significant potential advantage. We have also demonstrated that several maneuvers such as cool lavage and cool insufflation might enhance the blood vessels' thermographic appearance. According to these findings, the utilization of an insufflator, which will continuously administer cool CO2 and simultaneously evacuate it, will be of use for the improved detection of blood vessels in thermography-assisted laparoscopic surgery.
The application of monopolar diathermy causes immediate local heating and does not influence the thermographic view elsewhere. The use of diathermy, therefore, is not an obstacle for the utilization of thermography. Active bleeding is well recognized by thermography, which might improve the ability to localize the exact origin of bleeding within an obscured operative field full of blood and clots.
Finally, we have demonstrated that in contrast to local temperature changes, systemic temperature changes do not change the thermographic view and do not exclude the use of this technology.
The main difficulties encountered were to align the laparoscopic view together with the IR view. In this study the laparoscope and IR camera were inserted in different ports and thereby operated separately and viewed on two different monitors or via picture-in-picture mode. Alignment, focus, and zoom were needed to be performed separately to reach the same field of vision.
Improved visibility is expected with the use of color in the IR image; however, the IR measurements are needed just to identify the vessels' location. Future ability to display the IR view on top of the laparoscopic view with the use of software enhancement will enable color display following calculations of temperature ranges.
The use of other technologies for vessel detection, for example, ultrasound Doppler, is feasible. Nevertheless, ultrasound for vessel detection mandates direct contact of the probe to the organs. Because of the fact that in laparoscopy the peritoneal cavity is inflated with CO2 gas, probes placed on the abdomen will not be useful and ones placed within the abdominal cavity will obstruct the laparoscopic view. In addition, real-time merging of the laparoscopic view and the ultrasound images does not seem to be feasible, in contrast to the merge of the IR and laparoscopic views.
There is concern regarding the feasibility of laparoscopic thermography in humans, where there is increased intra-abdominal adiposity. To deal with that concern, we performed a simple procedure and dissected porcine femoral vessels under thermographic guidance. Thermographic view of these vessels was obtained clearly through the skin. After dissection was completed, the vessels' depth of 5 mm was recorded and hence the assumption that depth of thermographic tissue penetration equals or is larger than 5 mm, meaning that intra-abdominal thermography should be feasible in most nonobese human patients.
Conclusion
In this study we have investigated the use of thermography in laparoscopic surgery. We have shown that the use of thermography for the detection of blood vessels during laparoscopic surgery is feasible and is subject to several methods of local temperature changes.
According to our findings, there is place to develop laparoscopic thermographic systems, which will overcome the obstacles of detector size and the need for real-time merging of the IR and visible views. Such a system will enhance our ability to detect blood vessels intraoperatively, especially in surgeries with compromised views such as NOTES and SILS surgeries. As technology progresses, it can be expected that it will not be long before the aforementioned obstacles can be overcome and thermographic imaging can be readily employed in clinical use.
Footnotes
Disclosure Statement
Drs. N. Shussman, M.A. Gazala, A. Schlager, R. Elazary, A. Khalaileh, and G. Zamir, Mr. D. Kushnir, and Prof. A.I. Rivkind have no conflicts of interest or financial ties to disclose. Dr. Y. Mintz is a consultant to Easylap, EasyNotes, and Silenseed and has received educational grants from Ethicon Endosurgery and Storz Endoscopy.