
Abstract
Abstract
Background:
With the evolution of surgical techniques and instrumentation, surgeons have adapted methods to provide safe and effective therapy through less invasive operations. Conventional laparoscopy utilizes several small incisions in well-separated areas of the body, but more recently, surgeons have been performing minimally invasive procedures through a single incision. Specially designed ports and instruments have been employed to offset the disadvantage of losing the ability to have instruments separated in space while working through a single incision. We have reviewed our initial experience with single-incision laparoscopic cholecystectomy (SILC) in children using conventional straight laparoscopic instruments compared with those who underwent standard laparoscopic cholecystectomy (SLC).
Methods:
During the study period, a retrospective chart review was performed on 54 consecutive children who underwent laparoscopic cholecystectomy. Twenty-seven patients who underwent SILC (1 patient had splenectomy with cholecystectomy) were compared with 27 patients who underwent SLC by a single pediatric surgeon. Outcomes measured included successful completion rate, operative time, length of hospital stay, blood loss, and postoperative complications.
Results:
Fifty-four cholecystectomies were performed laparoscopically with no conversions to open. In the SILC group, 24 of 27 (89%) were successfully completed. Two patients required one additional trocar/incision (laparoscopic splenectomy with cholecystectomy) and another two additional trocars/incisions to complete the procedure. Operative time was longer in the SILC group than in the SLC group (116 versus 61 minutes; P value <.0001). Two umbilical wound infections occurred in the SILC group (7.4%) and 1 patient in the SLC group developed postoperative choledocholithiasis.
Conclusions:
In our experience, SILC in children using standard straight laparoscopic instruments is a safe and effective alternative to conventional four-incision laparoscopic cholecystectomy. This technique, although safe, may lead to longer operative times since there is a loss of instrument triangulation provided with SLC or use of articulating instruments.
Introduction
Methods
This study was approved by the University of Pittsburgh institutional review board where from March 2009 to April 2010, data from 54 consecutive patients who underwent laparoscopic cholecystectomy by a single surgeon were retrospectively reviewed. There were 27 patients who underwent SILC and 27 patients who underwent SLC. All procedures were performed at the Children's Hospital of Pittsburgh. The majority of patients undergoing SILC were performed during the latter part of the series and informed consent was obtained from every patient. The operative procedure was initiated by making a 1–2 cm incision concealed in the base or vertically through the umbilicus (depending upon the size of the child). Pneumoperitoneum was achieved in all cases by insertion of a Veress needle through the area of the umbilical stalk, which was removed. Next, either a SILS Port™ (Covidien, Norwalk, CT) was placed in 5 patients, or, more often, three individual 5.5 mm ports (Covidien) were placed through separate fascial incisions at the 2, 6, and 10 o'clock positions to perform the procedure as shown in Figure 1. Conventional 5 mm angulated (30° or 45°) laparoscope of standard length, Maryland dissector or duckbill grasping instrument, and an L-hook electrocautery device (Fig. 2) were used in all cases. In nine cases, one or two transabdominal sutures (2-0 PDS; Ethicon, Cincinnati, OH) were placed directly through the abdominal wall in right subcostal area and then through the gallbladder fundus and/or infundibulum. These sutures were used routinely in younger patients earlier in the series but were not considered standard. To achieve adequate exposure and retraction of the gallbladder-cystic duct junction most effectively, we found that placing the transabdominal suture through the infundibulum twice (while grasping the gallbladder dome) allowed for back–and-forth retraction on the external suture. Thus, the critical view of safety could be reliably obtained. In three larger patients, instead of using retraction sutures, a 2-mm Mini-Lap Alligator grasper (Stryker Endoscopy, San Jose, CA) was used through a separate stab incision in the umbilicus (1) or right upper quadrant (2) as the safer option to achieve adequate gallbladder retraction.
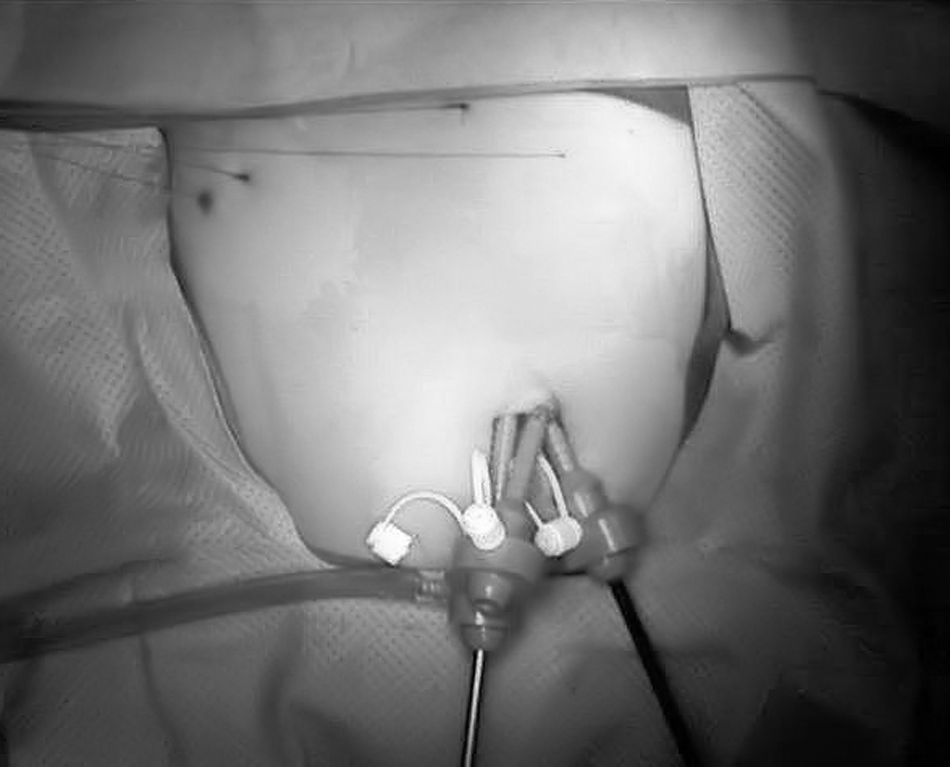
External view of the three port technique through the umbilicus with additional retraction sutures through the abdominal wall in a 10-year-old.
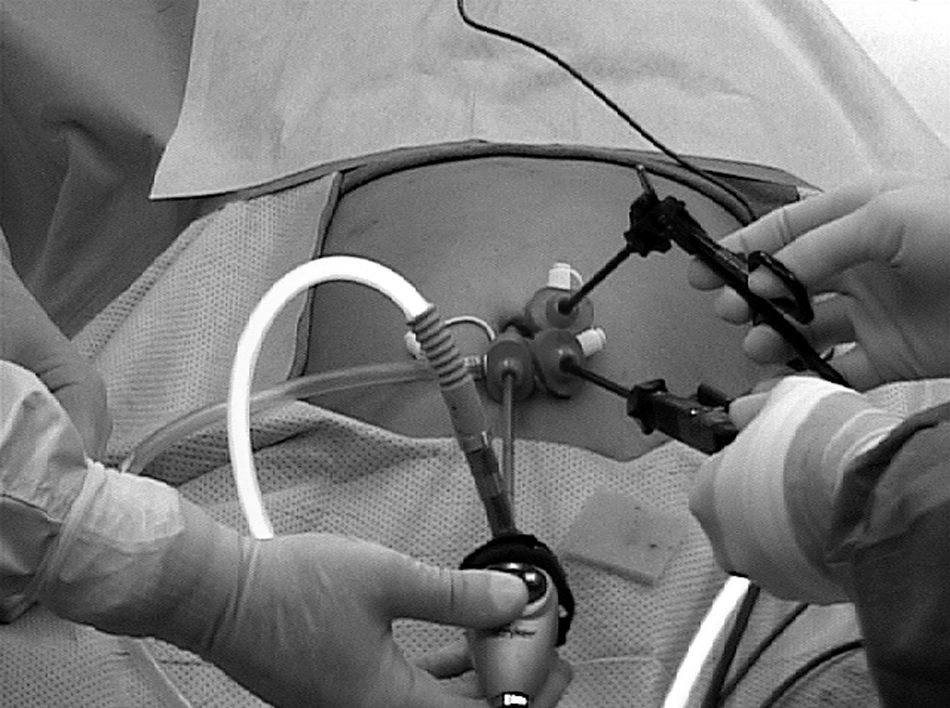
Instrument positioning as viewed in another patient with camera, straight grasper, and Maryland dissector.
The critical view of safety was confirmed after adequate exposure of both the anterior and posterior triangle of Calot was achieved, and observation of the cystic duct and cystic artery were verified to be entering the gallbladder in the presence of proper liver base exposure. The cystic duct was always clipped using a 5-mm laparoscopic clip applier and the cystic artery was either similarly clipped or divided with electrocautery. The gallbladder was dissected free of the liver bed using electrocautery and directly retrieved from the abdomen through the umbilicus without the use of an endobag. For the three trocar technique, the 5 mm abdominal fascial incisions were joined together into one incision to facilitate gallbladder removal and closed as a single incision in standard fashion. Outcomes measured for SILC included completion rate, operative time, length of hospital stay, estimated blood loss, and postoperative complications. These outcomes were compared with a concurrent set of 27 patients that underwent SLC. Data are reported as median and range. Continuous variables were analyzed by Mann-Whitney U test and categorical variables were analyzed by either a chi-square or Fisher exact test. A P value <.05 was considered statistically significant.
Results
We identified 54 consecutive patients who underwent cholecystectomy by a single surgeon during the study period from March 2009 to April 2010. SILC was attempted in 27 patients and SLC was performed in the remaining 27 patients. Twenty-four of 27 procedures (89%) in the SILC group were successfully completed. There were no differences in patient demographics (Table 1) or indications for surgery between patient groups (Table 2). The age ranged from 3 to 18 years in the SILC group (average 14 years) and 6 to 23 years in the SLC group (average 15 years). The 23-year-old patient had a corrected congenital heart defect and cholelithiasis.
Calculated as kg/m2.
BMI, body mass index; SILC, single-incision laparoscopic cholecystectomy; SLC, standard laparoscopic cholecystectomy.
For SILC cases, the patients were placed in stirrups with the surgeon standing between the legs. In the SILC group, there were 3 patients (11%) who required additional incisions for port placement for adequate exposure and/or safety concerns. One patient required an additional subxiphoid 5-mm port in addition to the three transumbilical ports to achieve adequate exposure. A second patient had significant cholecystitis, and thus two additional 5-mm ports were placed in the subxiphoid and right upper quadrant to complete the operation. The third patient with hereditary spherocytosis required a 12-mm port on the left side of the abdomen (in addition to the SILS port™) to safely perform division of the splenic hilum during planned splenectomy in addition to the cholecystectomy (Fig. 3). No additional ports were used in the remaining 24 patients in the SILC group, although in 3 patients a 2-mm Mini-Lap Alligator grasper was used through a right subcostal stab incision (2 patients), or through the umbilicus (1 patient) under direct laparoscopic observation for adequate exposure. As a replacement for transabdominal retraction sutures, the Mini-Lap grasper in these 3 cases was used as a safer alternative to adequately retract the gallbladder since the larger body habitus led to the increased difficulty of placing these sutures. The operation was safely completed in all 3 patients using this device, and at follow-up there was no visible scar in the 2 patients where the device was used through the right upper quadrant. All results are summarized in Table 3.
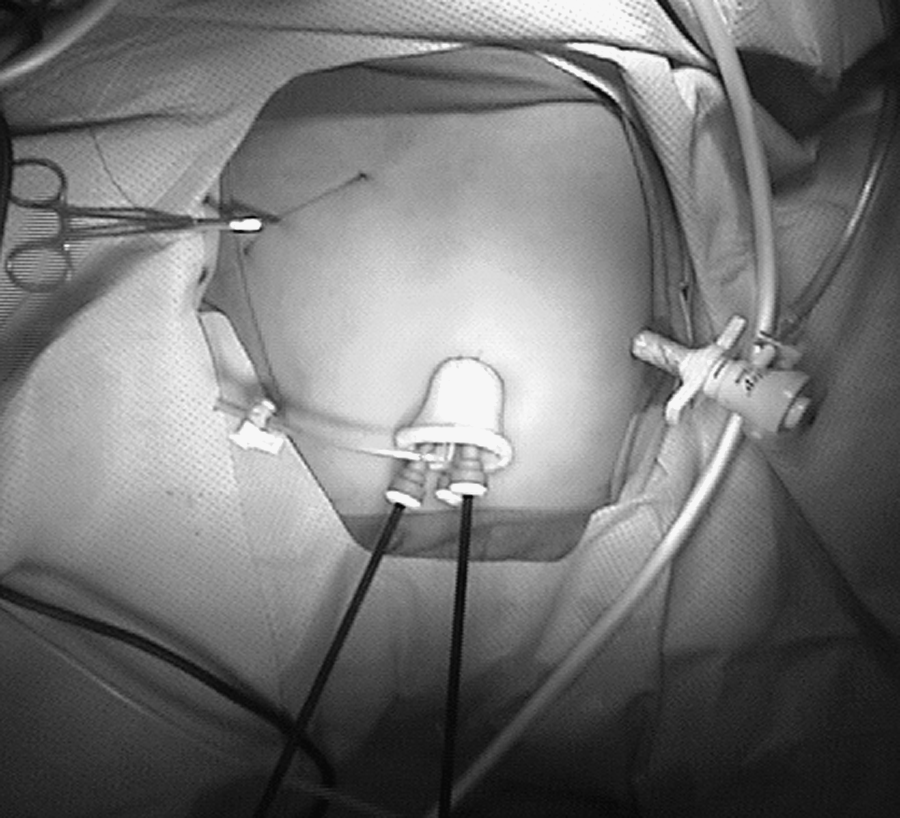
Trocar positioning for SILC with splenectomy. SILS™ port, retraction sutures for gall bladder, and 12 mm port in left abdomen in 8-year-old boy.
Operative time was significantly longer in the SILC group than in the SLC group (116 minutes versus 61 minutes; P value <.0001), but there was no correlation between operative times and patient BMI in either group. There were no intraoperative complications or conversions to an open procedure in either group. There were two postoperative complications in the SILC group and one postoperative complication in the SLC group. Two umbilical wound infections occurred in the SILC group and were treated with oral antibiotics. One of these patients had a prolonged operative time (193 minutes). In the SLC group, 1 patient was readmitted with scleral icterus and elevated liver function tests and was subsequently diagnosed with choledocholithiasis. This was managed by an endoscopic retrograde pancreaticography with sphincterotomy. Both groups had similar length of hospital stays with the majority of patients being discharged on the first postoperative day. Follow-up data from routine clinic visits 2–4 weeks after surgery were available for 25 patients (92.5%) in each group. The laparoscopic view of the critical view of safety during an SILC procedure is shown in Figure 4. All patients reported resolution of preoperative symptoms and returned to their normal activity levels.
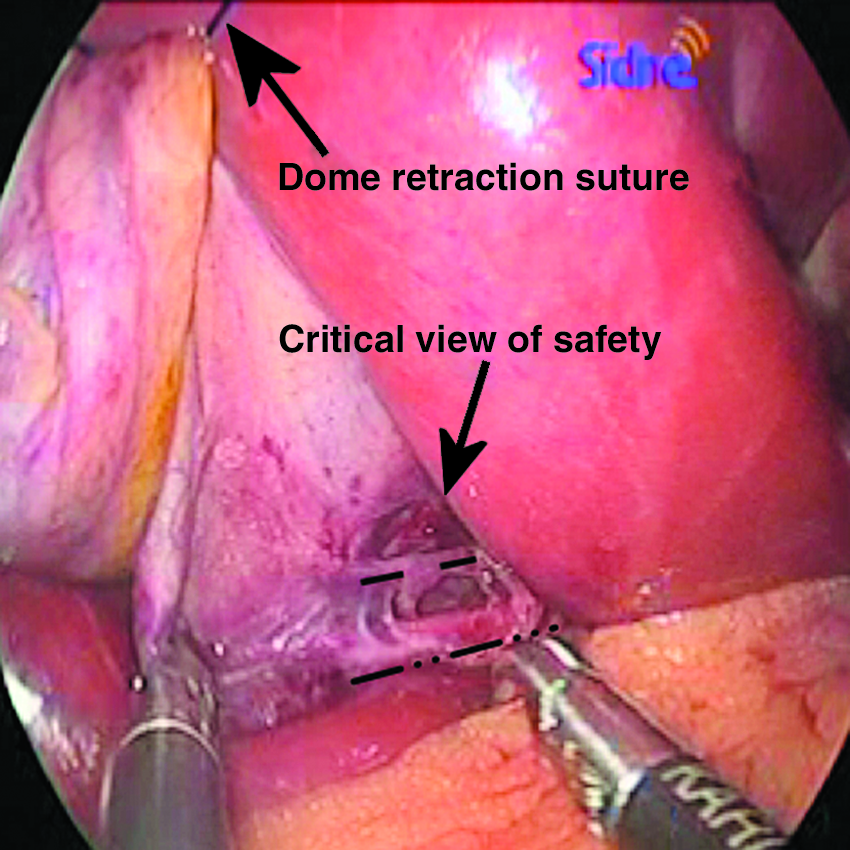
Operative view of the critical view of safety during an SILC procedure. The dashed line parallels the cystic artery and the dashed-dotted line parallels the cystic duct.
Discussion
An increasing number of surgeons are performing single-incision laparoscopic surgery for gall bladder disease in adults2–4 and a few reports in children.5–7 In this study, we were able to show that a laparoscopic cholecystectomy can be successfully completed using standard, straight laparoscopic instruments through a single umbilical incision in the pediatric population. Philipp et al. showed that for completion of SILC in the adult population, where they used straight instruments, this also took longer in their experience (85 versus 67 minutes). 8 They also employed frequent use of retraction sutures or one to three additional skin incisions in nearly 50% of patients to achieve success in completing SILC cases. Others have supported the use of reticulating instruments in children with success and OR times ranging from 68 to 99 minutes (studies with only 3 and 17 patients, respectively)5,6 compared with 54–199 minutes in our study. Whereas our approach may have been less costly in terms of instrumentation, we did not assess whether the increased operating room time for performing SILC would have negated any cost savings in instrumentation. In fact, it is likely that with the assistance of at least one articulating instrument, we would have had shorter operative times in the SILC group.
All attempted SILC cases as well as SLC cases were performed by pediatric surgery residents, second- or fourth-year general surgery residents with one attending surgeon (T.D.K.). There was a learning curve but no statistically significant decrease in operative time was observed for our SILC cases over the series. This is likely due to patient and resident variability along with the relatively low number of cases. In a similar-sized pediatric series of SILC, Nougues et al. demonstrated only a trend toward decreased operative time for these cases. 7 In spite of our success with the SILC technique, we do feel that it is the more challenging operation compared with standard laparoscopy. This study reveals that it takes longer and is subjectively more difficult to perform than standard laparoscopy as has been opined by others. 4 Using conventional straight instruments leads to in-line positioning of the laparoscope, proximity of the working instruments with limited triangulation, limited range of motion, and often a decreased number of ports, which contributes to increased difficulty.
The three individual port technique was our preferred approach with or without the use of transabdominal retraction sutures. Use of retraction sutures has been described in adult patients,9,10 but may be even more useful in pediatrics secondary to the decreased abdominal wall thickness in many patients. There are multiple devices and instruments developed to achieve this approach safely, but caution should be used when advocating this approach for the presumed improvement in cosmesis at the risk of compromising safety. 11 We did utilize the SILS port™ in some larger patients, but we do not believe that this system to be advantageous for use in smaller, thinner patients since the incision required to successfully place the port below the fascia is significantly larger (1.5–2 cm) and may be more difficult to conceal in these children. However, we feel that when used, the SILS port™ did allow for decreased back end instrument collisions with better separation of trocar heads within the platform.
We recognize the weakness of the retrospective nature of our study and our aim was to evaluate our results for the feasibility and safety of this approach in children in our initial experience. As suggested by Garey et al. there is a responsibility for all surgeons to identify methods to introduce “single-incision laparoscopic” surgery in an ethical and responsible manner based upon prospective collection of evidence. 12 There are concerns that if the SILC technology or approach is widely adopted without the evidence to support the safety and benefit; then, history may repeat itself whereby in the early 1990s there was an increase in common bile duct injuries after the introduction of laparoscopic cholecystectomy. 13 Accordingly, there is the need for further studies to determine the safety and benefit of this approach.
Chan et al. suggested in their pediatric hospital that the indications for cholecystectomy in children and thus the number of cases have been increasing in the “laparoscopic era.” 14 There has been an increasing number of cholecystectomies performed in our hospital within the last few years for uncertain reasons that cannot be explained by the “laparoscopic era” since the laparoscopic approach has been used almost exclusively for over 15 years. Safe performance of the procedure is of paramount importance and adherence to the principles of attaining the “critical view of safety’ must be achieved during every “single-incision cholecystectomy” as described by Rawlings and Strasberg.15,16 Rothenberg et al. reported an early series of a “modified single-port” laparoscopic procedure in children that included 10 cholecystectomies. 17 They advocated the liberal use of additional 3-mm instruments without additional ports, as a safe alternative to entirely single-incision access to achieve better observation and decreased operative time with no loss of cosmetic benefit. We would agree with this approach since operative time and observation can be significantly enhanced by use of these accessory instruments.
In conclusion, SILC in children can be performed safely and successfully with a variety of techniques using conventional straight laparoscopic instruments. Although operative times were significantly longer compared with SLC in a concurrent group of children, outcomes and results were otherwise equivalent. Liberal addition of additional trocars, retraction sutures, or instruments is recommended to enhance observation and safety as necessary. Additional studies should be performed to evaluate whether improved outcomes with respect to pain or cosmesis can be achieved compared with the standard laparoscopic approaches for cholecystectomy in children.
Disclosure Statement
No competing financial interests exist.