
Abstract
Abstract
Introduction:
Retroperitoneal fibrosis (RPF) is characterized by the presence of an inflammatory fibrotic process in the retroperitoneum causing compression of the retroperitoneal structures including the ureters. The ureterolysis is the liberation of the incarcerated portion of the ureter, from its proximal healthy portion to the distal portion, generally free of fibrosis, below the iliac vessels. We report the transmesocolic ureteral intraperitonealization as a new approach for laparoscopic treatment of RPF.
Patient and Methods:
A 52-year-old female patient diagnosed with idiopathic RPF was submitted to laparoscopic transmesocolic ureteral intraperitonealization after medical management failure. An open access using a Hasson trocar was placed through the umbilicus and two additional trocars were placed—10 mm in the midline at 6 cm below the umbilicus and a 5 mm in the midline at 6 cm above the umbilicus. The left mesocolon was incised 3 cm lateral to aortic pulsation and the left ureter was identified and dissected off the retroperitoneal mass. Lateral incised mesocolon was mobilized and wrapped posterior to the left ureter using a running suture.
Results:
Operative time was 2 hours. The mean blood loss was less than 100 mL. The patient was discharged painless on the second postoperative day. No complications were observed. Pathology showed fibrous tissue. An intravenous pyelography was performed at 6 months after the surgery and showed no ureteral obstruction. Serum creatinine level stabilized at 0.9 mg/dL.
Conclusion:
The transmesocolic ureteral intraperitonealization for laparoscopic treatment of RPF is feasible and can be considered a potential alternative for traditional laparoscopic intraperitonealization.
Introduction
Pain is the most common presenting symptom, but the clinical presentation can be secondary to obstructive uropathy and renal failure. 2 One of the treatment options for RPF with ureteral obstruction is ureterolysis. The ureterolysis is the liberation of all the incarcerated portion of the ureter, which is usually involved by a circular concentric fibrosis, from its proximal healthy portion to the distal portion, generally free of fibrosis, below the iliac vessels. In the majority of cases, the fibrotic retroperitoneal thickening is located between the last lumbar vertebrae and the first sacral vertebrae, in the region of the aortic bifurcation, sparing the posterior region of the great vessels. 4
The ureteral liberation, as an isolated procedure, can lead to relapse, hence the preference of the majority of surgeons for wrapping the ureters with retroperitoneal fat or greater omentum or, alternatively, intraperitonealization of them.2,5
Traditionally, this has been done as an open procedure with considerable morbidity and mortality.6,7 Laparoscopic ureterolysis (LU) was first reported by Kavoussi et al. in 1992. 8
Here, we report the transmesocolic ureteral intraperitonealization as a new approach for laparoscopic treatment of RPF.
Patient and Methods
A 52-year-old female patient was sent to our service with the diagnosis of idiopathic RPF. She presented with back pain and impaired renal function. She had no other comorbidity and had a 25 kg/m2 body mass index. Computed tomography showed an atrophic right kidney and severe left hydronephrosis due to a retroperitoneal fibrotic mass around the great vessels at the L4–L5 level (Fig. 1).

Computed tomography image showing a retroperitoneal mass anterior to the great vessels with entrapment of the left ureter (with stent).
Our initial attempt was bilateral ureteral stent and medical treatment using immunosuppression. The retroperitoneal mass had little regression after 1 year of treatment. An attempt was made to remove the ureteral stents, but the patient had a significant worsening of renal function. We opted for left surgical ureterolysis, using a laparoscopic transmesocolic approach. The patient signed the informed consent for the surgery.
Surgical technique
Under general anesthesia, after change of ureteral stents, the patient was placed in a 60° right lateral decubitus position. An open access using a Hasson trocar was placed through the umbilicus, allowing insufflation of the abdominal cavity with carbon dioxide. The pneumoperitoneum was maintained between 10 and 15 mmHg. Trocars were placed as follows: a 10 mm in the midline at 6 cm below the umbilicus and a 5 mm in the midline at 6 cm above the umbilicus. The laparoscope was introduced into the abdominal cavity through the umbilical port. The surgical steps were as follows:
Incision of the left mesocolon at 3 cm lateral to aortic pulsation with harmonic scalpel (Fig. 2) Identification of inferior mesenteric and left colic artery Identification of normal proximal ureter below ureteropelvic junction (UPJ) Access to the retroperitoneal fibrotic mass including ureter Mobilization of the ureter in an area above the level of the plaque Percutaneous stay suture (polypropylene 2) around the ureter to help the dissection Complete dissection of the ureter off the mass using a harmonic scalpel Biopsy of the fibrotic tissue showing no malignacy Lateral incised mesocolon was mobilized and wrapped posterior to the left ureter (Fig. 3) Running Vicryl 0 suture of medial and lateral incised mesocolon (Fig. 3) Closure of incisions
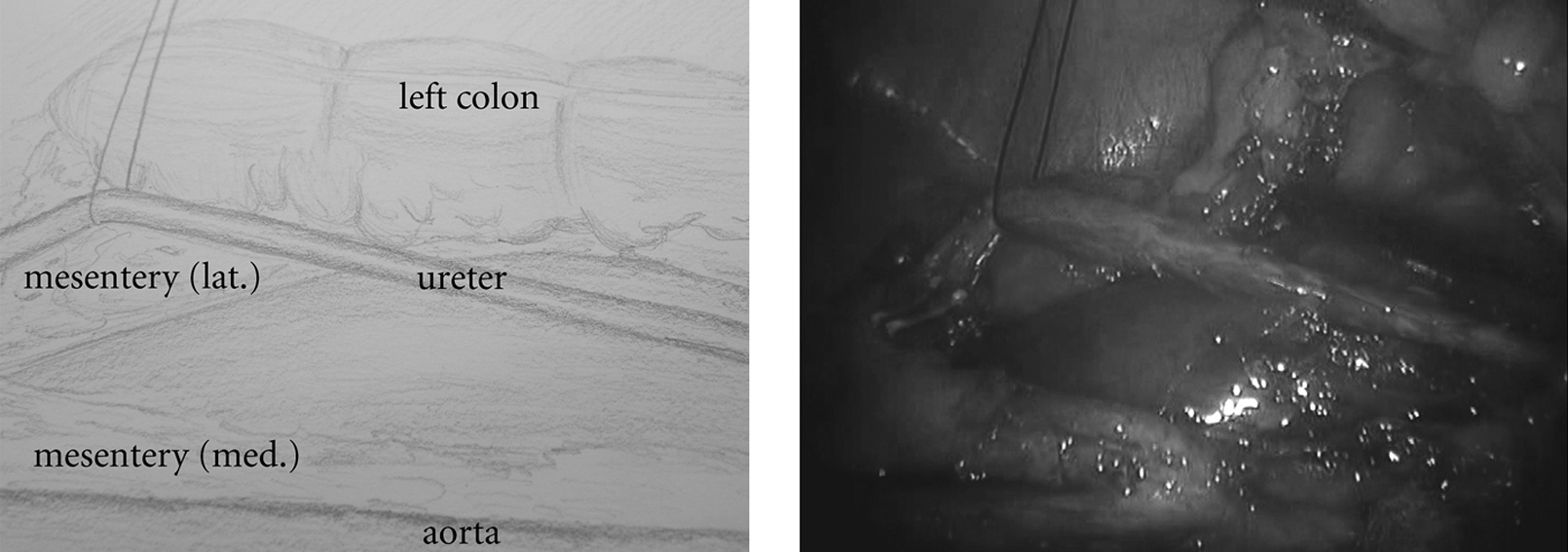
Complete ureteral dissection through the incision of left mesocolon.
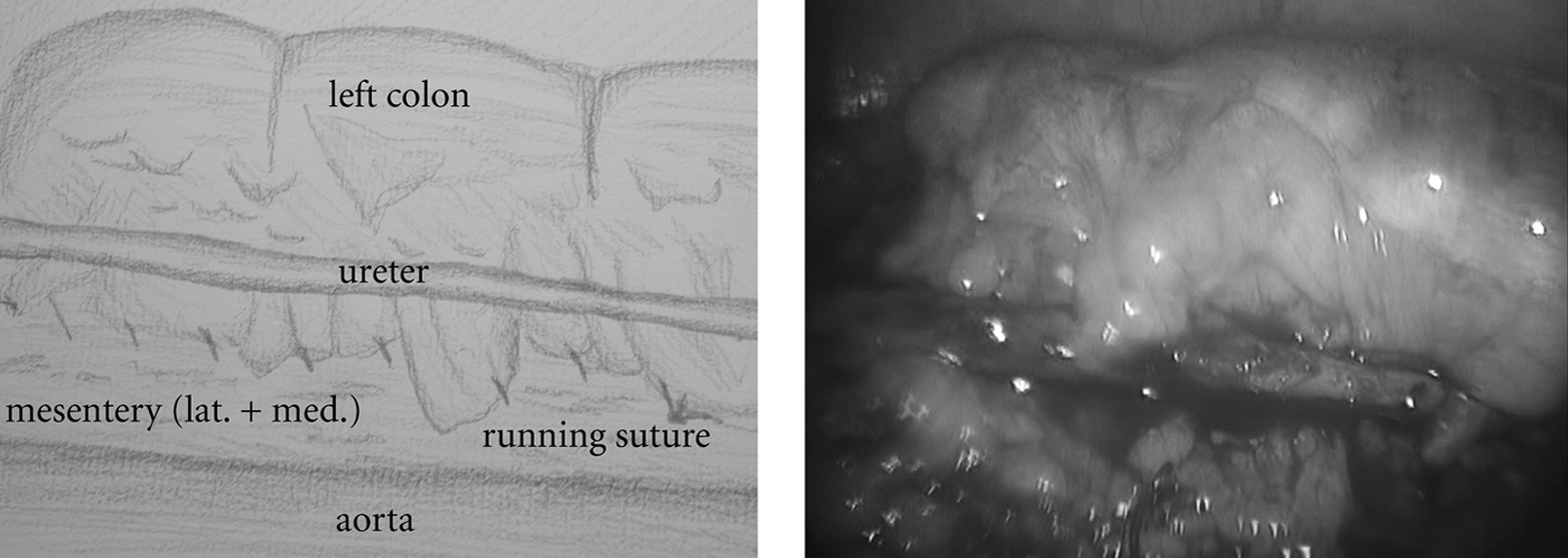
Final aspect after suture of medial and lateral mesocolon mobilized and wrapped posterior to the left ureter.
Results
Operative time was 2 hours. Blood loss was 100 mL (calculated and recorded by the attending anesthetist). Hospital stay was 2 days and the patient was pain free on discharge. No complications were observed. Pathology showed fibrous tissue with lymphocytes, plasma cells, macrophages, and fibroblast proliferation. The ureteral stent was removed at 1 month after the surgery.
One week after stent removal, the serum creatinine level was 1.2 mg/dL and an intravenous pyelography (IVP) showed no obstruction. Six months after surgery, the patient was asymptomatic and a new IVP and serum creatinine analysis were performed. The IVP showed good ureteral position and no signs of obstruction (Fig. 4). Serum creatinine level stabilized at 0.9 mg/dL.

Intravenous pyelography at 6 months after surgery shows no left ureteral obstruction. The atrophic right kidney was already nonfunctioning before the surgery.
Discussion
In 1948, Ormond described 2 patients with anemia, back pain, and a “chronic inflammatory retroperitoneal process.” 1 Since then, the RPF became established as a clinical entity.
RPF is typically characterized by the presence of an inflammatory, fibrotic process in the retroperitoneum causing compression of the retroperitoneal structures including the ureters. RPF most commonly affects patients who are 40–60 years of age. RPF cases have a male predominance, with a male-to-female ratio of 2 to 3:1. The true incidence is unknown but has been estimated to be 1:200,000 to 1:500,000 per year. 2
The retroperitoneal fibrotic mass generally centers around the distal aorta at L4–L5 and wraps around the ureters, leading to hydronephrosis via extrinsic compression on the ureters or interference with ureteral peristalsis. 9
In most cases of RPF, an initial attempt at medical treatment is pursued and is dependent on the suspected cause of fibrosis. For example, patients with primary idiopathic RPF are initially offered steroids or other forms of immunosuppression.10,11 Patients in whom treatment fails or those who experience recurrence after medical management or could not tolerate medical management are candidates for surgical ureterolysis.
A ureteral stent or a nephrostomy tube may provide temporary relief of the ureteral obstruction and preserve renal function; however, these devices are not curative. 7
Traditionally ureterolysis has been performed through a midline xyphopubic laparotomy, and various maneuvers such as intraperitonealization lateral to the colon and omental wraps passed through a mesocolon orifice have been described to decrease the chance of recurrence. 6
Tiptaft et al. 12 reported a 50% (4 renal units) rate of recurrence of RPF after open intraperitoneal placement of ureters and 6% (36 renal units) after omental wrapping. They also reported a 33% rate of complications in the omental wrap group and one death (5%).
The laparoscopic approach has gained acceptance since the first report of LU published by Kavoussi et al. in 1992. 8
Since then there have been several reports with small number of cases suggesting that patients who underwent this minimally invasive approach achieve lesser pain and better recovery compared with previous series of open procedure. Additionally, they showed that LU can be as effective and safe as the conventional surgery.5,13,14
Fugita et al. described a series of 13 patients with RPF who underwent LU. LU was successful in 11 patients (85%); two conversions to open surgery were needed (15%). 13
Srinivasan et al. 14 reported the largest series in the published literature, comparing open and laparoscopic techniques. Thirty-six (51.4%) patients underwent open ureterolysis and 34 (48.6%) underwent LU. Conversion to open surgery was required in 17.6% of the LU cohort. The etiology of obstruction was primary idiopathic RPF in 35 (50%) patients, whereas the remainder had secondary RPF, largely related to gynecological malignancy. There was no difference between the 2 groups when comparing operative time, estimated blood loss, length of hospital stay, complications, transfusion requirements, and postoperative resolution of ureteral obstruction. Of patients who underwent LU, 56% had intraperitonealization performed and 41% had omental wrap, demonstrating that these procedures can be safely performed laparoscopically if the surgeon deems it suitable.
Brown et al. 15 performed hand-assisted LU in 5 patients with less morbidity than open ureterolysis. It offers a shorter operative time and is less technically challenging than the conventional laparoscopy.
Miles et al. 6 reported two complications in 5 patients (40%) who underwent open ureterolysis: one pulmonary embolism and one phlebitis with sepsis. Kerr et al. 7 reported nine complications in a series of 16 patients (56%), including one death, two losses of a kidney, and two injuries to major arteries. Wagenknecht and Auvert 16 reported 26 patients treated by open ureterolysis with 1 postoperative death, 3 cases of ureteral leakage, and 1 case of aortic thrombosis (19%). Two complications, subcutaneous emphysema18 and pneumothorax,17 were described in previous case reports of LU. Fugita et al. reported four minor complications (30%) that were managed clinically and one major complication (8%), an iliac vein injury, which necessitated conversion to open surgery. 13
In all previous reports, colonic mobilization was the first maneuver to expose the retroperitoneum and to dissect ureter. On the basis of the safety and excellent exposition of ureter in previous reports concerning transmesocolic pyeloplasty for treatment of UPJ, we hypothesized that this approach could be applied to treat RPF.
Potential advantages of transmesocolic ureteral intraperitonealization include a direct access to middle third of ureter, faster operative time, less intestinal manipulation, less time to oral intake, and a physiologic position of mobilized ureter. It is also an alternative for patients who do not have retroperitoneal fat or an omental flap available to wrap the ureter.
Caution must be taken to preserve the major vasculature of colonic segment to prevent complications. In patients with very thin mesocolon, an omental flap can be mobilized to wrap the ureter.
Dissection of pelvic ureter distal to iliac vessels is a limitation of this approach. As the disease normally affects only the second portion of ureter above iliac vessels, our technique is feasible and safe. Other limitations can be observed in very fat patients, as the identification of ureter can be more difficult and challenging.
Conclusion
The transmesocolic ureteral intraperitonealization for laparoscopic treatment of RPF is feasible and can be considered a potential alternative for traditional laparoscopic intraperitonealization. Further evaluation of the technique in a larger patient cohort is indicated.
Footnotes
Disclosure Statement
No conflicts of interest exist.