
Abstract
Abstract
Purpose:
We describe a new minimally invasive percutaneous/laparoscopic-assisted technique based on the principles of the original open components separation described by Ramirez et al.
Methods:
The technique of minimally invasive components separation (MICS) is described in detail as a stepwise approach. The main advantages of MICS are compared with its traditional open counterpart and previously described endoscopic/laparoscopic modifications.
Results:
Open components separation is associated with increased wound problems due to extensive dissection. The MICS technique minimizes the need for large myocutaneous flap dissection, which in turn decreases postoperative wound complications. We have successfully corrected abdominal defects as large as 12 cm in diameter (113 cm2) with our MICS technique in a high-risk group of patients with minimal morbidity.
Conclusion:
The objectives of abdominal wall reconstruction, which includes restoring structural support, providing stable soft-tissue coverage, and optimizing aesthetic appearance, were all obtained with this newly described MICS technique. We believe that MICS is a safe, practical choice for repair of ventral hernia defects, because it minimizes postoperative morbidity and restores abdominal wall physiology.
Introduction
Operative Technique
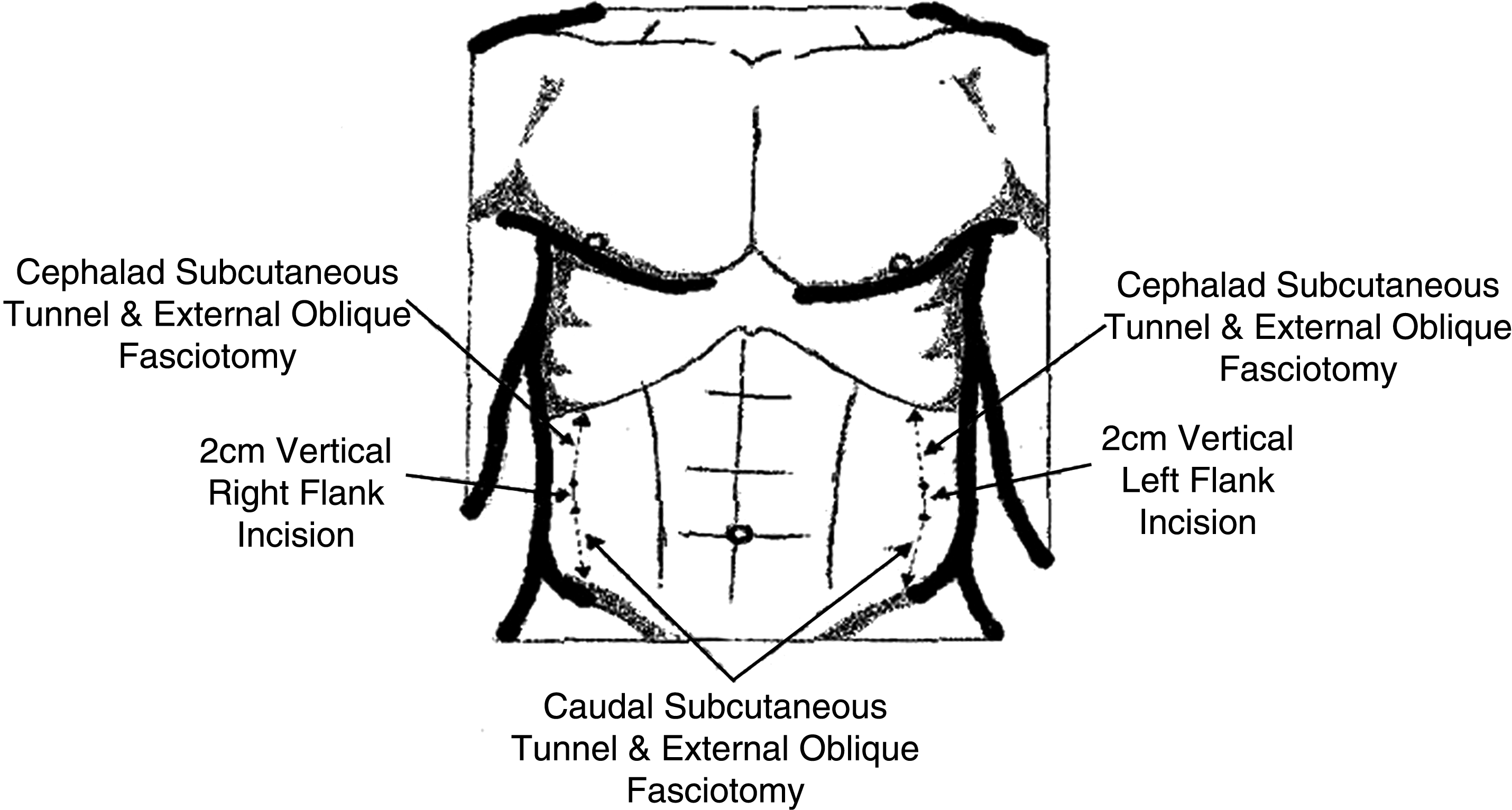
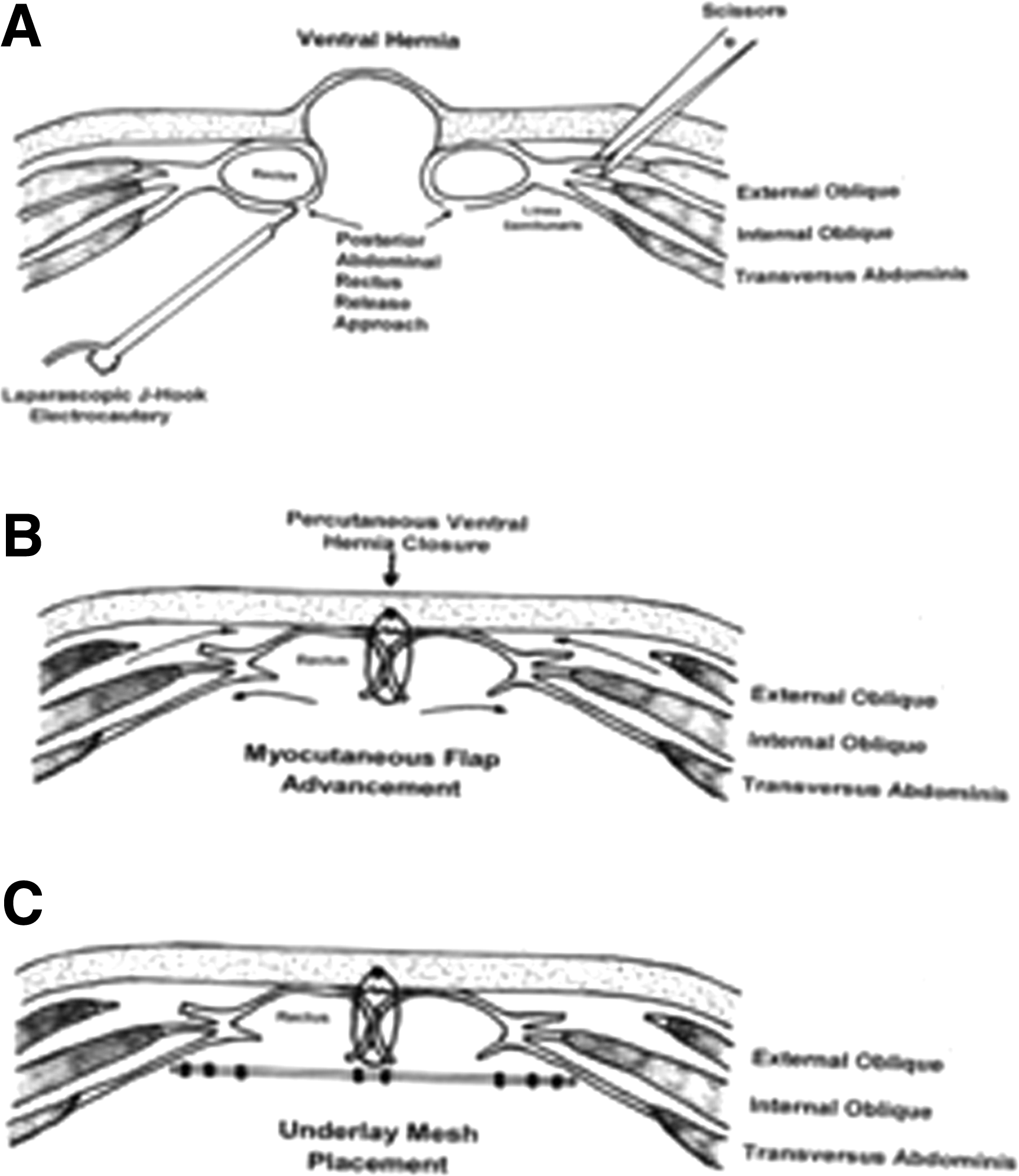
All patients receive preoperative prophylactic antibiotic therapy, deep venous thrombosis prophylaxis with sequential compression devices, foley catherization, and gastric tube placement. The patients are placed in the supine position with their arms out and a video monitor at each flank. The procedure begins with the placement of a 12-mm suprapubic midline trocar utilizing a Hasson technique for supraumbilical hernia defects or in the subxiphoid midline epigastrium for peri or infraumbilical defects. Carbon dioxide pnuemoperitoneum is insufflated up to 15 mm Hg pressure. Two vertical incisions, 2 cm each in length, are performed at the anterior axillary line on each flank midpoint between the costal margin and the iliac crest. The subcutaneous tissue is incised at each incision and a vertical subcutaneous tunnel is bluntly created with finger, with dissection up to the costal margin and downward to the iliac crest. Each subcutaneous tunnel is created lateral to the outer margin of the rectus abdominis muscle at ∼2 cm lateral to the semilunar line (Fig. 1). The external oblique fascia is identified via these flank incisions and a vertical fasciotomy is carried out with scissors under finger control following the previously created subcutaneous tunnels. The result is an external oblique fascial release 2 cm lateral to the linea semilunaris and extending as high as the level of the ninth rib down to the level of the iliac crest on each side (Fig. 1). Two 5-mm trocars are then transabdominally placed via each flank incision to aid in the posterior rectus sheath release (Fig. 2A).
Minimally invasive components separation.
Minimally invasive components separation.
We complete the components separation by performing a bilateral laparoscopic posterior rectus sheath release. A vertical incision is performed with a hook electrocautery instrument from the costal margin down to the level of the pubic symphysis and ∼2 cm from the medial edge of the posterior rectus sheath on either side (Fig. 2A). The peritoneal circular border of the ventral hernia defect is then cauterized to stimulate epithelization after primary closure. Primary closure of the ventral hernia defect is obtained via advancement of the rectus abdominis-transversus abdominis-internal oblique muscle flap complex by placing percutaneous perifascial ventral hernia figure of eight number 1 monofilament absorbable sutures (Fig. 2B). We recommend completion of the abdominal wall reconstruction with placement of an underlay synthetic mesh for clean cases or a biological mesh for potentially contaminated or contaminated cases. The mesh can be secured in place with a combination of stay sutures and absorbable tacks (Fig. 2C).
The pneumoperitoneum is deflated and the fascial defect of the 12-mm trocar site is closed with number 0 absorbable figure of eight interrupted sutures. All skin incisions are closed with number 4-0 absorbable sutures. There is no need for drains and diet is advanced as soon as bowel function resumes. Nasogastric tubes are used in cases in which extensive adhesiolysis is performed or signs of chronic incarceration are present.
Discussion
Ramirez and coworkers introduced the concept of “components separation” for closure of abdominal wall defects in 1990. This method produces immediate mobility of the ipsilateral rectus abdominis muscle-internal oblique-transversus abdominis muscle complex and allows significant freedom for medial transposition of this entire complex.4,5 This compound flap can be advanced ∼10 cm on each side around the waistline and it can achieve in most cases a dynamic closure of the abdominal wall.1,2 Despite its numerous advantages, the open components separation technique is still not without complications. 6 The original technique has the disadvantage that the skin and subcutaneous tissues must be mobilized over a wide area to reach and expose the aponeurosis of the external oblique muscle, which extends into the flank far laterally. This creates a very large wound, which predisposes to wound complications. Hematoma, seroma, and infection are reported in 11%–40% of patients, and skin necrosis was a frequent complication in the series of Lowe and colleagues.7,8 Also, recurrence rates of up to 30% have been reported with the use of this open technique alone. 9
These complications have led to the development of endoscopic and laparoscopic approaches for the separation of abdominal wall components, which allow myofascial advancement similar to the original open technique without the need for subcutaneous skin flaps. 9 Cadaver and animal studies have shown that endoscopic and/or laparoscopic components separation techniques provide from 86% to 100% of myofascial advancement obtained with the traditional open Ramirez technique.6,10 These newer methods of components separation have reduced the need for lengthy subcutaneous undermining, have decreased intraoperative blood loss, and have shortened the recovery time by nearly 50%. They have also reduced by 50% the rate of major wound complications (52% in the open group vs. 27% in the endoscopic group).11–13 Although a major wound complication rate of 27% represents a significant improvement, it remains unacceptably high.
The application of these newly developed techniques has certain drawbacks. One of these is the initial high cost of purchasing endoscopic equipment. Additionally, a learning curve is involved in becoming comfortable with the endoscopic approach, resulting in longer operative times. 8 Because of these drawbacks, we have developed a minimally invasive components separation (MICS) technique, which follows the original open description and resolves many of the previously described endoscopic/laparoscopic defaults. 6 With this new MICS technique, the use of a distention balloon and video endoscopy are avoided, minimizing cost and further abdominal wall tissue trauma by performing this portion of the procedure percutaneously. This also eliminates the need for drain placement. In our previously published case series, we have successfully corrected abdominal wall defects as large as 12 cm in diameter (113 cm2) with our MICS technique in a high-risk group of patients with minimal morbidity. Currently, we have expanded our capabilities with this technique and have successfully obtained primary fascial closures of abdominal wall defects that have extended up to 15 cm in diameter (177 cm2). There have been no technique-related complications or early recurrences during a short-term (1-year) follow-up. 14
The development of the lateral plane between the oblique muscles is considered critical by proponents of the endoscopic approach, because it enables greater release of the rectus muscle. 10 Our proposed MICS technique does not include such a dissection and reduces its possible advancement by an estimated 1–2 cm, but this deficiency is overcome by the addition of the posterior rectus sheath release on either side. Further, it is our early experience that the incidence of major wound complications is significantly less compared with the reported endoscopic counterpart as this virtual plane has not been extensively dissected where potential seromas and hematomas can form. 14
Conclusion
The objectives of abdominal wall reconstruction, which include restoring structural support, providing stable soft-tissue coverage, and optimizing aesthetic appearance, were all obtained with this newly described MICS technique. We believe that MICS is a safe, practical choice for repair of ventral hernia defects, because it minimizes postoperative morbidity and restores abdominal wall physiology.
Footnotes
Disclosure Statement
No competing financial interests exist.