
Abstract
Abstract
We report a case of a cystic adenomyoma in a 19-year-old nullipara who presented with severe dysmenorrhea and pelvic pain. Preoperative magnetic resonance imaging showed a 3-cm well-circumscribed mass with a 2.1-cm cystic cavity in the myometrium of the left fundus. The tumor, including the cyst, was excised via laparoscopy with a part of the normal myometrium using a modified myomectomy method. On histologic examination, the cystic cavity was lined by endometrial tissue composed of endometrial epithelium and stroma. After 12 months of postoperative follow-up, the patient had significant improvement of dysmenorrhea.
Introduction
In most cases, adenomyosis induces smooth muscle hypertrophy and hyperplasia and sometimes presents with the macroscopic appearance of a leiomyoma, so-called “adenomyomas” and “cystic adenomyomas” when cystic spaces are filled with blood.1,2
Diffuse adenomyosis is present in up to 20% of hysterectomy specimens from parous women >30 of age, but circumscribed forms, such as solid and cystic adenomyomas or cystic adenomyosis are rare conditions that occur even less frequently in juveniles.2,3
Based on the patient's age at the time of symptom onset, cystic adenomyomas can tentatively be classified into adult and juvenile forms, and each form may have different etiologies and clinical characteristics.2,3
Herein we report a case of a juvenile cystic adenoma with a review of the literature (Table 1).
SOAM, symptom onset after menarche; ICD/OCD, inner cystic diameter/outer cystic diameter; USG, ultrasonogram; CT, computed tomography; MRI, magnetic resonance image; HSG, hysterosalpingogram; NA, none available; LT, laparotomy; LPS, laparoscopy; RAL, robotic-assisted laparoscopy.
Case
A 19-year-old unmarried nulligravida presented with a 12-month history of pelvic pain and progressive dysmenorrhea that was not relieved by medications.
She underwent menarche at 12 years of age. After menarche, she repeatedly sought evaluation at other hospitals because of dysmenorrhea and pelvic cramping during menstruation and intermittently received treatment with nonsteroidal anti-inflammatory drugs or oral contraceptives. During the previous year, the pelvic pain and dysmenorrhea worsened. Thus, she was referred to our hospital for evaluation.
She declined a pelvic examination and transvaginal ultrasonography, because she was virginal, but consented to a magnetic resonance imaging (MRI) study.
The MRI demonstrated a thick-walled 3-cm round myometrial mass with a 2.1-cm cystic cavity in the left posterior uterine fundus, with no communication with the endometrial cavity (Fig. 1). No associated urogenital anomalies were noted on intravenous pyelography.
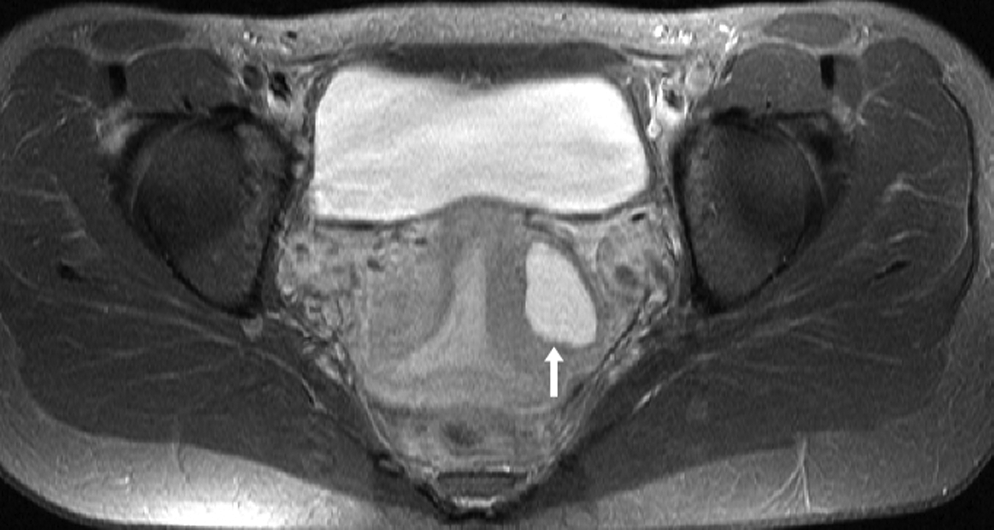
Transverse T2-weigted magnetic resonance image of cystic adenomyoma (white arrow) located on the left side of the uterine corpus.
A laparoscopy was performed on day 11 of her menstrual cycle under general anesthesia. A 10-mm triple-edge pyramidal trocar was used for the primary puncture after a skin incision was made along the lower margin of the umbilicus. Carbon dioxide was used for insufflation of the abdominal cavity. Both the second and third punctures were made in the lower quadrants with 5-mm trocars, and a fourth puncture was made in the left upper quadrant with an 11-mm trocar. The uterus was suspended by suturing both round ligaments to the abdominal wall.
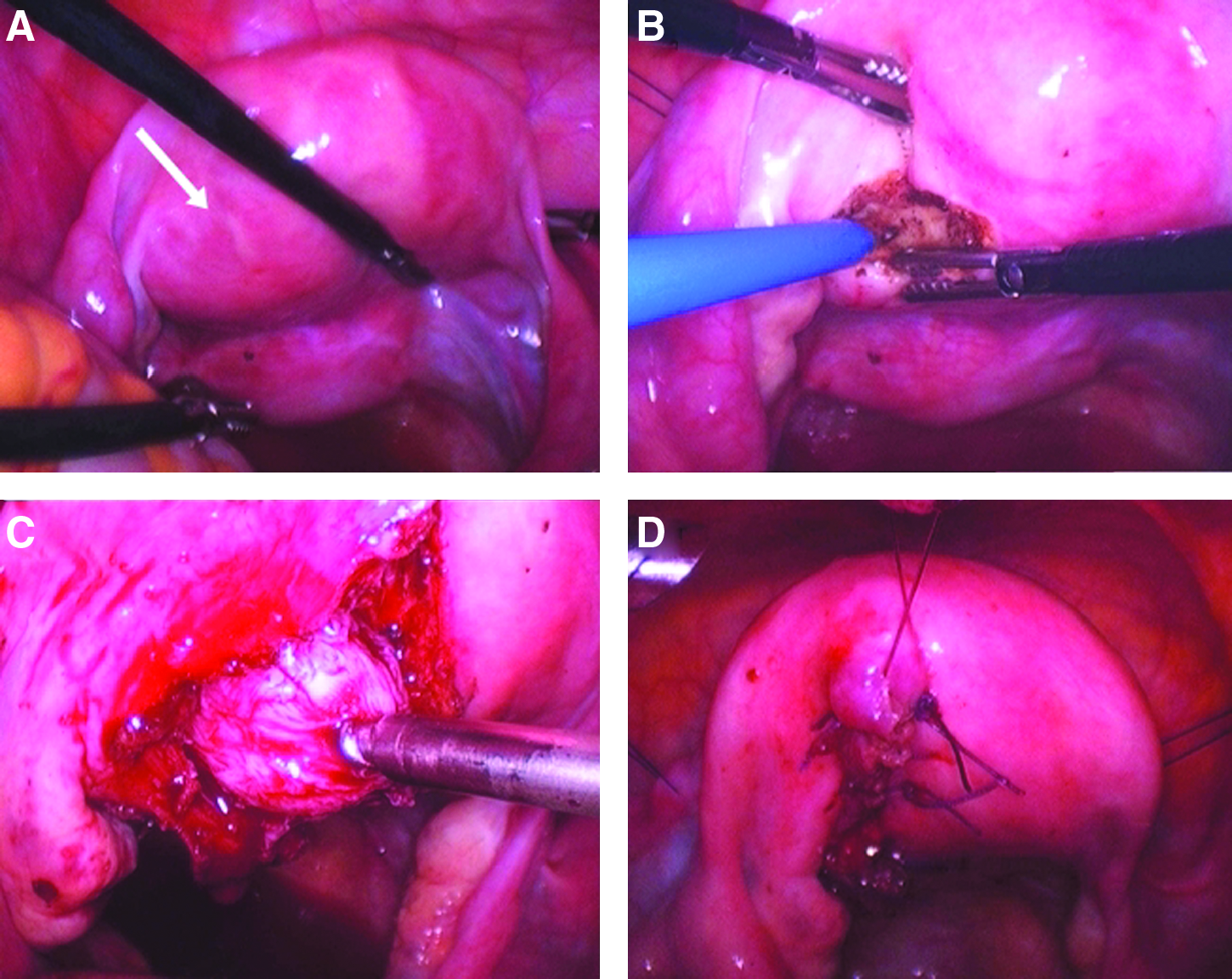
Under laparoscopic vision, the nodular lesion with an external appearance similar to that of leiomyoma was identified on the left posterior aspect of the uterus. Both ovaries and fallopian tubes were entirely normal in appearance.
After injection of vasopressin (10 units diluted in 100 mL of normal saline) into the surface of the lesion, monopolar cautery was used to vertically incise the serosa overlying the lesion.
During enucleation of the lesion, it was difficult to establish a clear plane and difficult to remove the lesion intact; thus, the tumor was divided and drained of thick chocolate-colored fluid reminiscent of an ovarian endometrioma. After drainage of the fluid, the tumor was removed from the uterus by careful excision with a Harmonic scapel and screw. There was no communication between the cystic cavity and the normal uterine cavity.
Serosal and myometrial defects were closed in an interrupted fashion with two layers of 1-0 monofilament sutures, then covered by an adhesion barrier (Fig. 2).
The excised tumor samples were removed through the 11-mm port using an endopouch. The patient was discharged 2 days postoperatively. After 12 months of follow-up, the patient has remained free of pain without any medications.
Macroscopically, the cystic cavity was lined by a cystic wall similar to endometrial tissue or the inner surface of an ovarian endometrioma. The outer surface appeared similar to normal myometrium; however, it was difficult to demonstrate clear margins between the inner cystic surface and the outer myometrial layer without magnification.
Microscopically, the inner layer was lined by endometrial glandular epithelial cells and stroma identical to the normal endometrial cavity. The outer layer appeared similar to normal myometrium without endometrial gland invasion, which was differentiated with diffuse adenomyosis (Fig. 3).
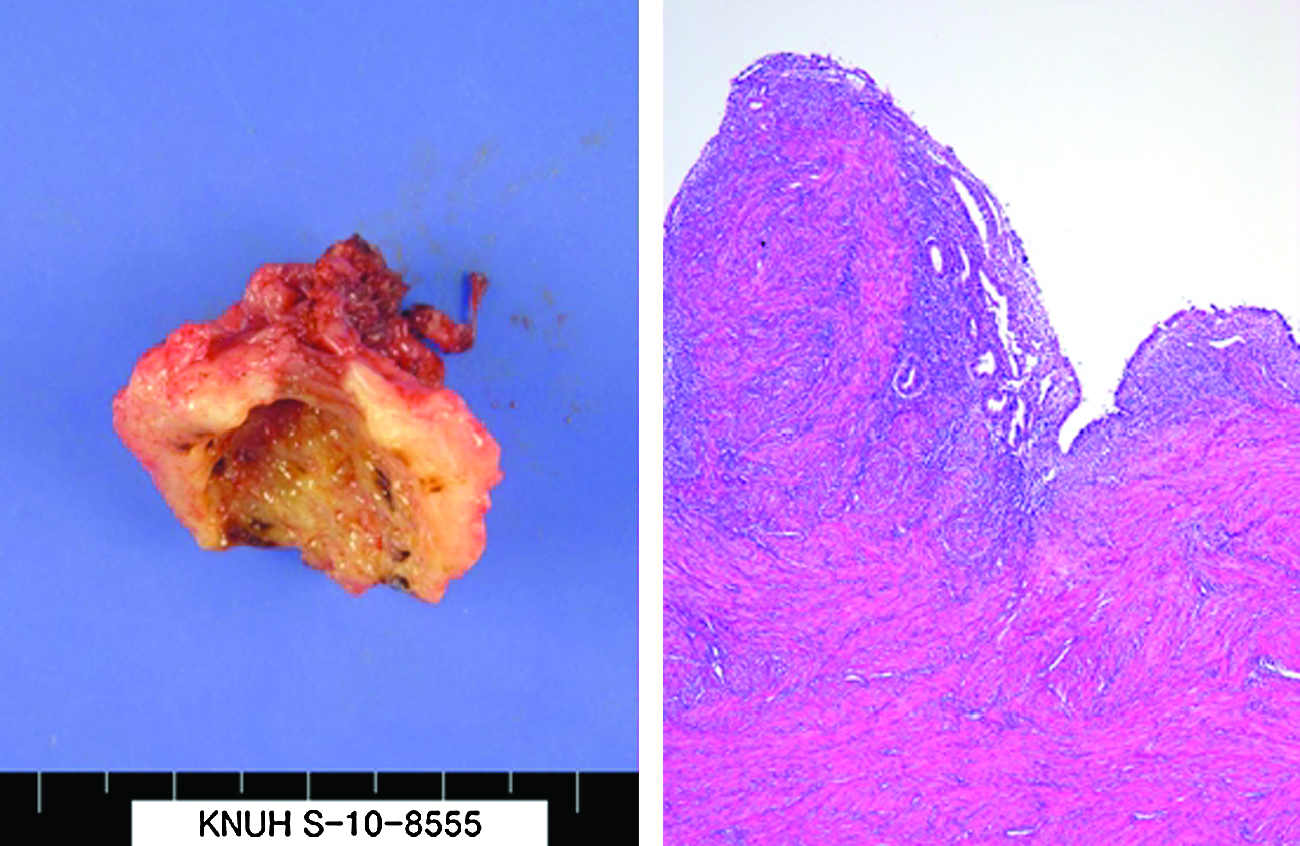
The inner layer was lined by endometrial glandular epithelial cells and stroma. The outer layer appeared similar to normal myometrium without endometrial gland invasion.
Discussion
The adult form of cystic adenomyomas is considered to represent small amounts of blood in the myometrium because of uterine adenomyosis. The lesions are usually <5 mm in diameter and occur in adult parous women >30 years of age and in association with surrounding diffuse adenomyosis. The adult form of cystic adenomyomas is considered to represent the hemorrhagic cysts resulting from menstrual bleeding in ectopic endometrial glands.2–6
The juvenile form of cystic adenomyomas is even more infrequent, and the inner cystic lesions are larger than the adult form, ranging between 1 and 3 cm in diameter. The lesions usually occur in young women with less of an association of surrounding adenomyosis. The juvenile form of cystic adenomyomas is considered to result from a congenital defect in the development of Müllerian ducts or a rare variant of cystic adenomyomas.2–6
Juvenile cystic adenomyosis and similar lesions have been reported under various diagnostic names, such as juvenile cystic adenomyosis,1,3,7 juvenile adenomyotic cysts, 6 an accessory uterine cavity, 8 and cystic myometrial lesions.2,9,10
Recently, Takeuchi et al. 10 suggested the diagnostic criteria for juvenile cystic adenomyoma and demonstrated successful laparoscopic excision in nine cases. They defined the diagnostic criteria as follows: (1) age ≤30 years; (2) cystic lesion ≥1 cm in diameter; and (3) associated with severe dysmenorrhea independent of the uterine lumen and covered by hypertrophic myometrium on diagnostic image.
These criteria have some limitations in differentiation of the adult and juvenile forms. First, the most striking clinical feature in the juvenile form is the early onset of severe dysmenorrhea that usually occurs soon after menarche. Takeuchi et al. 10 reported that the age of onset of dysmenorrhea had a mean of 6.6 years with a range of 1–13 years after menarche.
Second, there were 2 cases that delivered before surgery. Pregnancy and deliveries might give rise to endometrial injuries or lead to secondary adenomyosis.
Third, it has been reported that the inner cystic lesions are usually <5 mm in size in the adult form.
We suggest that more concrete or detailed criteria for juvenile cystic adenomyomas are needed, as follows: (1) the age of onset of severe dysmenorrhea within 5 years after menarche or ≤18 years of age; (2) no history of suspected endometrial or uterine injuries (delivery, myomectomy, and dilatation and curettage); and (3) cystic lesion ≥5 mm in imaging studies or after surgery.
We should not include the presence or absence of adenomyosis in the myometrium surrounding adenomyotic cysts. Until now, it is not clear whether or not juvenile cystic adenomyomas result from Müllerian duct anomalies or are a rare variant of adult cyst adenomyomas.
If the estrogenic stimulation of Müllerian rests (ectopic cells of paramesonephric origin) after long periods of quiescence lead to severe dysmenorrhea, the rate of adenomyosis in the surrounding myometrium would be lower. In contrast, if the lesion results from a rare variant of the adult form of cystic adenomyoma, the rate of adenomyosis in surrounding myometrium would be higher.
The etiologic causes or developmental defects in origin should be discussed, because the juvenile form of cystic adenomyoma could be diagnosed with clinical features based on the histologic findings, such as the presence of adenomyomas in the smooth muscle layer. Takeuchi et al. 10 considered the juvenile form as a cystic variant of adenomyosis rather than as a congenital abnormality. However, Tamura et al. 6 were unable to confirm the histologic evidence of adenomyosis in a specimen from a 16-year-old woman with the juvenile form of cystic adenomyosis. The authors suggested that the presence or absence of adenomyomas in the specimens might be related to the duration of symptoms after menarche or the age of the patient when undergoing surgery. 6
In contrast, Takeda et al. 2 suggested that juvenile cystic adenomyomas might be a congenital malformation caused by a developmental defect of the Müllerian duct, because of the symptoms presented soon after menarche and the histologic evidence of a well-developed, uterus-like organization.
Given the name of a noncommunicating accessory uterine cavity, Potter and Schenken 8 reported a case of juvenile cystic adenomyoma and suggested that the case would result from abnormal Müllerian duct development. In addition, Ball et al. 3 suggested a developmental etiology for juvenile cystic adenomyomas when a pre-existing developmental cyst within the myometrium became symptomatic after repetitive bleeding.
When diagnosing juvenile cystic adenomas, exclusion of Müllerian duct abnormalities, such as a noncommunicating rudimentary horn with a unicornuate uterus is important. Further differential diagnosis includes ovarian endometriomas and leiomyomas with fatty or hemorrhagic degeneration. 1 For this purpose, MRI is much more useful than ultrasonography or hysterosalpingography in establishing the diagnosis. Further, intravenous pyelography should be performed to exclude urinary tract anomalies that are frequently associated with uterine malformations.
The treatment of dysmenorrhea and abdominal cramps with nonsteroidal anti-inflammatory drugs, oral contraceptives, or gonadotropin-releasing hormone analogs in patients with juvenile cystic adenomyomas results in temporary relief of symptoms.
Therefore, surgical intervention, preferably laparoscopic resection, is the optimal treatment of juvenile cystic adenomyomas with severe dysmenorrhea.
At present, the etiology and actual incidence of juvenile cystic adenomyomas is unknown, but expected to be elucidated with advances in genomics and diagnostic procedures. However, the unified diagnostic name of these lesions should be based on pathologic evaluation.
Footnotes
Disclosure Statement
No competing financial interests exist.