
Abstract
Abstract
Laparoscopic management in a case of congenital urethroanal fistula with a normal anterior urethra in a 5-month-old male child is reported. A congenital H-type urethroanal fistula is a rare entity. Management of such fistula has always been surgical, ranging from perineal dissection, posterior saggital approach, to abdomino-perineal approach. We describe a minimally invasive laparoscopic method for approaching such fistula, which has not been described in the literature and is being reported for the first time.
Introduction
Case Report
A 5-month-old male child was referred with a history of repeated episodes of epididymo-orchitis and urinary tract infection requiring antibiotics treatment. The external genitalia appeared normal except for mild scrotal transposition and the anus was normally situated. On rectal examination, there was anal stenosis and no presacral mass was palpable. The boy was continent for urine and feces.
A micturating cysto-urethrogram showed a fistulous communication between the posterior urethra and the anorectum (Fig. 1). The anterior urethra was normal and grade II vesico-ureteric reflux was noted in the right ureter. Ultrasound examination of the abdomen revealed a horseshoe kidney with no evidence of a presacral mass and other investigations were normal.

Micturating cysto-urethrogram showing a fistulous communication (arrow) between the posterior urethra and anorectum.
At laparoscopy, an optical 5-mm port was introduced in the supraumbilical area and two 5-mm ports were introduced at the lateral border of rectus in the right and left flanks at the level of umbilicus.
The bladder was lifted up with a 2-0 vicryl stitch passed through the skin suprapubically, hitched with the bladder and brought out through the skin, and held with artery forceps. The peritoneum in the rectovesical pouch was opened up and rectum and anus were mobilized anteriorly and laterally all around. Below the seminal vesicles the rectum was found adherent to the urethra. Careful dissection around the urethra revealed a long, thick tortuous tract between the urethra and anorectum. Two silk ties were ligated on the rectal side and one on the urethral side (Fig. 2). Silk was used to prevent absorption and any recurrence, and also it would create a foreign body reaction so as to cause fibrosis of surrounding structures and further prevent recurrence. A portion of the fistulous tract in-between was divided and sent for histopathology, which was reported as a stratified columnar-lined fistulous tract. A tongue of omental tissue was dissected to interpose between the urethra and rectum but it did not reach; hence, no tissue interposition could be done.
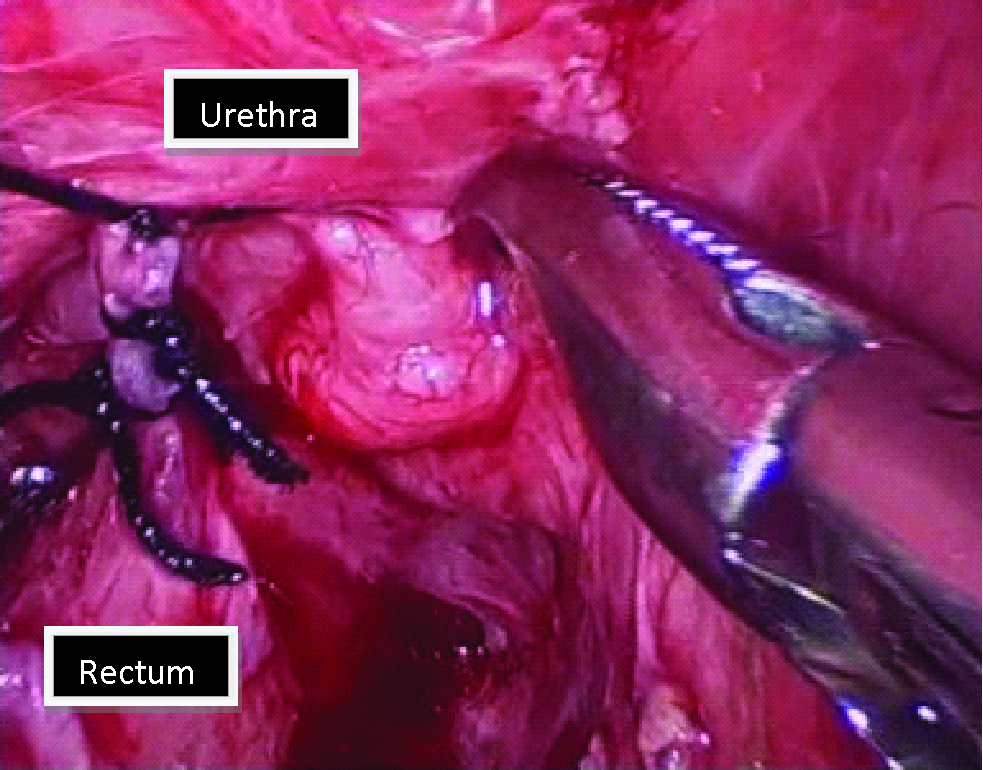
Laparoscopic dissection of the fistula between the anorectum and the posterior urethra with two ligatures on the rectal side and one ligature on the urethral side.
A peritoneal tube drain was introduced and urethral catheter was fixed. The baby was started on feeds after 24 hours and he passed normal stools on the second postoperative day. The baby was discharged on the third postoperative day with urethral catheter in situ, which was later removed after 7 days. Hegars dilatation was recommended for management of the anal stenosis. The baby made uneventful recovery and is doing well on a 6-month follow-up.
Discussion
H-type anourethral fistula is a congenital anomaly in which there is a fistulous communication between the anorectum and urethra without anal atresia. The fistula usually arises from the posterior urethra at the verumontanum. However, it can also arise from the distal posterior urethra or the bulbar urethra. The distal opening of the fistula may be seen in the rectum, pectinate line, or anorectal junction. In the present case, the fistula was seen arising from the posterior urethra; the distal opening was seen at the anorectal junction. 9
The embryologic basis for H-type anorectourethral fistulae remains unclear and controversial. Various theories have been forwarded by different authors.2,6,10 In the developing embryo, the urorectal septum divides the cloaca into a ventral component (urogenital sinus) and a dorsal component (rectum). Stephens and Donnellan 11 postulated that the fistula develops as a result of misalignment of these two components, which allows the cloacal duct to be preserved, communicating the urethra with the anal canal. In the present case, the fistula was seen arising from the posterior urethra and the distal opening was at the anorectal junction. The baby had right grade II vesico-ureteric reflux with horseshoe kidney and no presacral mass.
Surgical treatment includes anterior perineal approach with or without colostomy, 12 posterior saggital approach, or an abdomino-perineal approach if fistula is located high up.
The present case was managed with more innovative minimal access technique, thereby reducing multiple-staged procedure and avoiding major dissections around the sphincteric areas. Laparoscopic ligation and division of the fistula were facilitated by laparoscopy in terms of the excellent visualization of the anatomy and less damage to the surrounding structures such as sphincters, urethra, vas, and seminal vesicles. The recovery and discharge of this patient were earlier (3 days), compared with those operated by open technique (10 days). 8
If the fistula would not have been laparoscopically visualized, then a posterior saggital approach would have been tried as we are more conversant with the posterior saggital approach.
To the best of our knowledge and with respect to extensive literature search, laparoscopic approach to this rare anomaly has not been reported.
Footnotes
Disclosure Statement
No competing financial interests exist.