
Abstract
Abstract
Background:
This study was designed to analyze the outcomes of Nissen fundoplication (NF) versus Toupet fundoplication (TF) in patients undergoing laparoscopic antireflux surgery (LARS).
Methods:
All perioperative data, operative/postoperative complications, and follow-up data were prospectively recorded. All patients were seen on the 2nd month postoperatively and by yearly intervals thereafter. All patients have at least 12-month follow-up. Using SPSS software, groups were compared by t-test and chi-square tests as appropriate.
Results:
One thousand consecutive patients underwent primary LARS from May 2004 to August 2009. Six hundred eighty-four patients had NF and 316 had TF fundoplication. The mean follow-up of the NF (51.26 months) group was slightly longer than the TF group (43.53 months) (P=.018). There was no mortality and conversion. Esophageal perforation, jejunal perforation, and pulmonary emboli were the sole three major complications in separate patients. Dysphagia occurred in 15.4% and 9.9% in NF and TF, respectively (P=.001). Corresponding numbers for bloating were 19.6% and 10.8% in NF and TF, respectively (P=.001). Seventeen patients underwent reinterventions such as dilatation and re-do surgery and all 17 were in the NF group (P<.05). All other minor complications were similar except hiccups, which were seen in 30 patients and all were in the NF group (P<.05). Recurrence of reflux was observed in 1.8% and 2.2% of the NF and TF, respectively (P=.620).
Conclusion:
Both NF and TF are effective procedures in controlling the acid-reflux symptoms. The functional side effects appear more often in the NF group. These side effects can be minimized and reinterventions for severe/prolonged dysphagia can be avoided with TF.
Introduction
Since its introduction in 1991, LARS has become the gold standard for the surgical treatment of GERD. 2 The Nissen fundoplication (NF) entails a complete 360° wrap and is the most frequently used surgical procedure for the treatment of GERD. Although the efficacy of NF on acid reflux has been well documented,3,4 postoperative troublesome functional side effects of the procedure such as gas bloat and dysphagia have prompted the development of modifications and alternative techniques. Nevertheless, the Toupet fundoplication (TF) has become the most commonly used alternative procedure.
Over the past 10 years, a few number of randomized studies comparing these two procedures have been reported, with conflicting results.5–10 In this report, we analyzed and compared the outcome parameters in 1000 consecutive patients who underwent primary LARS with special reference to the type of the procedure. This report seems to be the largest series from a single center addressing this issue.
Materials and Methods
The study was conducted at our antireflux therapy center, which is a specialized tertiary referral center for the diagnosis and treatment of GERD. Gastroscopy (Olympus CV 260) at our center with biopsy is a routine procedure after a detailed history is obtained. All endoscopic procedures were carried out in the presence of an anesthesiologist. Before achievement of deep sedation during spontaneous breathing with propofol 1–2 mg/kg, the patients were premedicated with midazolam 0.05 mg/kg and fentanyl 1 μg/kg, while monitoring the vital signs. The Los Angeles classification was used for the endoscopic assessment of esophagitis. 11 Hiatus defects larger than 5 cm were defined as large hiatal hernia. pH meter was a routine diagnostic tool in patients without esophagitis. All patients were requested to stop any form of acid suppressive therapy for 5 days before pH testing. Orion II and Ohmega (MMS Enschede) devices were employed for a 24-hour pH meter test. A double-sensor, single-use catheter was used after calibration with pH 1.07 and 7.01 solutions. The results were analyzed and evaluated with a commercial software program.
A definite diagnosis is established according to the patient's history (typical symptoms responding to PPI) in addition to presence of esophagitis at gastroscopy. DeMeester score higher than 14.7 and/or symptom index >50% at pH meter analysis and biopsy-proven Barrett's disease were also conclusive evidence for GERD in symptomatic patients seeking surgical care. Indications for surgery were quite straightforward. Any patient having a definite diagnosis of GERD and who preferred surgical approach instead of daily lifelong PPI therapy and diet was a candidate for LARS. Before surgery, all patients routinely underwent a detailed interview regarding GERD symptoms, and extra esophageal symptoms were carefully recorded.
Manometric examination of the esophagus was also a routine procedure before the surgery. Drugs that might affect esophageal motility were discontinued 24 hours before the manometric study. The UPS 2020 stationary GI (MMS Enschede) device and four lumen water-perfused catheters with side holes positioned at 5 cm intervals and connected in series to a microcapillary infusion system were used to record esophageal motility and lower esophageal sphincter (LES) pressures. After nasal intubation with the catheter, the LES pressure, esophageal peristaltism, and the LES relaxation were measured using the “stationary pull-through technique.” The mean esophageal body contractile pressure (MECP) was measured using the mean values of 10 wet swallows of 5 mL of water at 30 seconds intervals.
Sonographic examination of the upper abdomen was also a preoperative routine as well as upper gastrointestinal series.
All operations were done by the senior author (M.A.Y.) and the series does not contain his learning curve. All patients were admitted on the day of surgery and underwent an antireflux procedure after an overnight fast. All patients with body mass indexes >30 received subcutaneous low-molecular-weight heparin during the induction of anesthesia. High-resolution video recordings of all operations were also collected for possible future analysis of technical details. The surgical procedure (NF or TF) was decided based on the preoperative manometric examination. Partial 270 degrees posterior fundoplication, namely Toupet's operation, was the procedure of choice in patients having mean esophageal contraction amplitudes <20 mmHg. In patients having mean esophageal contraction amplitudes between 20 and 30 mmHg, the choice between NF and TF procedures was tailored according to the severeness and erosive nature of the disease and compliance of the patient. Therefore, all patients in this category were specially informed about the probable increased risk for dysphagia that may alter their postoperative management if Nissen operation is to be preferred. In patients who are not willing to tolerate any swallowing problems, Toupet procedure was preferred. Partial fundoplication was also performed whenever there was a technical difficulty to secure a floppy wrap, that is, inability to cut short gastric vessels or difficulties in dissection. Patients who could not tolerate manometry also underwent the TF procedure. In patients with a symptomatic (causing dysphagia) Schatsky ring or benign lower esophageal stricture who had undergone preoperative pneumatic balloon dilatation, the TF was the procedure of choice regardless of manometric calculations, as further postoperative dilatations might be needed in the future and a Nissen's procedure may interfere with the success of dilatation.
Surgical technique
LARS was very standard for both procedures. All procedures were performed under general anesthesia with the patient in a modified lithotomy position. Six trocars were used. A careful dissection of the diaphragmatic cruras, the reduction of the hiatal hernia into the abdomen, and the crural repair with silk sutures were routine for both procedures. Usage of prosthetic grafts for the reinforcement of the hiatal repair also became a routine early in our experience and a V-shaped monofilament polypropylene graft (Prolene; Ethicon Ltd.) was used.
NF was performed by creating a 360° floppy wrap over a 60F esophageal bougie, with routine division of the short gastric vessels by using LigaSure™ (Valleylab). A 1–2-cm short floopy wrap was created and fixed around the esophagus with four/five stitches, two of them anchoring the anterior esophageal wall and two/three anchoring the right crura (Fig. 1a).
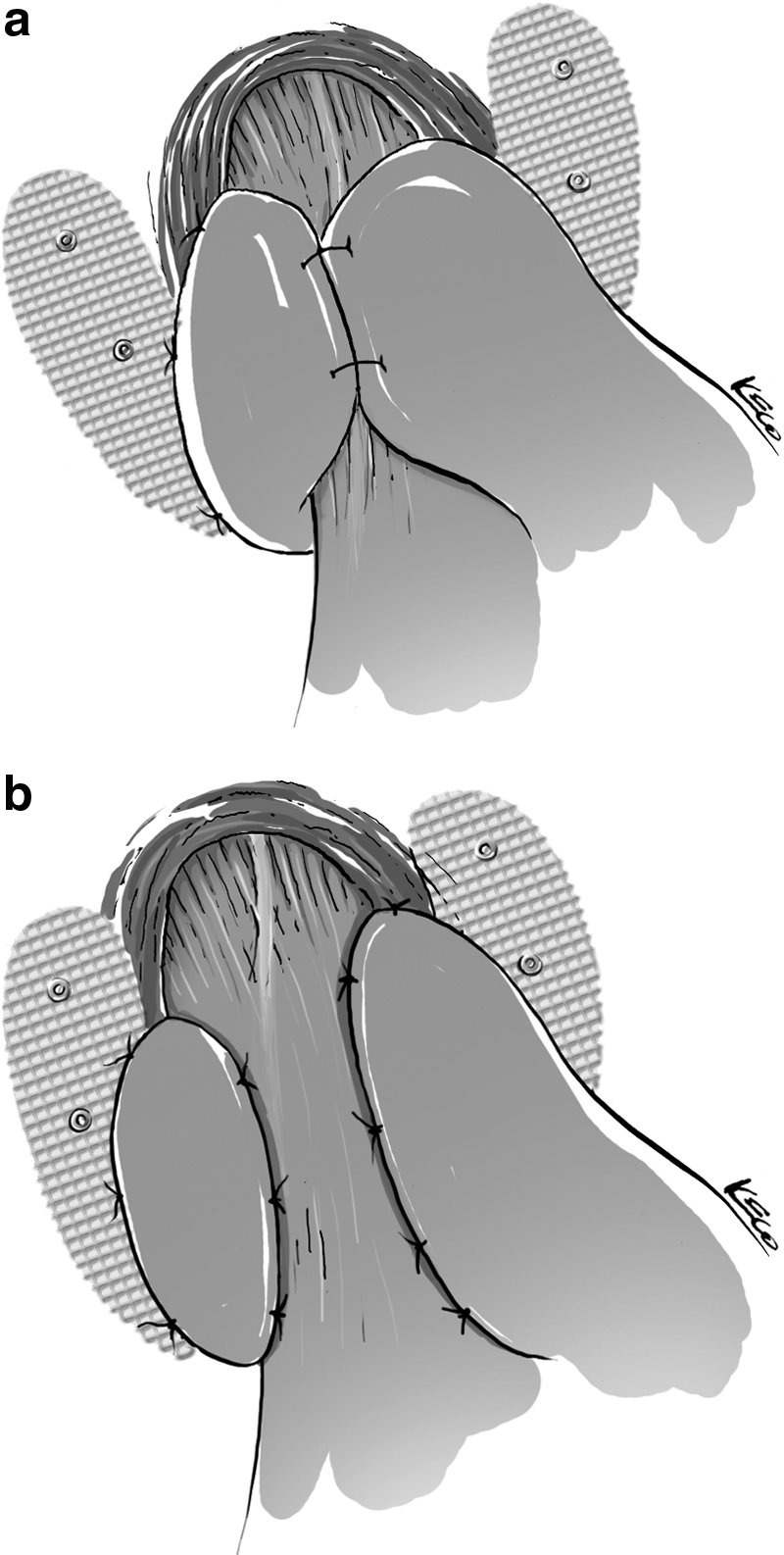
TF was performed by fashioning a posterior 270° wrap without bougie. The decision concerning division of short gastric vessels during Toupet procedure was taken based on the mobility of the stomach fundus and very rarely needed. The posterior (right) side of the wrap was first fixed to the right crura with two/three sutures. Then, the right side of the wrap was fixed to the esophagus using two/three silk sutures. The left part of the wrap was sutured to the anterior side of the esophagus by two or three sutures and a single suture was used to fix the upper side of the wrap to the upper edge of the left crura (Fig. 1b). Drains were rarely used at the surgeon's discretion.
Postoperative period
All patients were discharged at the first postoperative day unless specific problems occurred. Patients received liquids at the night of operation day, soup on day 1 and 2, soft diet on day 3, and a comparatively normal diet on day 4. All patients were seen at 1 week and 2 months after surgery and yearly thereafter. Patients who were not able to come for yearly visits were contacted by phone and asked their symptom status. No attempt was made to perform gastroscopy or pH meter testing during these controls unless the patient was symptomatic or had Barrett's disease.
Statistics
All data including demographics, perioperative details, operative/postoperative complications, and early/late outcome parameters were prospectively collected and stored in a computer database using SPSS software (SPSS for Windows 11.5; SPSS). The chi-square and t-tests were used for statistical analysis; P<.05 was recognized as statistically significant.
Results
Between May 2004 and August 2009, a total of 1000 patients underwent LARS. There was no mortality and none of the cases was converted to open procedure. NF was performed in 684 (68.4%) patients, and 316 (31.6%) patients underwent TF procedure. Demographic characteristics of the patients are outlined in Table 1. The mean age (40.95 versus 39) and the mean body mass index (26.49 versus 24.95) was slightly higher in the TF group.
Significantly different versus other group.
BMI, body mass index.
Apart from the MECP, preoperative findings of patients are similar in both groups as outlined in Table 2. As the choice of procedure was based on preoperative manometric findings, it is not surprising that MECP was significantly less in the TF group (31.87 versus 44.76 mmHg).
Mean±standard deviation.
Significantly different versus other group.
LES, lower esophageal sphincter.
Perioperative findings are shown in Table 3. Duration of surgery, discharge time, additional procedures, and drain usage were similar among the groups. Reinforced hiatoplasty with prosthetic grafts were more frequent in the TF group.
Additional procedures performed concomitantly.
Significantly different versus other group.
Perioperative complications are outlined in Table 4. Esophageal perforation, jejunal perforation, and pulmonary emboli were the only major complications. In one obese patient who underwent a TF procedure, pulmonary emboli developed the day after surgery. Prompt diagnosis with lower extremity duplex and pulmonary angiography, followed by immediate subcutaneous heparin for a week and oral anticoagulation for 1 year thereafter, was needed in this patient and she recovered without sequelae. Esophageal perforation was seen in the NF group and resulted from the bougie insertion. Perforation was immediately diagnosed and laparoscopically repaired with success, without any further sequelae. In 1 patient who also had an NF procedure, jejunal perforation, which resulted from the umblical trocar insertion, became evident 10 hours postoperatively. This patient was operated the day after LARS with laparotomy and recovered uneventfully. The distribution of these three major complications did not show a statistically significant difference between the groups. All the other minor complications were evenly distributed between the groups except hiccup. Hiccup was seen in 30 patients and all were in the NF group (P<.05).
Significantly different versus other group.
The mean follow-up of the NF (51.26 months) group was slightly but significantly longer than the TF group (43.53 months) (P<.05). Long-term follow-up and recurrence data are presented in Table 5. Dysphagia, resolving spontaneously within 6 months, was observed in 13.3% of all 1000 patients. This rate was 15.4% for NF and 8.9% for TF and there was a significant difference between the groups (P=.001). Prolonged dysphagia lasting >6 months was observed in 2% of the patients during the entire series. Prolonged dysphagia was also encountered significantly more in NF (2.8%) compared with TF (0.3%) (P=.001). Acute dysphagia, typically occurring during the immediate postoperative period, was easily diagnosed by no passage of opaque liquids in the upper gastrointestinal series and was observed in 9 patients. All of these 9 patients have had undergone a NF procedure and all were treated by early reoperation laparoscopically. All nine NF procedures were converted to TF within 1–7 days postoperatively, with enlargement of the hiatus in two. All early reoperated patients had an uneventful recovery without any dysphagia thereafter. Four patients required re-dos for prolonged dysphagia after failed dilatation attempts. All underwent laparoscopic conversion of their Nissen's procedure to Toupet with enlargement of the hiatal opening in 3. Dysphagia resolved completely in these 3 patients. In the other patient in whom the hiatal opening was not enlarged, a tolerable dysphagia still persists. Regarding bloating, there was also a significant difference between the groups and bloating occurred more frequently in the NF group (19.6% versus 10.8%).
Significantly different versus other group.
A total of 8 patients had esophageal dilatation postoperatively for prolonged dysphagia. Four patients responded to dilatation, whereas 4 required a re-do operation after several dilatations as aforementioned. Although not statistically significant, dilatations were all in the NF group.
Rehospitalizations for any reason excluding re-dos for dysphagia were evenly distributed between the groups (Table 5). The main reasons for these rehospitalizations were gas bloat, psychological problems, wound-related problems, and abdominal complaints, and all were conservatively treated without any sequela.
pH meter–proven reflux recurrence occurred in 19 patients (1.9%) during the entire series. A 1.8% recurrence rate observed in the NF group was not statistically different than the 2.2% rate observed in the TF group (Table 5).
Discussion
Patients diagnosed with GERD face a lifelong treatment requirement. As an alternative to lifelong treatment with PPIs, LARS can be offered to such patients. As LARS is not a lifesaving procedure and the main aim is to provide better life quality, the risk involved should be very low. Therefore, an ideal antireflux procedure should be safe, durable, and must result in minimal complications. In this study, we found no significant difference in reflux control up to 4 years after surgery between the treatment groups, although functional side effects were much more prevalent in the NF group.
The NF was first described by Rudolf Nissen in 1956 as an open abdominal approach, but over the past 15 years the procedure is being performed by using the laparoscopic technique. Since then, many studies demonstrated excellent results with laparoscopic NF, with an 86%–98% success rate on the control of acid reflux.12–14 Although its efficacy is well shown in these reports, the NF procedure has undergone many modifications because of troublesome side effects such as dysphagia and gas bloat.
Historically, a 3–5-cm tight wrap had been advocated as Rudolph Nissen first described the open procedure. This approach, although effectively controlling the reflux, has never gained wide acceptance because of its invasive nature and unacceptable high rate of dysphagia and gas bloat. Donahue et al. should be credited for their pioneering attempts to reduce such side effects by introducing the concept of “floppy” NF in the pre-LARS era. 15 On the other hand, as availability of laparoscopic technology considerably decreased the threshold for referring patients to LARS because of its minimally invasive nature, aforementioned side effects became a much greater concern. Generally, the investigators were focused on the tightness and length of the wrap, bougie usage, and division of short gastric vessels to reduce postoperative functional side effects. del Pino Porres and coworkers reported the results of 98 patients who were operated on by two different techniques of NF. 16 Group I underwent a short fundoplication that did not surpass 1.5 cm and group II underwent a 5 cm fundoplication. The postoperative manometric results demonstrated that there was a significant increase in tone and length of LES pressures after the fundoplication in both groups. DeMeester et al., besides emphasizing the importance of “floppy” NF, were able to decrease the rate of persistent dysphagia from 21% to 3% by shorting the fundoplication from 4 to 1 cm. 17 Recently, construction of a 1.5–2-cm-long floppy wrap is often preferred worldwide, as in our series.
Construction of the wrap around a bougie was another attempt to decrease postoperative complications. Patterson et al. reported the results of 171 patients who were randomized to bougie (56F) versus no-bougie group during fundoplication. 18 A significant decrease in mild to moderate dysphagia (13% versus 31%) and in severe dysphagia (5% versus 14%) was found in the bougie group after about 1-year follow-up. In the present series, we routinely used a bougie with a size of 60F during NF.
Division of the short gastric vessels during NF is another modification from the traditional procedure, which is still controversial. Previous reports demonstrated that fundoplication with division of the short gastric vessels is obviously associated with a better outcome. 19 However, more recent studies found no difference in postoperative dysphagia or overall satisfaction. Mardani and coworkers enrolled 99 (short gastric divided in 52 and left intact in 47) patients in a randomized trial to determine the efficacy of short gastric vessel division in reducing dysphagia. After a 10-year follow-up, they found no differences between the groups in symptoms reflecting postfundoplication complaints and quality-of-life outcomes. 20 Division of short gastric vessels during NF was also a routine in the present series.
To create a less obstructive form of wrap that would still prevent reflux appears to be a good option to reduce the mechanical side effects of NF. In this context, TF, which is described as a 270° posterior fundoplication, has become the most widely used alternative technique. Lindeboom et al. demonstrated that LES pressure is significantly increased after TF. 21 Some published studies from centers that are routinely performing TF reported that it achieves good control of acid reflux.22,23 However, Klapow et al. 24 reported a 20% reflux recurrence in a 3-year follow-up after TF. Further, Jobe et al. reported a minimum reflux recurrence rate of 21% after TF in a 2-year follow-up and condemned the procedure in patients with normal esophageal motility. 25 Therefore, only esophageal dismotility was thought as an indication to perform a TF instead of NF for many years. However, this hypothesis is still not clear and being tested by the investigators.
Thor et al. evaluated the results of open NF versus TF in a prospective, randomized fashion. Although the number of patients were small during this prelaparoscopic era, they showed unacceptable complication rates after NF without any recurrence advantage as well. 26
Over the past 10 years, a few randomized studies comparing the laparoscopic version of these two procedures have been reported, with conflicting results.5–10 None of these trials have shown any disadvantage of TF in the control of acid reflux. Among these studies, two reports failed to demonstrate any advantage for either procedure.6,10 Three studies demonstrated that TF has a better outcome in terms of dysphagia rates.7–9 One study favored the NF procedure according to immediate postoperative symptoms. 5
A recent meta-analysis that enrolled a total of 32 articles (9 randomized controlled trials, 8 prospective cohort trials, and 15 retrospective trials) was reported with 6236 patients, of whom 4252 (68.18%) underwent NF and 1984 (31.82%) underwent TF. 27 This study found no difference between NF and TF in terms of patients' satisfaction, perioperative complications, and reflux recurrence. However, the postoperative functional side effects after NF were more common than after TF as in our series.
Overall, dysphagia rates of the present series were 13.3% (15.4% for NF and 8.9% for TF) for early dysphagia and 2% (2.8% for NF and 0.3% for TF) for prolonged dysphagia. Severe esophageal dismotility diagnosed by routine preoperative manometry was an indication to perform TF in our series. Nevertheless, the TF group included all the severely dismotilitic patients, but yet dysphagia rates were still significantly lower than that in the NF group. These results were similar to the study by Strate et al. 8 Dysphagia rates in the trial by Booth et al. 7 were 27% and 9% for NF and TF, respectively, at a 1-year follow-up. Interestingly, Guerin et al. 5 found a significant difference between the two procedures regarding hyperflatulance (3.8% for NF and 16.5% for TF) and dysphagia to solids (11.6% for NF and 33.3% for TF), which were observed more often in the TF group. However, 1 month after the surgery, no significant difference in aforementioned symptoms remained.
Although postoperative dysphagia dramatically decreases within a few months after LARS, some patients will still undergo reinterventions such as balloon dilatation and re-do operations for severe/prolonged dysphagia as clearly shown in this series. Seventeen (1.7%) patients underwent reinterventions in the present series. Balloon dilatation was performed in 8 of 17. Four patients responded to dilatation, and the other 4 underwent a late re-do operation after several failed dilatation attempts. Acute dysphagia, which was easily diagnosed by no passage of opaque liquids in the upper gastrointestinal series, was another phenomenon and observed in 9 patients and all were reoperated. The most striking finding in the present series is the fact that all dysphagia-related reinterventions, namely dilatations and re-dos, were encountered in the NF group. In other words, dysphagia-related reinterventions were never needed with the TF procedure and the difference between the groups were highly significant (Table 5). It should also be noted that all reported precautions such as creating a short floppy wrap, using a 60F bougie, routine cutting of the short gastric, and good esophageal motility were secured during the entire NF operations. Nevertheless, against all precautions, dysphagia and dysphagia-related reinterventions could not be totally eradicated in the NF group.
In the present series, the prevalence of perioperative complications showed no significant difference between the groups except hiccup. Somehow, hiccup was seen only in the NF group.
One of the most important outcome parameter, namely the problem of recurrence, deserves special emphasis. The recurrence rate of LARS procedures considerably varies in the literature and have a wide interval between 2% and 21%.5,25 For achieving better recurrence rates, surgical expertise had been already credited enough, but reported recurrence rates of reflux after LARS show great discrepancy from one series to another, even in very experienced hands, depending on how the recurrences were sought. It is well known that aggressive follow-up protocols by routine postoperative pH meter and endoscopic control would result in much higher recurrence rates. Further, increased follow-up durations will also result in higher recurrence values. However, we do not think that invasive testing of an otherwise asymptomatic and satisfied patient is justifiable. We are aware that our approach might have missed some of the recurrences and our recurrence rates therefore could reflect a minimum, but 100% proven recurrences. As the definition of recurrence is very clear during the entire series (pH meter– and endoscopy–proven surgical failure in a patient whose symptoms are back), there were no comparison bias among our groups. In several studies, it has been shown that only 22%–29% of patients who have recurrent heartburn have evidence of anatomic failure or a pathological pH study.28,29 As suggested by Thompson et al., some patients with recurrent heartburn and a negative pH study have associated functional or psychiatric comorbidities such as depression. 30
The usage of prosthetic grafts for reinforced hiatoplasty is also a controversial issue. Although the use of a prosthetic mesh seems to reduce the risk for postoperative wrap herniation significantly thereby reducing the rate of mechanical failures, 31 deployment of a mesh is not free of complications. There are some anecdotal reports of mesh erosion 32 into adjacent organs but this has never been a problem in our series. As asymptomatic patients have not undergone routine endoscopical control, we might have underdiagnosed this theoretical problem.
We diagnosed GERD recurrence in 19 patients during a mean follow-up of 49.5 months and there was no statistical difference between the groups (1.8% in NF versus 2.2% in TF). All these 19 patients were back on daily PPI therapy instead of a reoperation. It is noteworthy that the mean follow-up of the NF group was significantly longer than that in the TF group.
We acknowledge that there are limitations of this trial. Nonrandomized nature of the study, lack of a scoring system for quality of life after the procedure, and the differences of the mean follow-up length between the groups are the weak points of this investigation. However, the large sample size, which seems to be the largest one addressing this issue, the prospectively collected data, regular follow-up of all patients, and the standardized nature of the operations owing to a single surgeon's experience seem to be the powerful points of this study.
The results of this study showed that NF and TF are both effective and durable procedures in terms of acid-reflux control. Functional complications are more often after NF, and although these side effects cannot be totally avoided, they can be minimized by choosing TF. It should be kept in mind that, despite all recommended preventions (bougie usage, division of short gastric vessels, and short fundoplication) to reduce postoperative dysphagia, 3% of patients who undergo NF may need a reintervention (dilatation and reoperation) even in skilled hands. These reinterventions can be totally avoided with TF. Patients suffering from GERD and who prefer a surgical therapy should be informed about the benefits and possible side effects of both procedures and should make their own choice.
Footnotes
Disclosure Statement
No competing financial interests exist.