
Abstract
Abstract
Background:
The laparoscopic Roux-en-Y gastric bypass (LRYGB) is generally considered the gold-standard bariatric procedure. It has a usual inpatient stay of 3 days. There have been few reports of gastric bypass patients being discharged within 23 hours of surgery, but its safety and feasibility has not been reviewed before. The aim of this study was to review the published literature on 23-hour stay post-LRYGB.
Methods:
Systematic search was performed in Medline, Embase, and Cochrane library using the medical subject heading terms “ambulatory surgical procedures” and “bariatric surgery” with further free text search and cross references. All articles on 23-hour LRYGB that described patient selection criteria, 23-hour discharge, complications, and readmissions were reviewed. Data were extracted by two independent reviewers.
Results:
There were no randomized controlled trials. Four cohort studies were included in this review. The patients age ranged from 14 to 70 years, mean body mass index ranged from 41.2 to 49.25, and the mean operative time ranged from 112.8 to 169 minutes. 1852/2201(84.14%) patients could be discharged within 23 hours. Forty-eight patients (2.18%) developed complications and 40 patients (1.82%) were readmitted. The commonest 30-day complications were anastomotic strictures (16), gastrointestinal bleeding (9), and internal hernias (9). Five patients developed anastomotic leak and 2 patients developed pulmonary embolism. Two patients died but neither was discharged after their bypass surgery.
Conclusion:
There is a paucity of data regarding 23-hour discharge after LRYGB. The evidence suggests that it is feasible in selected patients. However, further studies are necessary to assess its safety and acceptability.
Introduction
Materials and Methods
All articles published in English after 1990 on day-case bariatric procedures were considered. A systematic search in Medline, Embase, and Cochrane library was performed up to July 2010 using the medical subject heading (MeSH) terms “ambulatory surgical procedures,” “ambulatory surgery,” and “bariatric surgery” with equivalent free text searches and cross-references. Two independent assessors (H.T. and S.A.) evaluated the abstracts to select the studies for this review. Studies on 23-hour laparoscopic gastric bypass that described patient selection, 23-hour discharge, complications, and readmissions were included in this review. The two independent reviewers used specific data collection forms to extract data on patient selection, analgesic and antiemetic protocols, operative procedure, discharge criteria, discharge rate, causes of failed discharge, follow-up protocols, complications, and re-admission. The above data were analyzed and expressed as total, percentage, median (range), and in descriptive terms as applicable.
Results
Advanced PubMed search combining the MeSH terms “ambulatory surgical procedures” and “bariatric surgery” yielded 53 abstracts of which 7 were analyzed. MeSH term search in Embase and Cochrane provided 11 abstracts of which 1 new article on day-case bariatric surgery was obtained. Further cross references and free text searches using the key words “extended day case,” “ambulatory surgery,” “outpatient surgery,” “free-standing surgery,” “23-hour stay,” and “bariatric surgery” provided 369 abstracts from which 4 articles were obtained (Fig. 1). Of the above 12 articles, 410–13 were found to be suitable for this review (Table 1). The eight excluded articles were on day-case laparoscopic adjustable gastric banding (LAGB).
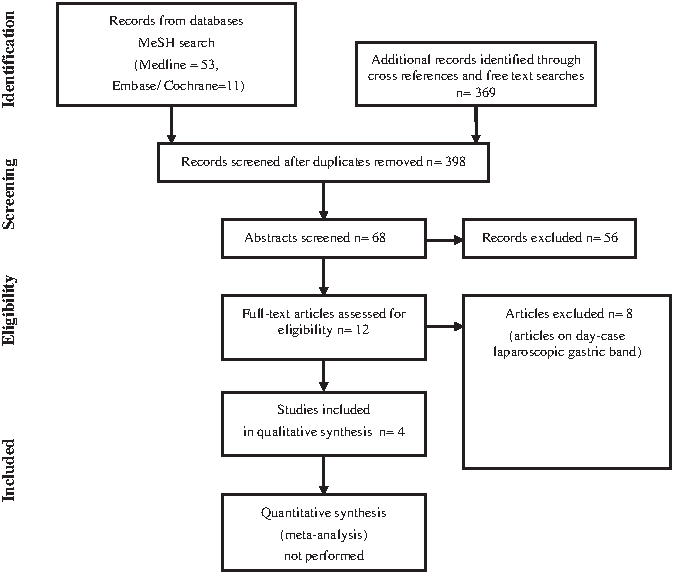
Flow chart of articles identified, included, and excluded.
ASA, American Society of Anesthesiologists; BMI, body mass index; N/M, not mentioned.
Participants
The patients age ranged from 14 to 70 years, mean body mass index (BMI) ranged from 41.2 to 49.25, and the mean operative time ranged from 112.8 to 169 minutes. 1852/2201(84.14%) patients could be discharged within 23 hours. Forty-eight patients (2.18%) developed complications and 40 patients (1.82%) were readmitted.
Patient selection
Patients included in the studies had a BMI >40 kg/m2 or BMI >35 kg/m2 combined with significant comorbidity.10,13 Exclusion criteria in the different studies included history of pulmonary hypertension, 12 revision procedures, 10 American Society of Anesthesiologists score more than 3, and uncontrolled obstructive sleep apnea. 12
Thorough history and physical examination and extensive anesthetic workup was performed to identify the most suitable patients for 23-hour discharge. 11 The preoperative workup included routine chemistry, chest X-ray, electrocardiogram, and either an upper gastrointestinal series or esophagogastroduodenoscopy. 10 An echocardiogram was obtained in patients with known cardiac disease. 10 Pulmonary function tests or sleep apnea tests were only selectively performed. Preoperative support group meetings were crucial to educate patients and motivate them for early discharge. 11
Analgesia and antiemetics
Intraoperative analgesia was by local infiltration of the wound with long-acting local anesthetic like ropivacaine hydrochloride and parenteral nonsteroidal anti-inflammatory drugs. 13 Postoperative analgesia was using intravenous morphine, 13 cyclo-oxygenase-2 inhibitor, 10 or patient-controlled analgesia, 10 which was converted to oral tramadol and diclofenac before discharge. 13 Intraoperative steroids along with other antiemetics were administered to reduce the postoperative nausea and vomiting.10,13
Operative details
Laparoscopic access was carried out through five to six ports. 13 A gastric pouch of 20 to 30 mL10,13 was created using staplers. The alimentary limb ranged from 100 cm13 to 150 cm10 and the biliopancreatic limb ranged from 60 and 80 cm. 13 Fares et al. 11 performed a dye test, upper gastrointestinal contrast study, and air leak test intraoperatively. McCarty et al. 10 included cohorts of patients with either 21- or 25-mm circular stapled gastrojejunostomy and either antecolic or retrocolic placement of the roux limb.
Discharge criteria
Moraes et al. 13 discharged patients if their pain was controlled with oral medications, had no complications, were able to cooperate, and had easy access to the surgical team. Sasse et al. 12 discharged patients who were ambulating and tolerating oral liquids. Fares et al. 11 discharged patients if their heart rate was less than 100/minute and did not have any unexpected symptoms. McCarty et al. 10 had a care path that allowed patients to tolerate liquids and initiate early ambulation. The key elements that were assessed on the morning after surgery were clinical evidence that the patient was tolerating liquids, the vital signs of pulse rate and respiratory rate, and the laboratory indicators of serial hematocrits. If any of these parameters were abnormal, an algorithm that includes a possible upper gastrointestinal series, a computed tomography scan, and additional observation was initiated. 10
Discharge rates
About 1852 out of 2201 (84.14%) patients could be discharged within 23 hours (Table 2). In the series by Moraes et al., 13 out of 13 patients who were admitted for more than 1 day, 11 remained for 2 days, 1 for 3 days, and 1 for 11 days. The reasons were gastrointestinal bleeding in 1 case, deep vein thrombosis in 1 case, vomiting and abdominal pain in 3 cases, and distance to home more than 100 miles in 8 patients. Fares et al. 11 reported that 5 out of 96 patients had unexplained tachycardia on the first postoperative day and underwent relaparoscopy, which delayed their discharge. McCarty et al. 10 had a 83.45% success at 23-hour discharge but has not specified the causes of prolonged stay.
Follow-up
Moraes et al. 13 reviewed patients on the 30th day after discharge, being seen by a surgeon, a clinician, a psychologist, and a nutritionist. Sasse et al. 12 followed them up long term but has not mentioned the specific protocol and Fares et al. 11 initially followed them up weekly.
Early complications
Forty-eight patients out of 2201 (2.18%) developed complications within 30 days of whom 17 required further surgical procedures and 31 were managed conservatively. The complications requiring further surgical procedures were internal hernia (9), 10 gastrojejunal leak (4), 10 jejunojejunostomy leak (1), 10 small bowel obstruction caused by adhesions (1), 12 small bowel perforation possibly caused by traction injury (1), 11 and revision of jejuno-jejunostomy for narrowed anastomosis (1). 11 The complications managed conservatively were gastrojejunal anastomotic strictures (16), 10 gastrointestinal bleeding (9),10,13 pulmonary embolism (2), 10 deep vein thrombosis (1), 13 anastomotic fistula (1), 13 urinary tract infection (1), 13 and pseudomembranous colitis (1). 13
There were 2 mortalities 10 among 2201 patients. One patient had a gastrojejunal anastomotic hemorrhage followed by cardiac failure and 1 patient developed unexplained postoperative multisystem organ failure. 10 Both patients were not discharged after their LRYGB.
Re-admissions within 30 days
Forty patients out of 2201 (1.82%) were readmitted within 30 days (Table 3). Moraes et al. 13 reported that 5 out of 67 patients were readmitted of which 2 were readmitted at 13th and 28th day because of gastric bleeding, 1 was readmitted on the 7th day with anastomotic fistula, 1 readmitted on the 17th day with urinary tract infection, and 1 patient readmitted on the 5th day with pseudomembranous colitis. In the series by Sasse et al. 12 1 patient out of 38 was readmitted because of small bowel obstruction. McCarty et al. 10 had a 1.7% rate of readmission but has not specified the causes of readmission.
Discussion
The LRYGB is generally considered the gold-standard bariatric procedure. It has been traditionally associated with prolonged in-patient stay and more early complication compared with LAGB. Improvements in surgical and anesthetic techniques have gradually reduced the duration of inpatient stay with some reports on 23-hour discharge after LRYGB. Early discharge after LRYGB reduces hospital costs and returns the patients to their familiar home environment. 11
Good patient selection and preoperative work-up is essential for early discharge after bariatric surgery. 14 The patient's overall physiological condition, ability to tolerate a general anesthetic, their BMI, and social aspects should be considered and optimized. Early identification and correction of comorbidities especially obstructive sleep apnoea is paramount. 14 Preoperative support group meetings are crucial to educate patients about the perioperative events and motivate them for early discharge. Sasse et al. 12 reported that the 38 patients discharged within 23 hours in their series represent only 3% of the total number of LRYGB performed, which demonstrates the extent of patient selection undertaken preoperatively.
A well-trained and experienced bariatric anesthetist is important for the success of early discharge after bariatric surgery. 10 Use of short-acting anesthetic agents, avoiding postoperative nausea and vomiting, and pain control techniques that minimize the use of narcotics can increase the chance of an early discharge. 14 Dexmedetomidine has shown a significant decrease in the use of narcotics and respiratory suppression. 15 The use of intraoperative steroids has long been used in the field of otolaryngology to decrease postoperative nausea. 16 Additional studies have shown that the steroids also decrease the excess inflammatory cytokine release that can accompany surgery. 17 Better postoperative pain relief was observed after intraperitoneal infiltration of local anesthetic agents after laparoscopic gastric procedures. 18 A positive nursing attitude before surgery to build confidence and expectation in the patients about early discharge is extremely important. 19
In this review, there was a 15.86% (349/2201) overall rate of failed 23-hour discharge after LRYGB. However, out of the 2201 patients included in the review 2000 were from a single series, 10 which did not specify the reasons for failed discharge. A protocol-driven pathway is essential for the success of early discharge after LRYGB. 10 The common causes for prolonged stay were due to suspicion of early complications and social reasons. This contrasts with studies on laparoscopic gastric band, where more than 99% of the patients could be discharged on the same day. 20 This reflects the more invasive nature and potential for complications after LRYGB compared with gastric banding. A cautious approach should be taken in selecting the discharge criteria at 23 hours. Any unexpected clinical features, especially pain and tachycardia, should delay discharge and prompt further investigations or re-laparoscopy. In their series of 2000 patients, McCarty et al. 10 demonstrated surgeon experience (>50 cases), age (<56 years), BMI <60 kg/m2, weight <400 lbs, comorbidities <4, and intraoperative steroid bolus as predictive of successful outpatient discharge.
In our review the 30-day complication rate was 2.18% (48/2201). The series by Moraes et al. 13 was a comparative study between next-day discharge after open and laparoscopic gastric bypass. The laparoscopic arm has been included in this review, which reported on their early laparoscopic cases that could explain the high complication and readmission rate. The commonest 30-day complications were anastomotic strictures (16), gastrointestinal bleeding (9), and internal hernias (9). This contrasts with a 0.91% rate of 30-day complication after gastric banding where most of the complications were caused by gastric pouch outlet obstruction or port and wound problems. 20 Many techniques have shown to reduce the incidence of complication after LRYGB. A decreased leakage rate was observed when staple line reinforcement strips were used. 21 An anticolic approach is associated with a significant decrease in internal hernias 22 and the incidence of gastrojejunal strictures was significantly lower with a 25-mm compared with a 21-mm anastomosis. 10 Surgeons should have completed their learning curve and demonstrate low complication rates before implementing early discharge after gastric bypass. 10
Robust follow-up plans are essential after early discharge post-LRYGB. This can be in the form of telephone contact in the first few days, clinic reviews, and availability of a 24-hour access telephone number for the patients in the early postoperative days. Patients need to be educated about the warning symptoms of complications and the need to seek urgent medical help if required.
In our review there was a readmission rate of 1.82% (40/2201). Most readmissions were for postoperative complications, but early discharge did not increase the rate of readmission. McCarty et al. 10 did not find a significant difference in the 30-day readmissions rates comparing those patients discharged within 24-hours and those discharged beyond 24-hours (1.7% versus 1.4%, P value not significant). Patient satisfaction was not assessed in any of the studies after LRYGB. Patient satisfaction showed conflicting reports after same-day discharge after laparoscopic gastric banding. Many patients felt that recovery is quicker in the familiar home atmosphere. 20 Others felt safer staying in hospital on the day of surgery because of the nursing care available and regular observations. 23
Limitations of this review are that only articles in English accessible from the main databases have been included. Further data may be available in the gray literature or published in other languages.
This review suggests that there is a paucity of data regarding 23-hour discharge after LRYGB. Evidence from limited studies available suggests that LRYGB is feasible as a 23-hour procedure in selected patients. However, its safety and acceptability needs to be evaluated further. Standardized approach to patient selection, good education and preparation, meticulous operative technique, robust postoperative care, and follow-up are essential for early discharge after LRYGB.
Footnotes
Disclosure Statement
No competing financial interests exist.