
Abstract
Abstract
Pediatric minimally invasive surgery is a rapidly developing field with a steep learning curve for each new procedure that is developed and integrated into practice. The European consensus is that the training across the learning curve should not be on the patients. Simulation is a widely accepted methodology to shorten the learning curve. Training on animal models is an advanced form of simulation. This helps to reduce morbidity and the costs of patient care. This article describes our 3 years of experience in the development of animal models for training in pediatric minimally invasive surgery.
Introduction
We present 3 years of our experience from January 2008 to December 2010 in the development of animal models, which offer a high level of simulation for training of pediatric surgeons in advanced MIS.
The detailed descriptions in this report will obviate the need for repeating the development phase in other centers and will provide a useful foundation for development of models for other more complicated procedures.
Protocol
The study was approved by the Scientific Advisory Committee and Animal Ethics Committee of Children's Hospital at Westmead, Westmead, NSW, Australia. Measures were taken to fully comply with the Australian Code of Practice for the care and use of animals for scientific purpose.
Twenty-three Landrace cross-bred pigs (weighing 19–21 kg) and eight piglets (weighing 6 kg) were sanctioned for the purpose. Various MIS procedures were performed over a period of 3 years between April 2007 and March 2010 by a team of pediatric surgeons, which included three Research Fellows and three Consultants. The Research Fellows had at least 5 years of pediatric surgical experience, and either a Fellow or a Consultant was scrubbed during any given procedure. They were supported by a research nurse and the veterinary personnel of the animal facility. Special attention was paid to the selection of the size of the animal to best simulate the common age group of children in whom the procedure is commonly performed. Innovations that were necessary in order to simulate the pathological features of the disease or the anatomy of the operative field were carefully documented. The level of experience required to successfully complete the procedure on the animal model and the level of simulation achieved were noted and are presented in Tables 1–3.
VUR, vesicoureteral reflux.
Initially in 2007 we tried using a rabbit model and pigs of various sizes and then concluded that a 20-kg female pig and 6-kg piglet were ideal models for training in pediatric MIS.4,5
Procedures
Anesthesia
The animals were anesthetized by a veterinary surgeon with zolazapam/tiletimine (Virbac) (4.4 mg/kg), xylazine hydrochloride (Tray Laboratories) (2.2 mg/kg), and atropine sulfate injected intramuscularly. Intubation was then performed using an endotracheal tube: 7.5 mm for pigs and 4–5.5 mm for piglets. Anesthesia was maintained on isoflurane (2%).
At the end of the procedure, while the animal was under anesthetic, euthanasia was administered with pentobarbitone sodium (Virbac) (160 mg/kg) injected intravenously. 5
Thoracoscopy (neonatal)
A 6-kg piglet was positioned mid-prone with its right side elevated. This allowed the lung to fall away for ideal exposure. An orogastric tube was placed prior to the procedure. The ports were inserted as shown in Figures 1 and 2. Pneumothorax was created and maintained at 3 mm Hg. In total, 8 piglets were used to develop the following thoracoscopic models.
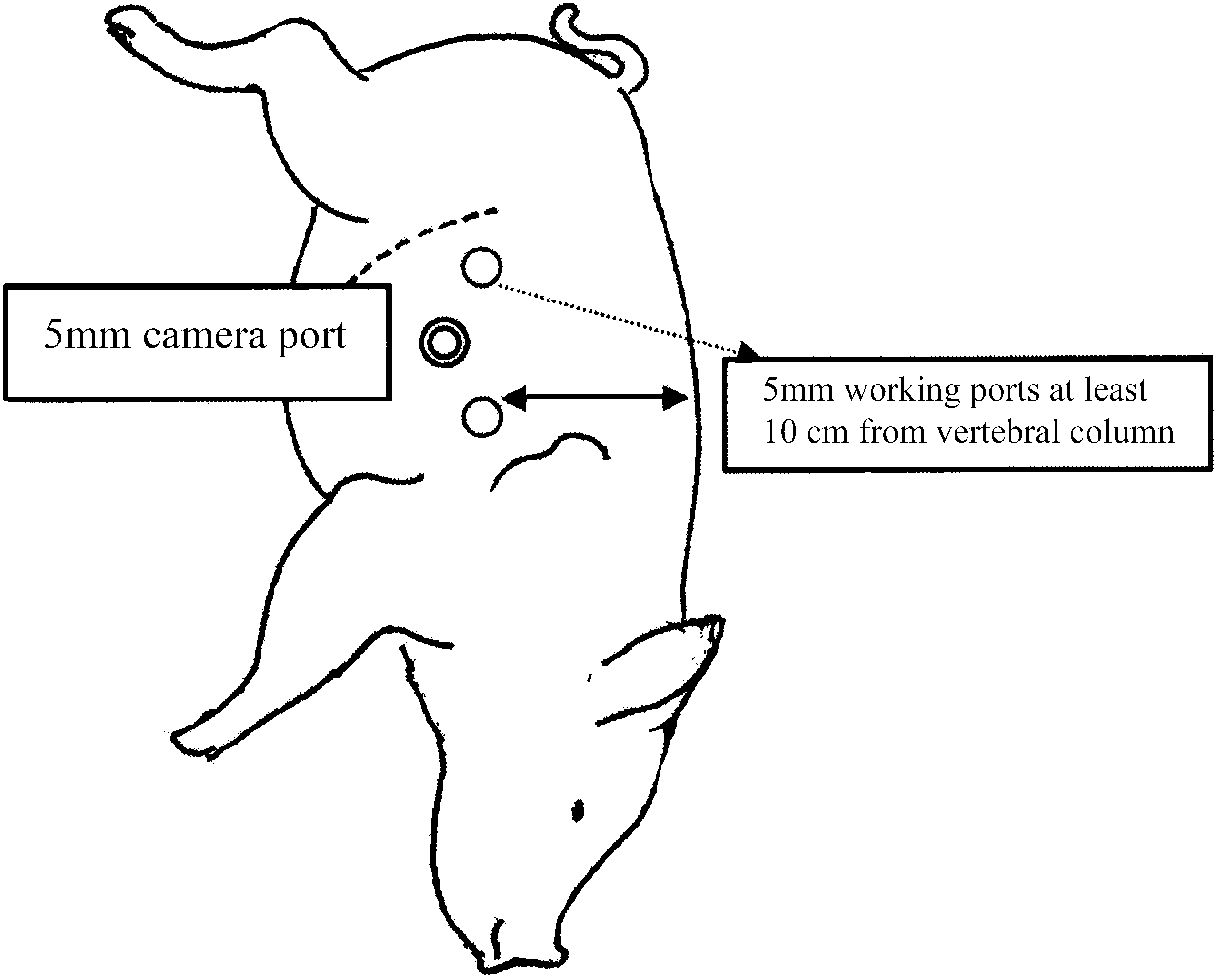
Recommended port placement for esophageal anastomosis.
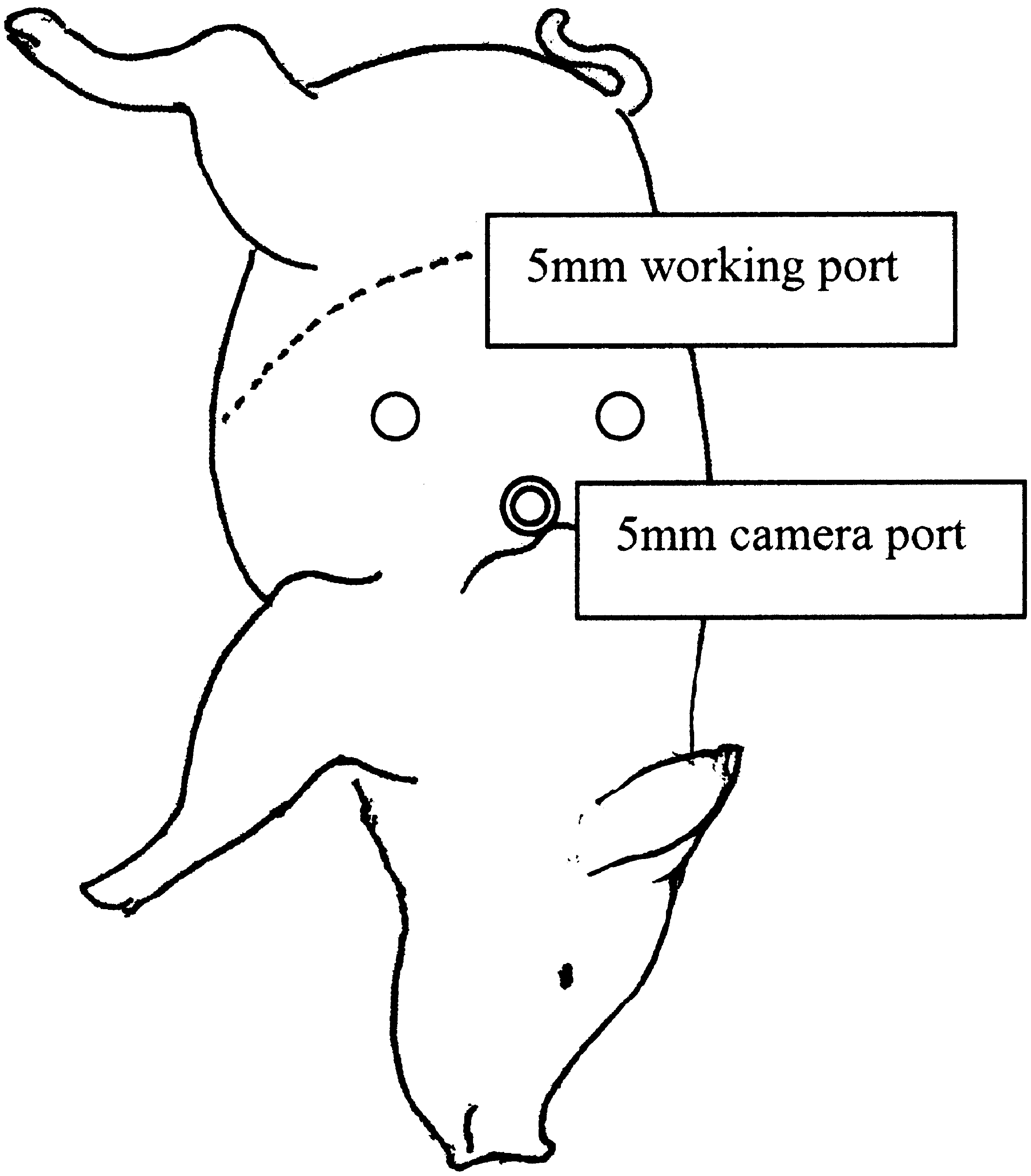
Recommended port placement for diaphragmatic hernia repair.
Esophageal anastomosis and diaphragmatic hernia repair
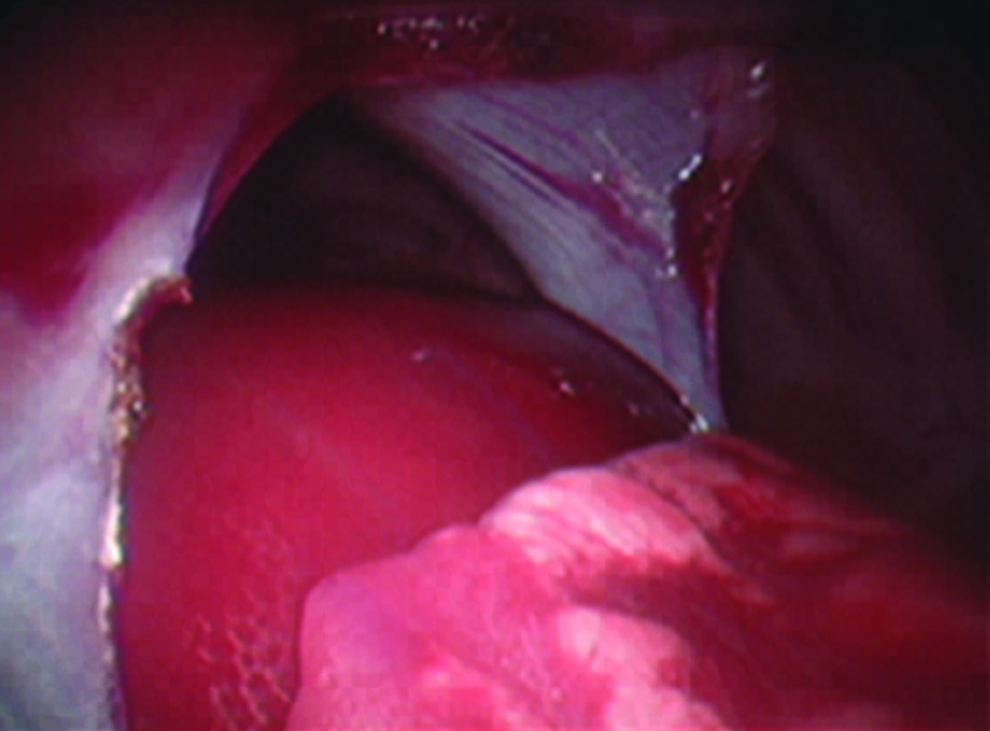
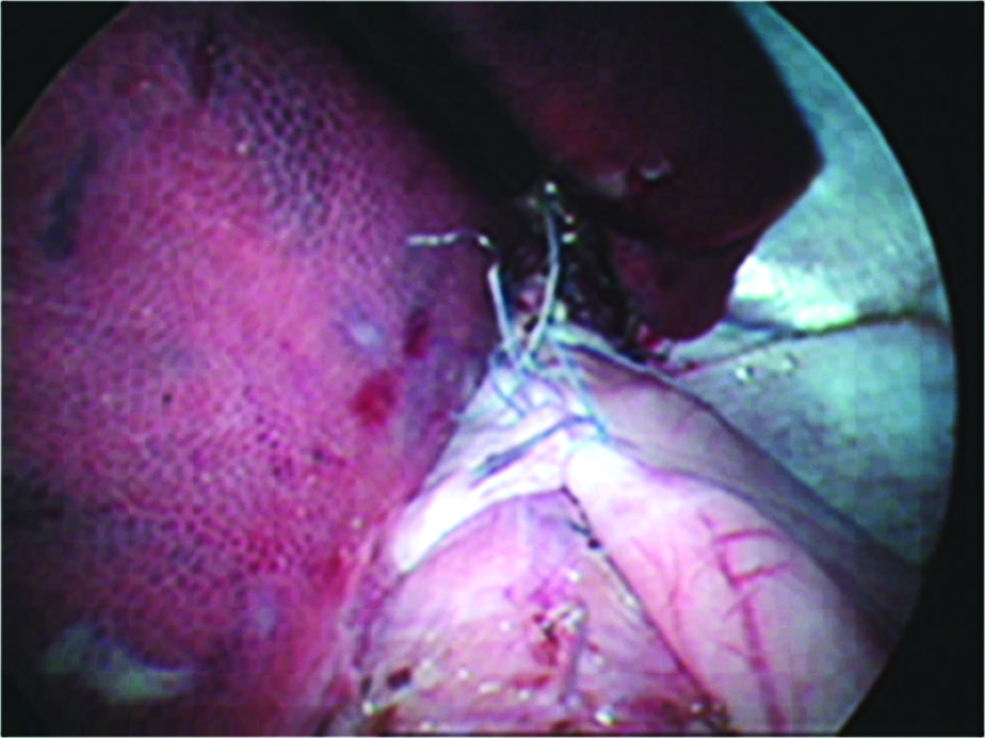
The surgery was performed using 5-mm instruments. The esophagus was identified with the aid of the orogastric tube and transected. Mobilization was avoided to reduce the tendency of the esophagus to retract back on transection. Intracorporeal suturing was done, using TI-CRON™ (nonabsorbable silicone-coated braided polyester) (Covidien) 5-0 sutures. When access was limited, the esophagus was hitched up using a TI-CRON 3-0 suture (Fig. 3). A diaphragmatic defect was then created with hook diathermy under vision over the central part of the right hemidiaphragm. The expanded incision simulated a diaphragmatic hernia (Fig. 4). This was repaired using a running mattress suture or interrupted suturing with 2-0 TI-CRON and, in one case, with Endo Stitch™ (Covidien). The angle of approach, as in neonates, was difficult. Therefore, during our earlier part of the learning curve additional ports were required to modify the working angle. The port placement sites are very important in the successful completion of surgery (Table 1).

Esophageal anastomosis.
Diaphragmatic hernia.
Lung biopsy
This was done using EndoLoop™ 3-0 PDS™ (Ethicon, Johnson & Johnson) and a vessel sealing device. Porcine lung is flimsy and bled profusely after the biopsy in one case.
Laparoscopy (transperitoneal)
The position of the animal was similar to that used in pediatric MIS, with the hind legs flexed and strapped to prevent interference with the instruments inserted through the lower abdominal ports. Primary access was created in the midline at the level of the umbilicus using the open technique. Insufflation pressures of about 8–10 mm Hg were used. Port placement for fundoplication, cardiomyotomy, pyloromyotomy, splenectomy, transperitoneal nephrectomy, and colonic biopsies were similar to those used in pediatric laparoscopic practice. Organs were not retrieved outside after completion of nephrectomy, splenectomy, and adrenalectomy. A vessel sealing device was preferred for hemostasis. Endo GIA™ (Covidien) staplers were used only when needed. The fan retractor was useful in retraction of the spleen and liver. In total, 17 pigs were used to develop the models for the following laparoscopic procedures.
Fundoplication
The creation of a fundal wrap was preceded by a splenectomy. The left and middle lobes of the liver were retracted using either a fan retractor or a grasper, inserted through the epigastrium. The anatomies of the gastroesophageal junction and the stomach were found to be very similar to those of humans (Fig. 5).
Fundoplication.
Cardiomyotomy
The esophagus is thick walled with a definite plane between the mucosa and muscular layers.
Pyloromyotomy
This procedure was performed on the greater curvature of the stomach, which has a thick wall. The spreading of the muscle layer was more challenging than that encountered in pyloric stenosis.
Splenectomy
The spleen lies horizontally across the upper abdomen and is very mobile, soft, and friable. Splenic devascularization was performed serially. The spleen was retracted as the dissection progressed towards the hilum. This was necessary to prevent the spleen from falling over, once the attachments were released.
Colonic biopsy
Multiple biopsies were taken in the left colon by tracing it back upwards from the rectum.
Nephrectomy
Nephrectomy is performed by the transperitoneal approach. The renal vein may divide outside the renal hilum, and a vessel sealing device was used for hemostasis.
Adrenalectomy
The strip-like elongated adrenal is difficult to locate. This is facilitated by releasing the lateral bowel attachments. The tail of the pancreas was identified and protected (Table 2 and Fig. 6).
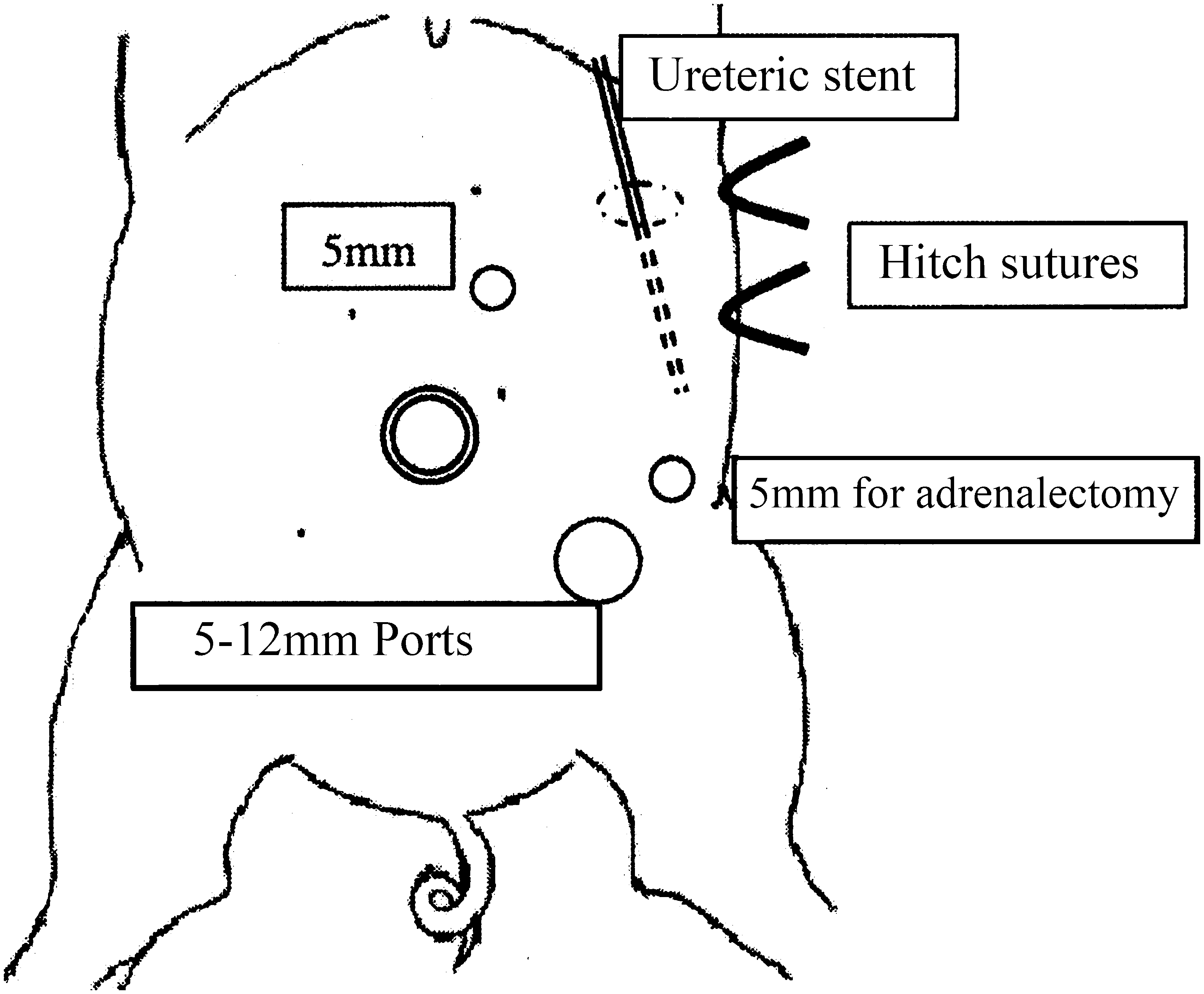
Recommended port placement for left pyeloplasty and adrenalectomy.
Pyeloplasty
The model was based on the previously reported experience of Fu et al. 4 The left side was chosen with the animal rotated to the right side. Two operating ports were used: One in the upper abdomen, approximately 3 cm to the left of the midline, and another in the lower abdomen, approximately 5 cm to the left of the midline. A small bowel loop was identified, and a conduit was created using an Endo GIA stapler to resemble a dilated pelvis. The conduit and upper ureter were hitched to the abdominal wall using a stay stitch. The upper ureter was divided and spatulated, and the bowel conduit was partially cut open at one end. Anastomosis was then performed using 4-0 Vicryl® (Ethicon, Johnson and Johnson). A 3.7 Fr. ureteric catheter was inserted across the anastomosis after completion of the posterior layer. This catheter was introduced into the abdomen using the sheath of a 16-gauge intravenous cannula from a site that is co-axial to the lie of the anastomosis (Fig. 7).
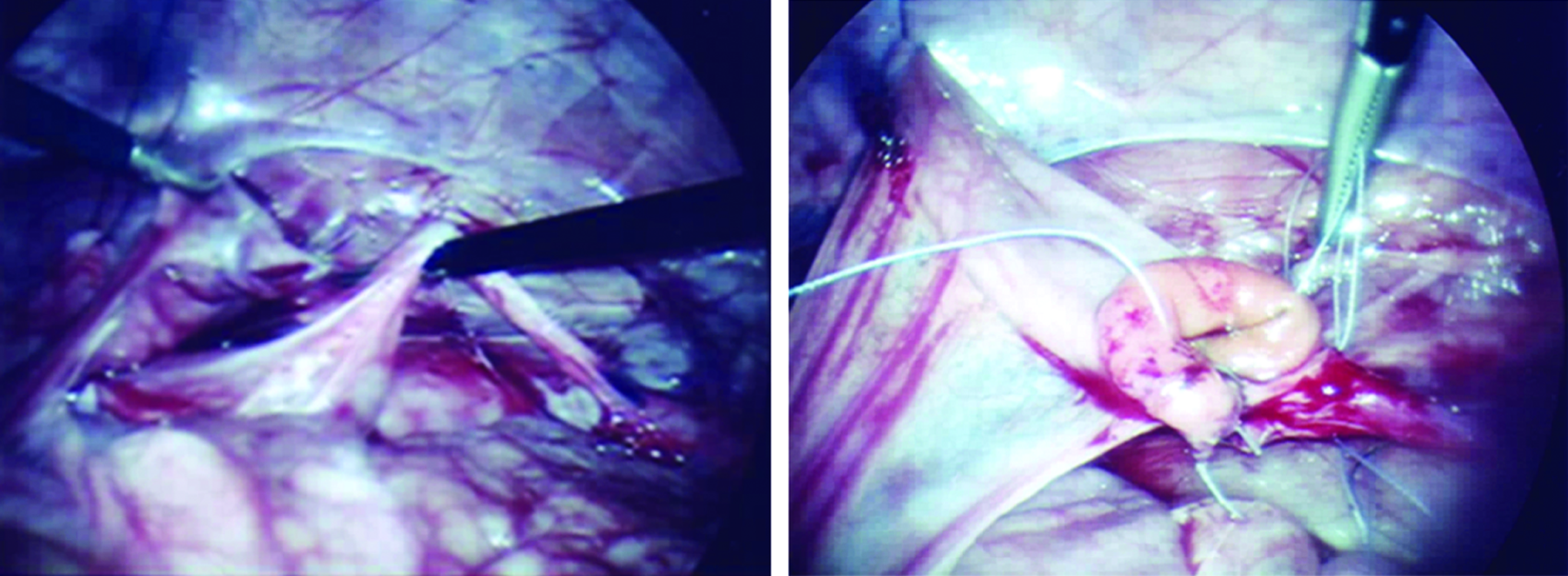
Pyeloplasty.
Cystoscopy and endoscopic injection of the ureteric orifice(s)
A female pig was required because of anatomical constraints in males. The membrane covering the ureteric orifices was incised using hook diathermy inserted transvesically. Two separate suprapubic ports were used for better visualization and diathermy. This also necessitated creation and maintenance of CO2 pneumovesicum at 8 mm Hg. Then through the 13 Fr. cystoscope a metal endoscopic injection needle 3.7 Fr×23 gauge×350 mm was inserted, and two injections were made—one 5 mm within the ureter and other at the ureteric orifice; 0.3 mL of dextranomer and hyaluronic acid combination (Deflux®) was used on each side. A stream of water was then directed at the ureteric opening via the cystoscope, and there was no hydrodilatation of the ureters.
Single-port laparoscopic surgery
A 20-kg female pig was preferred for single-port laparoscopic surgery (SPLS) procedures. The animal was placed in the supine position, and a 2-cm S-shaped skin incision was made in the midline at the level of the lowest point of the costal margin. 6 The SPLS port was well lubricated and inserted at an angle. The port was initially inserted at 90° and then swept to 180°, simulating a bucket handle action. The SPLS port can be regrasped if required. CO2 insufflation through a dedicated channel on the port helped achieve a pneumoperitoneum, and this was maintained at a pressure of 8 mm Hg and a flow rate of 1 L/minute (Table 3 and Fig. 8). In total, 6 pigs were used to develop the SPLS models for training.
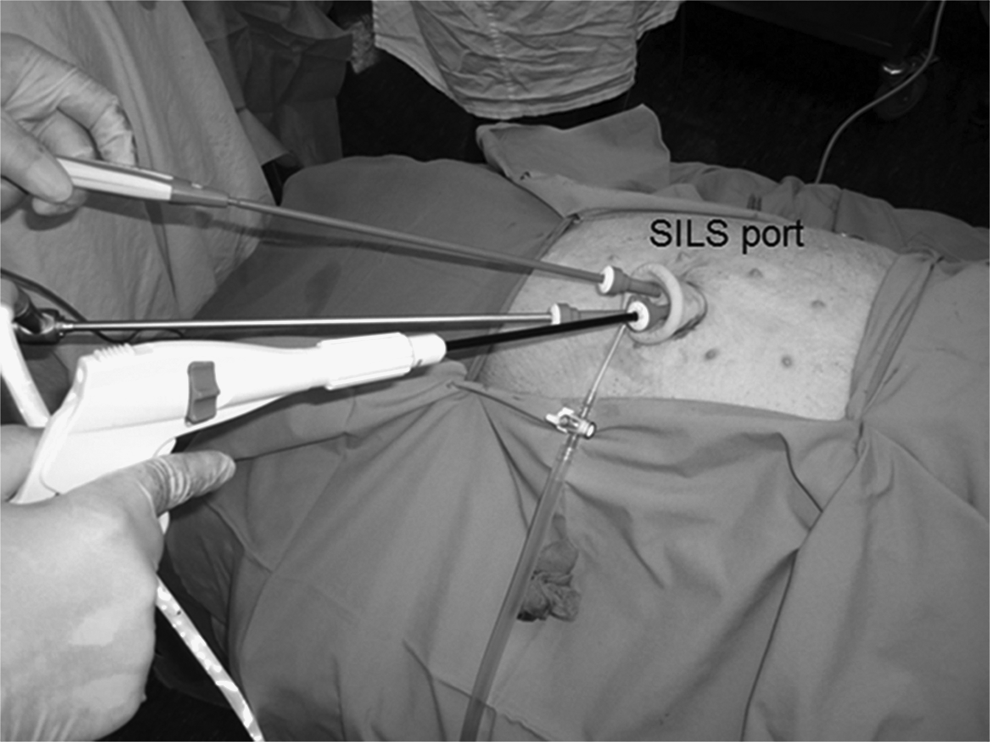
Single-port laparoscopic surgery port and instruments in use.
Cholecystectomy
A 5-mm normal needle-holder was used to take a stay stitch at the fundus of the gallbladder. The needle was brought out with the help of an Endo Close™ (Covidien) inserted as high as possible. This helped us achieve good retraction. The procedure then began with exploration of the gallbladder and triangle of Calot. A Roticulator™ Endo Grasp™ (Covidien) was used to grasp the infundibulum of the gallbladder and also to explore the triangle of Calot; the articulating action of this instrument helped in making this task safer and easier. The cystic duct, common bile duct, and the cystic artery were identified, dissected, and then clipped. A Roticulator Endo Mini-Shears™ (Covidien) was used to divide the duct and artery and later to dissect the gallbladder from the liver bed. Insertion of another instrument port to help with retraction, as attempted in one case, was found to be of little advantage. Following removal of the port, the incision was closed under vision.
The operative principles of SPLS require instruments to cross-over within the abdomen, and there is difficulty in orienting the operative field with SPLS instruments; however, this was overcome with some practice on the SPLS trainer and on the porcine model.
Cardiomyotomy
Cardiomyotomy was then attempted on the same animal. This was achieved easily with only one additional port inserted to the right of the umbilical port.
Splenectomy
In another case, splenectomy was attempted after cholecystectomy. It was achieved with only one additional port. This port was inserted below and slightly to the left of the SPLS port.
Nephrectomy
Similarly, in another case right nephrectomy was performed. The renal vein may divide outside the hilum. A vessel sealing device was used for hemostasis.
Discussion
Pediatric MIS does not offer the luxury of large numbers of patients and training by repetition in the operating room. In addition, the diversity of procedures is increasing. Tutors in pediatric surgery continue to search for a safe and reliable method to pass on skills used in advanced MIS. Porcine models offer a promising solution to this challenge. Because the visceral anatomy of pigs is similar to that of humans, pigs offer a high level of simulation in pediatric MIS. 5 They may be superior to endotrainers, which complement the animal models for training and can be used for repetitive training through workshops.
An ideal training model must provide the skills required, be universally available, and be physiologically and anatomically similar to an anesthetized patient, thereby offering a working field comparable to a patient. 7 We used animals of different sizes for different procedures. Innovations were also necessary in situations where anatomical similarity with the pathology was not possible.4,5,8 The porcine models reported here may also offer many advantages for training programs in other parts of the world. They can be directly incorporated into curricula in the form of workshops. In countries where experiments on live animals are restricted, these models may also be tried on cadaveric pigs. 9 We hope that detailed descriptions in this report will be of benefit to tutors and students in pediatric MIS around the world.
Animal models in pediatric MIS should be designed for surgeons in different levels of training. Although our models were developed by experienced surgeons, we remain optimistic about their usefulness for junior surgical trainees following our experience in recent training workshops. We propose to address this issue in a separate report, which will be submitted for peer review separately in the near future.
SPLS is being increasingly used in adult laparoscopy. We believe that SPLS will continue to be increasingly adapted in pediatric practice. It is a technique that demands a high level of dexterity, and hence a systematic, hands-on training may be of value. The models described in this article may provide a useful template for SPLS training.
In conclusion, successful use of porcine models may lead to better acquisition of minimally invasive surgical skills without interfering with patient safety and increasing the operative time.
Footnotes
Acknowledgments
Financial support was provided by Covidien Pty Ltd. The authors wish to acknowledge the contributions of Covidien Pty Ltd., Q-Med Australia, Karl Storz Australia, Craig Godfrey, Gordon Thomas, and Ms. Irene Tsang for their help with this study.
Disclosure Statement
No competing financial interests exist.