
Abstract
Abstract
The management of long-gap pure esophageal atresia (LGEA) remains controversial. An 8-month-old girl with LGEA underwent a laparoscopic and thoracoscopic gastric pull-up and esophago-esophagostomy in the right thorax combined with intrathoracic fundoplication. She was positioned supine, and three 5-mm ports were placed in the standard locations for laparoscopic Nissen fundoplication. The gastrostomy was taken down and an additional 5-mm port was inserted at the gastrostomy site. Laparoscopic gastric mobilization was performed; the short gastric and left gastric vessels were divided using harmonic shears, and the whole stomach and distal esophageal stump maintained their vascular supply via the right gastric and gastroepiploic arteries. The hiatus was enlarged by radial incisions at both cruras, and the mobilized whole stomach and distal esophageal stump were pushed up into the right thorax through the hiatus. The patient was placed in a modified prone position and three 5-mm ports were inserted into the right thorax. Via thoracoscopy, the upper esophageal pouch was dissected bluntly, and an esophago-esophagostomy was performed using interrupted 4-0 absorbable sutures and was wrapped by a 360-degree gastric fundoplication. The patient was positioned supine again, and a Heinecke-Mikulicz pyloroplasty and gastropexy were also performed laparoscopically. The patient has mild respiratory distress that requires bronchodilators; however, she is eating baby food well without vomiting. Postoperative intrathoracic gastrofiberscopy showed a well-functioning antireflux valve, and her parents are also satisfied with the cosmetic appearance of the seven small wounds. Our new procedure is feasible and is an excellent option in selected patients with LGEA.
Introduction
Recently, in many children's hospitals, up to 50% of abdominal operations can be performed using minimally invasive techniques, and thoracoscopic repair of esophageal atresia has been reported to be feasible.5,6 Further, laparoscopy-assisted gastric transposition combined with a cervical esophagogastrostomy through a mediastinal tunnel has been reported by a few institutions.7–9 Herein, to demonstrate the minimally invasive techniques, we also show the different procedures for gastric pull-up using combined laparoscopy and thoracoscopy in an 8-month-old girl with LGEA.
Case Report
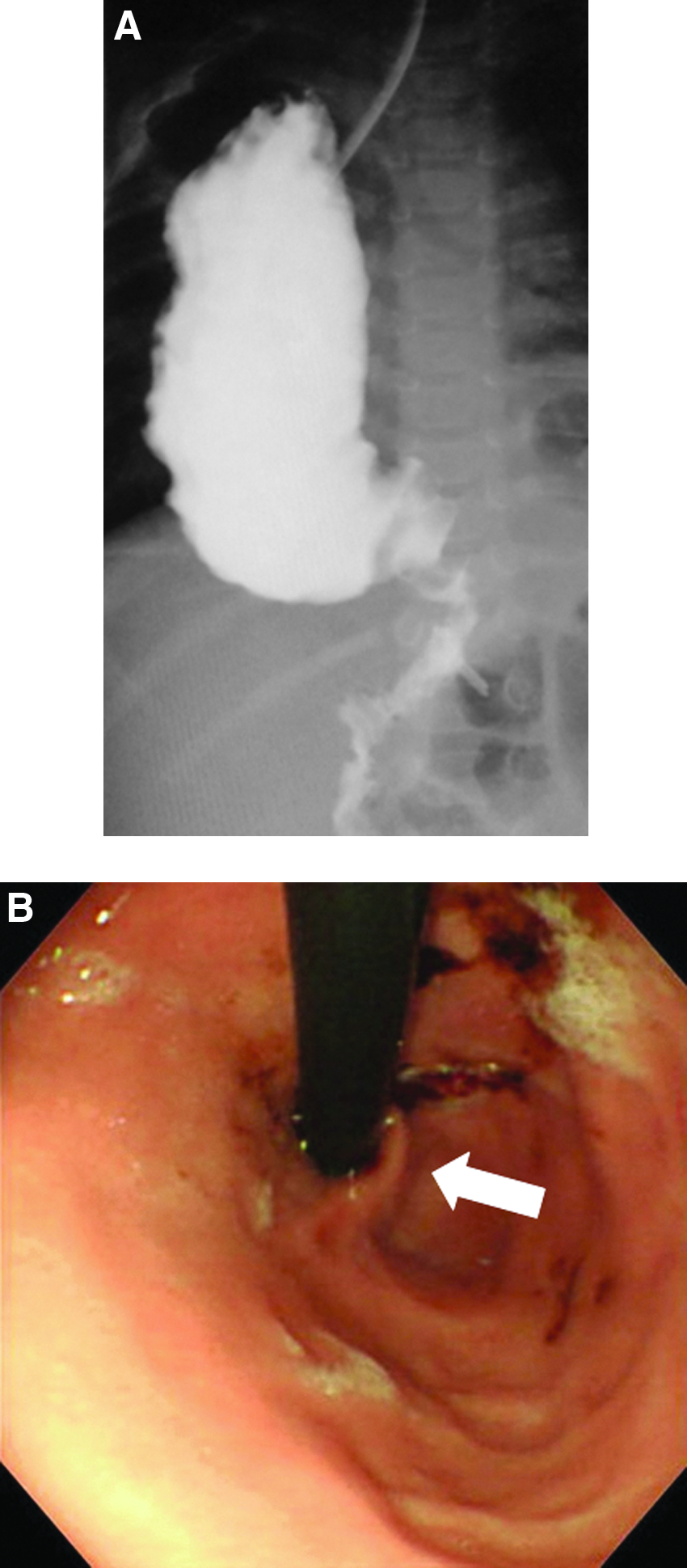
The patient was an 8-month-old girl with LGEA. Initially, she had undergone open gastrostomy insertion for enteral feeding and a salivary suction tube was introduced into the upper esophageal stump. The distance between the upper and lower esophageal stumps was more than 5 vertebrae, and the distal esophageal stump was located at the level of the esophageal inlet even after elongation via gastrostomy (Fig. 1). She was gaining weight appropriately (6.0 kg at operation), and esophageal replacement was performed.
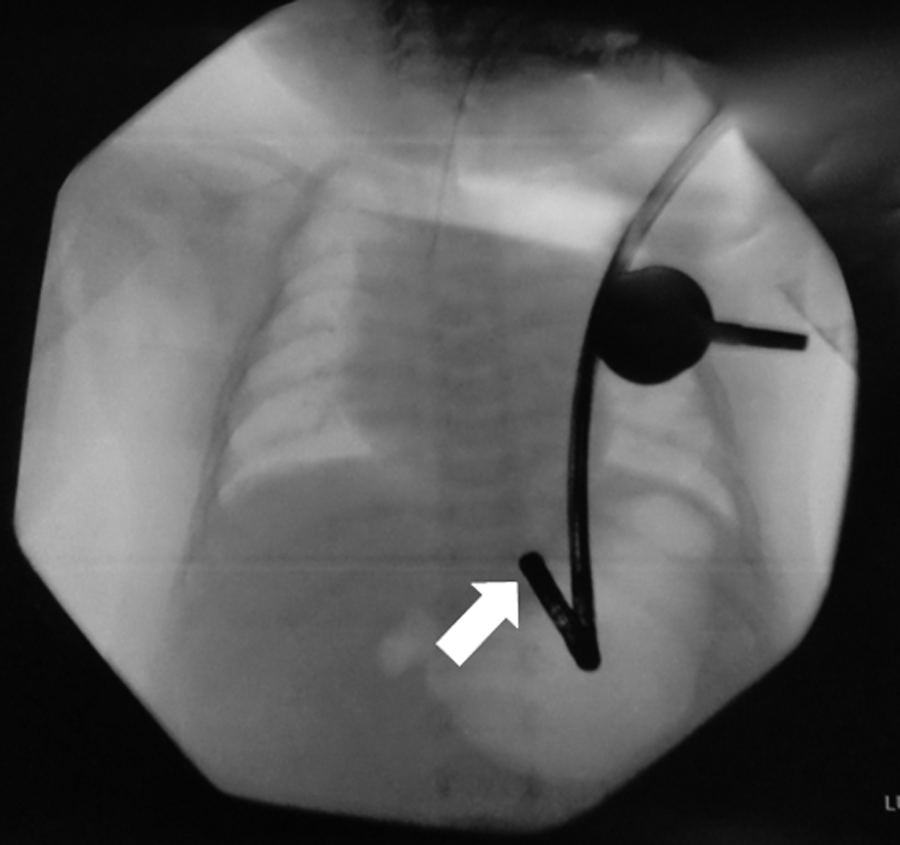
Preoperative finding of lower esophagus using gastrofiberscope via gastrostomy at 5 months of age. A very short, lower esophageal stump was suspected (white arrow).
Surgical Technique
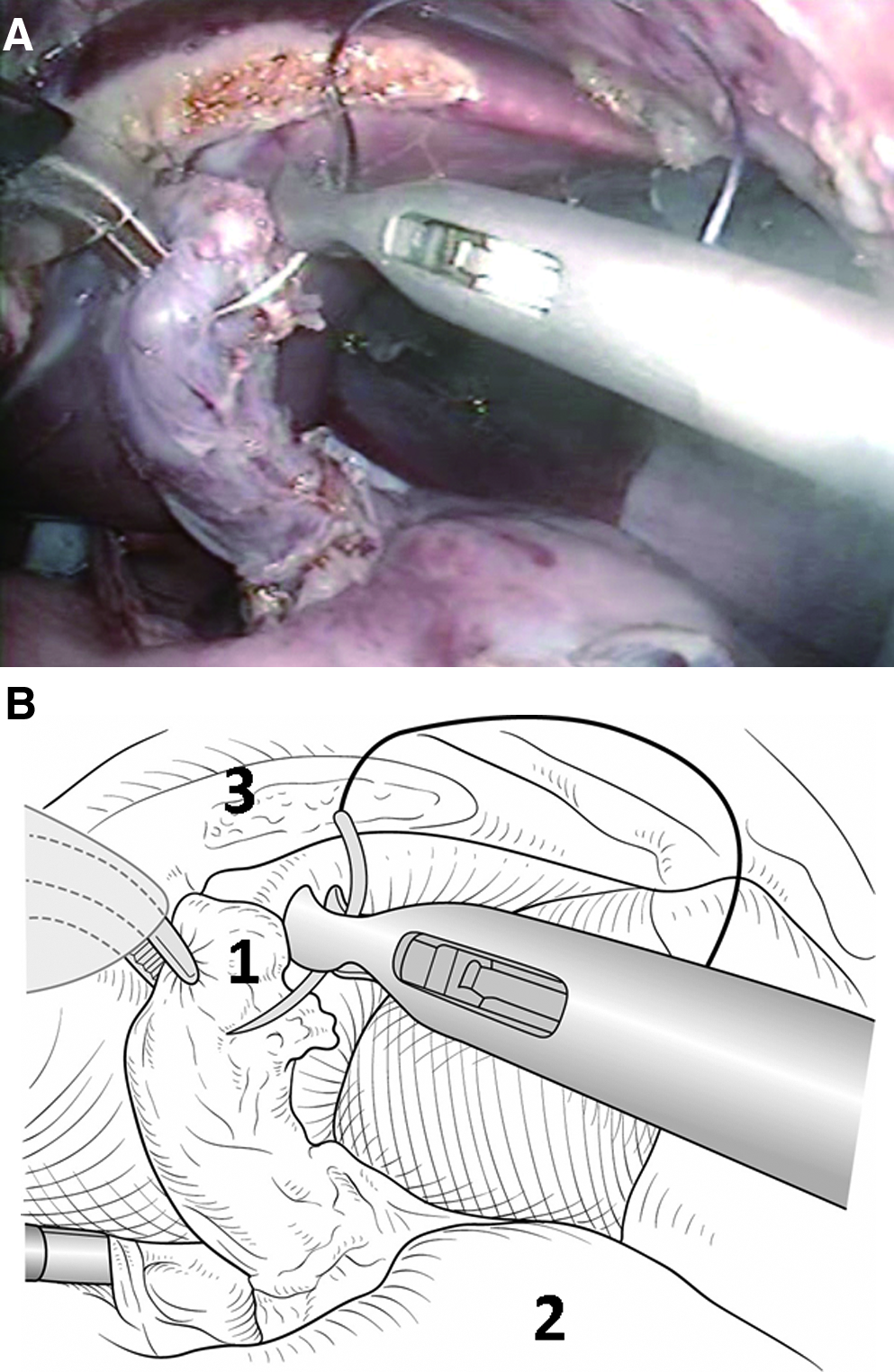
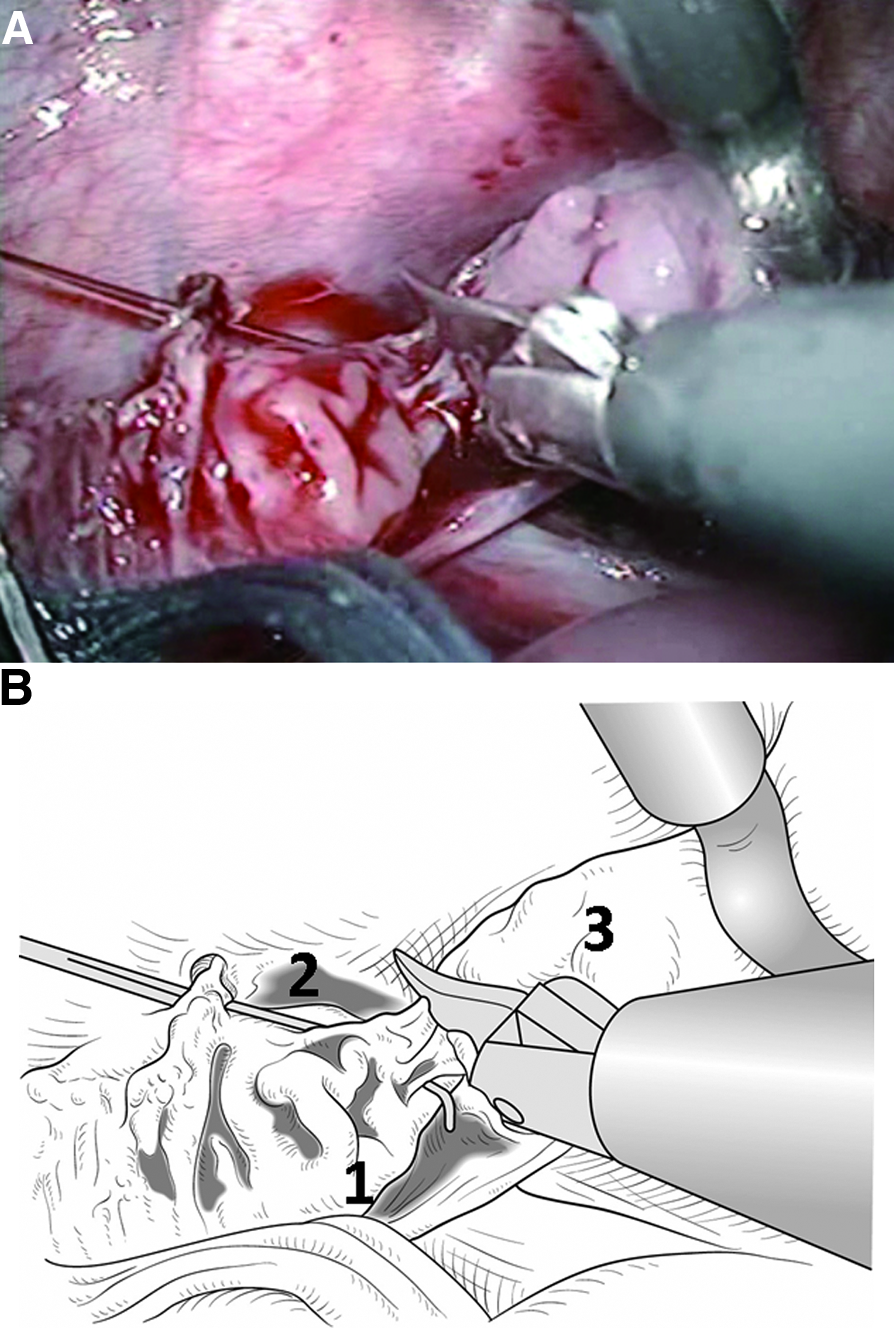
The patient was positioned supine at the end of the operating table. The first 5-mm port was inserted using the open Hassan technique from the umbilicus. The abdomen was insufflated and a couple of 5-mm working ports were placed in the standard locations for laparoscopic Nissen fundoplication. The gastrostomy was taken down from the anterior abdominal wall and was closed with interrupted 3-0 sutures, and then an additional 5-mm port was inserted through the gastrostomy site (Fig. 2). Complete gastric mobilization was performed, leaving the blood supply of the stomach via the right gastric and the right gastroepiploic vessels intact. The left gastric artery was identified and ligated. The rudimentary, lower esophageal stump was also mobilized from the esophageal hiatus by using blunt and harmonic shears. The distal esophageal stump received a triple 3-0 traction suture to allow the pull-up later (Fig. 3A, B). The hiatus was enlarged by radial incisions at both cruras using harmonic shears, and the mobilized whole stomach and distal esophageal stump were pushed up into the right thorax through the enlarged hiatus.
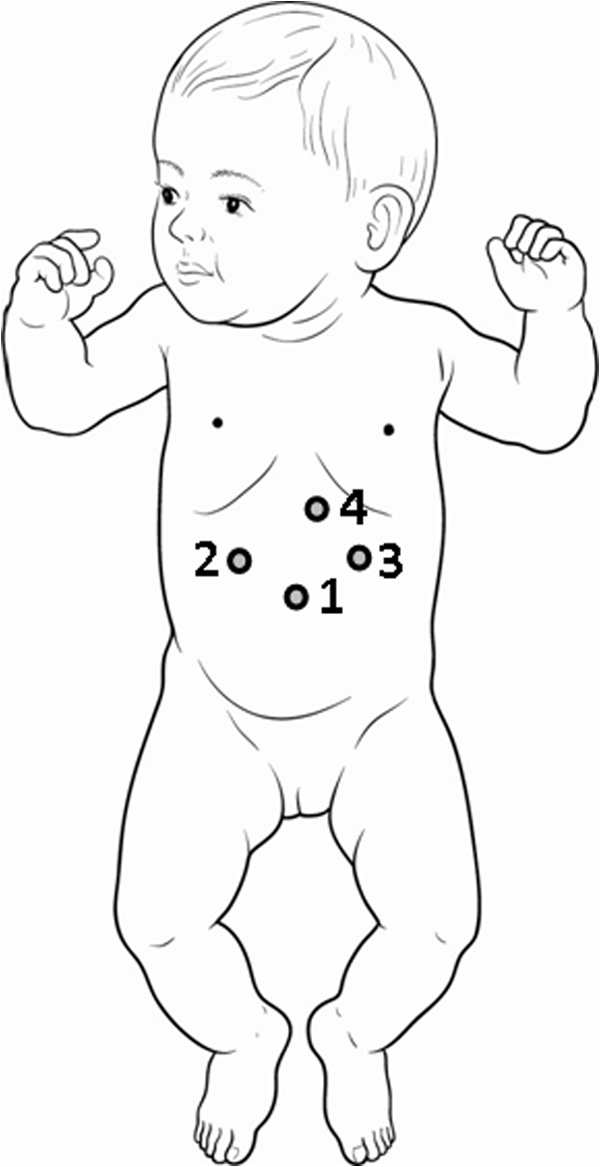
Port location of laparoscopic procedure. (1) Umbilicus: telescope; (2) and (3) upper abdomen: operator's working ports; (4) gastrostomy site: assistant's working port.
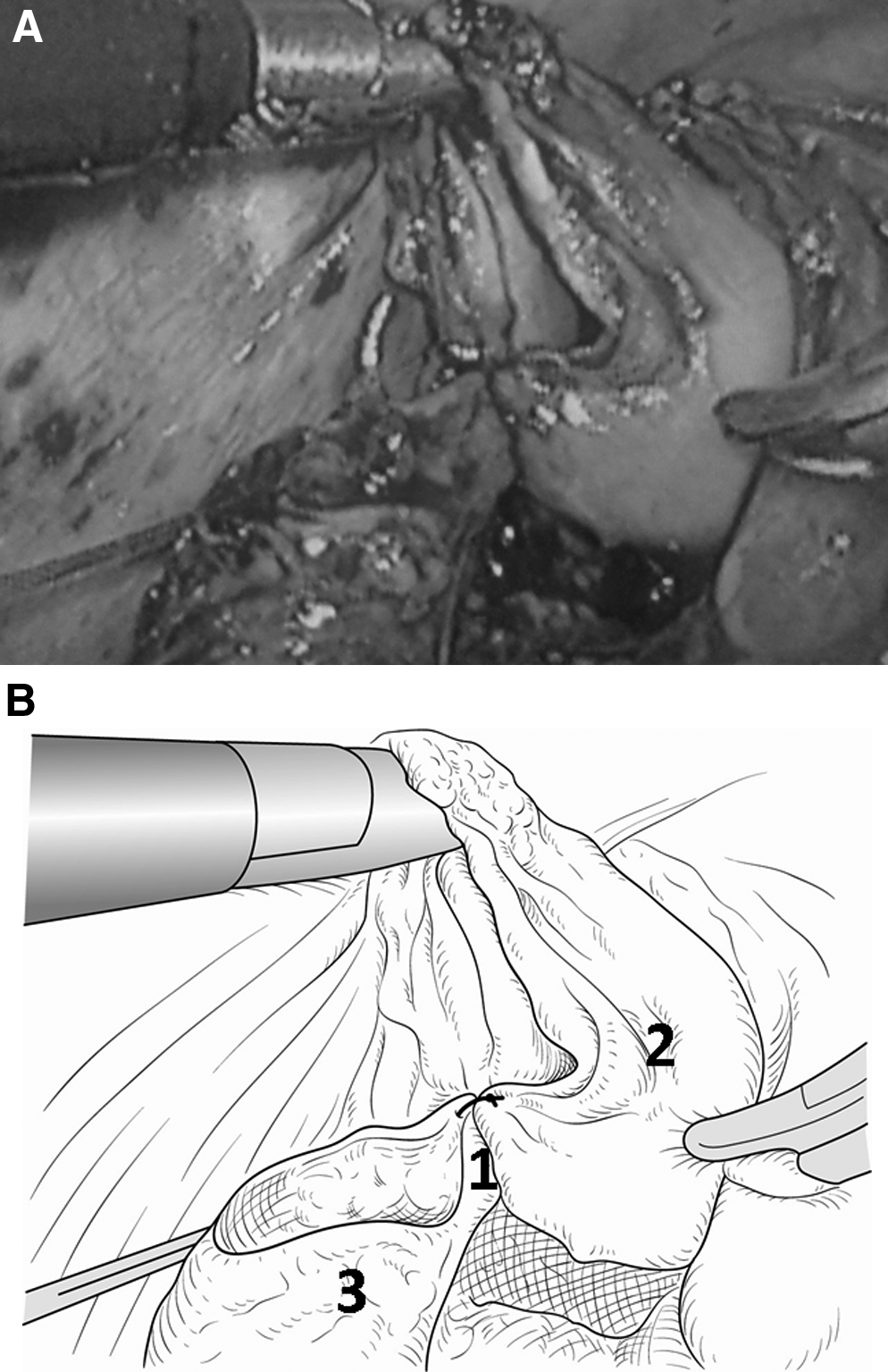
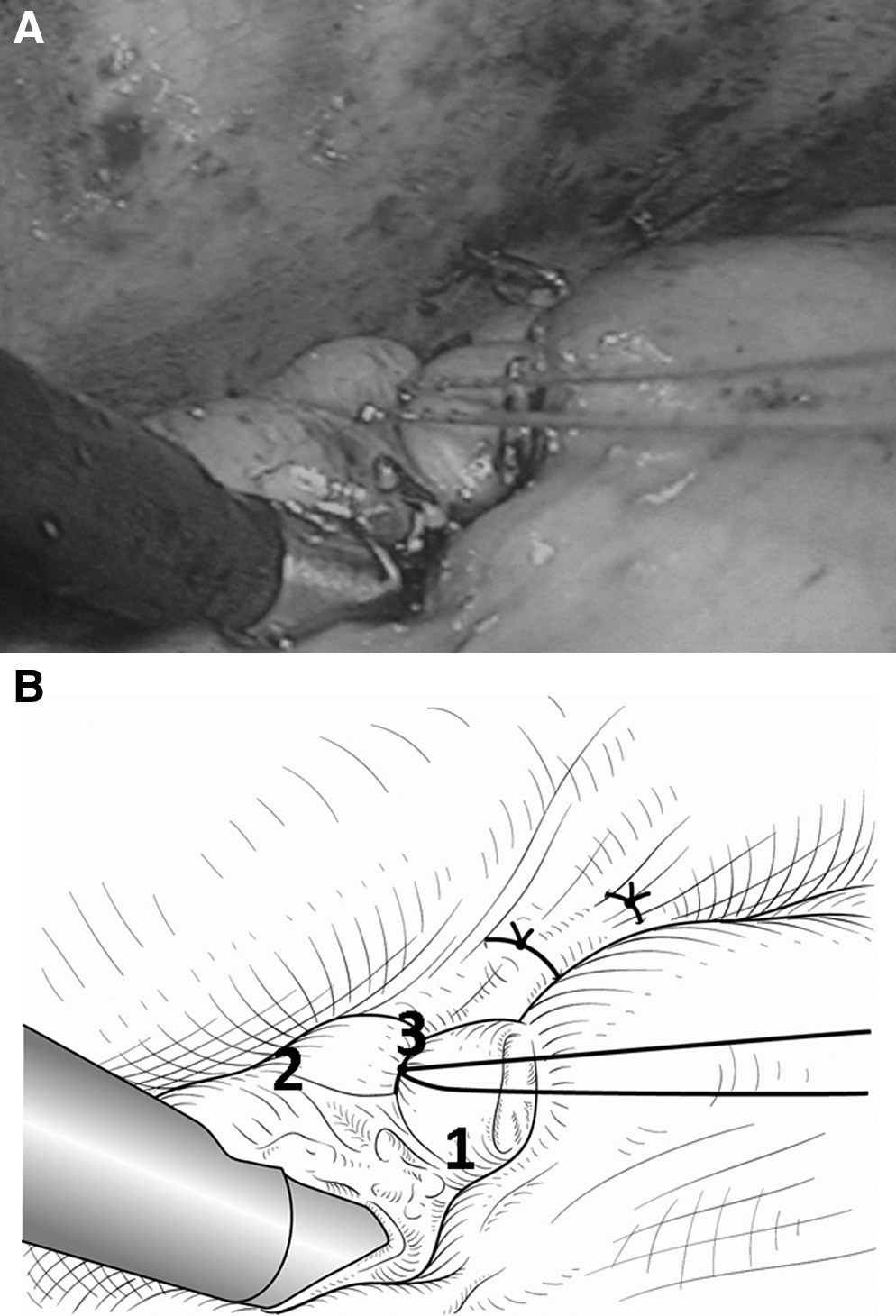
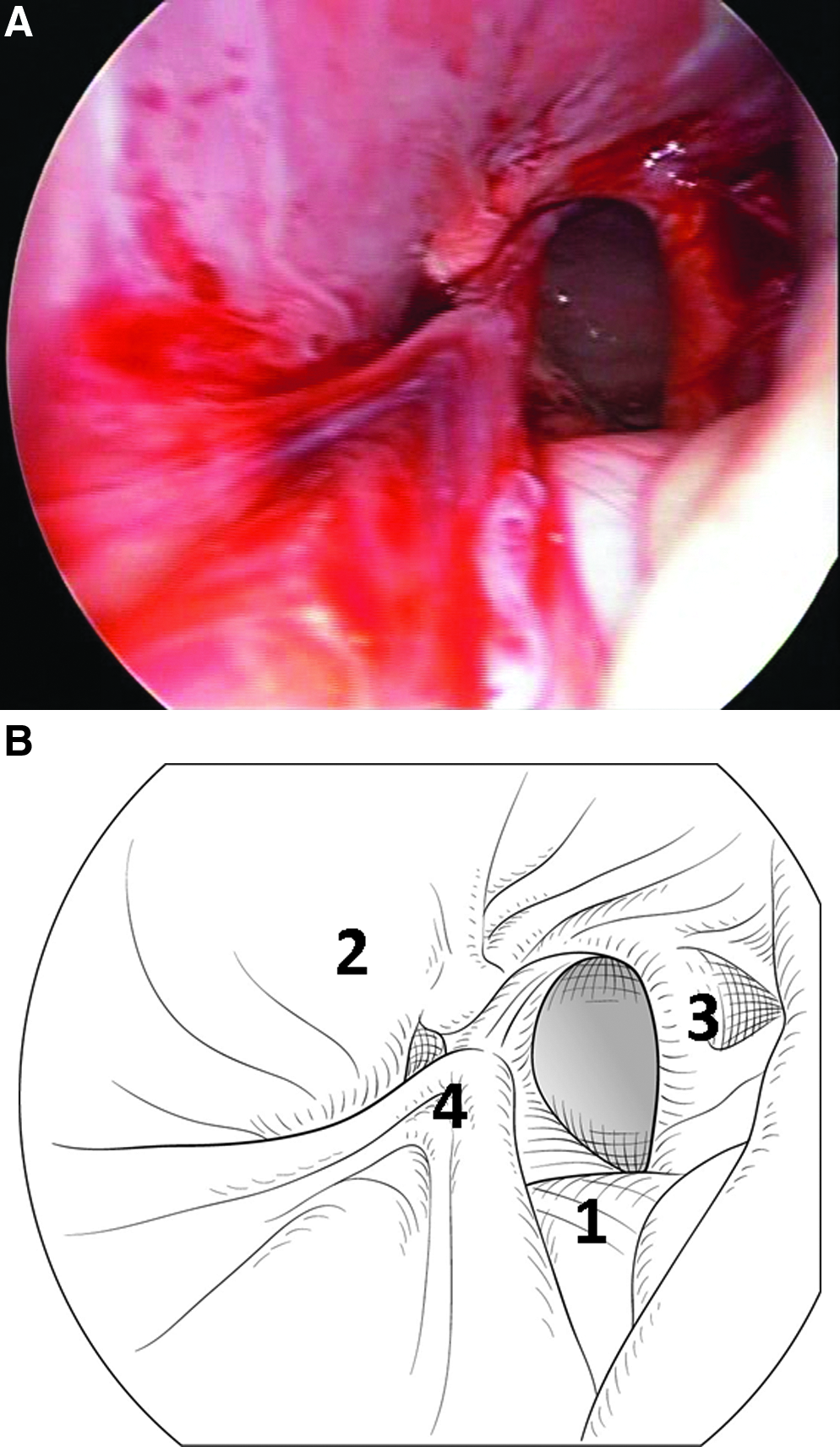
The patient was placed in a modified prone position with the right side elevated 30 degrees. Three 5-mm ports were inserted in the standard locations for thoracoscopic repair of neonatal esophageal atresia (Fig. 4). A pneumothorax with carbon dioxide at a 4 mmHg pressure sustained a mild collapse of the lungs. Via thoracoscopy the upper esophageal pouch was dissected bluntly, and then the distal esophageal stump together with the whole stomach were pulled up into the right thoracic space. The end of the distal esophageal stump with insufficient blood supply was divided using scissors, and sufficient bleeding on the cutting edge was observed (Fig. 5A, B). Esophago-esophagostomy was performed using eight interrupted 4-0 absorbable sutures (Fig. 6A, B). After a transanastomotic tube and another enteral feeding tube were inserted through anastomosis, the esophago-esophagostomy site was wrapped by a 360-degree gastric fundoplication (Fig. 7A, B).
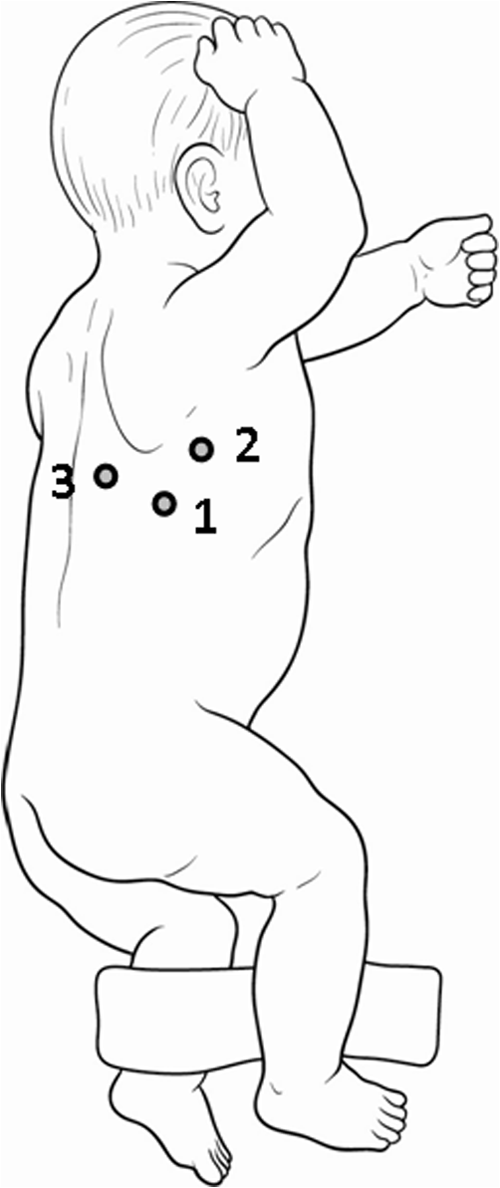
Port location of thoracoscopic procedure. (1) Two centimeters below the inferior tip of the scapula and slightly anteriorly: telescope; (2) more anteriorly from (1): operator's working port for right hand; (3) more posteriorly from (1): operator's working port for left hand.
The patient was positioned supine again and attention was turned back to the abdomen. The pulled-up stomach was found to be appropriately positioned, and the antrum was fixed to the hiatal crura using six stitches of nonabsorbable suture (Fig. 8A, B). Heinecke-Mikulicz pyloroplasty was also performed with interrupted 4-0 sutures. The operation time, including changes of patient's positioning and dressing, was approximately 6 hours.
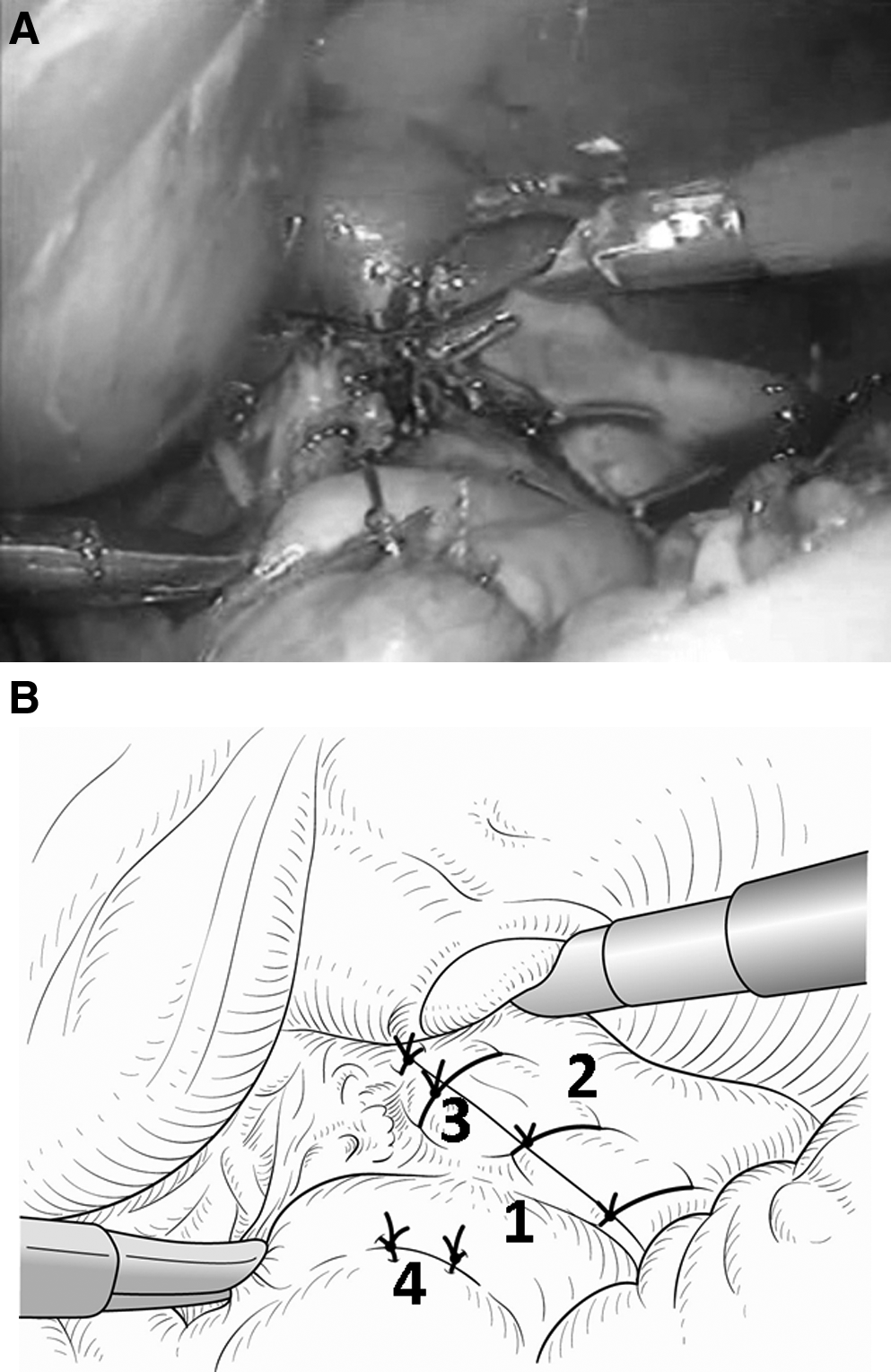
Laparoscopic view of final finding of surgery. The gastric antrum (1) was fixed to the hiatal crura (2) using six stitches of nonabsorbable suture (3). (4) Pyloroplasty.
Postoperative Course
The patient had mild anastomotic stenosis that required balloon dilatations; however, she is eating baby food well with neither vomiting nor severe respiratory distress. Postoperative intrathoracic gastrofiberscopy showed a well-functioning fundoplication (Fig. 9A, B), and her parents are also satisfied with the cosmetic appearance of the seven small wounds. Four months later, she had a left diaphragmatic hernia via an esophageal hiatus, however laparoscopic repair of the hernia was easily performed (Fig. 10A, B), and she is doing well without any complaints 1 year postoperatively.
Discussion
Esophageal replacement for LGEA is not a common surgical procedure in infants and children. The number of such patients who require this procedure is less than 10 each year in Japan. The type of graft and whether it should be located in the mediastinum or the right thorax are controversial,1–4 and dependent upon the surgeon's preferences. We prefer whole stomach for esophageal replacement, but our standard procedure for these infants during the last two decades has been gastric pull-up and esophago-esophagostomy in the right thorax combined with intrathoracic fundoplication. In a gastric pull-up for esophageal replacement (Spitz procedure),1,2,4 an antireflux valve is not created at the site of the cervical esophagogastric anastomosis. Therefore, nocturnal reflux of retained gastric contents or refluxed bile into the remnant esophagus is anticipated, 2 and these phenomena might cause an unknown number of postoperative deaths and anastomotic stricture. When making an antireflux valve around the distal esophagus, the thickness of the upper stomach becomes larger and the stomach pulled up through the narrow mediastinum might cause respiratory distress and difficulty of swallowing. Our procedure combined with construction of an antireflux valve is expected to prevent gastroesophageal reflux (Fig. 9B), so we chose the intrathoracic route for esophageal replacement. However, the esophago-esophagostomy of our procedure in the right thorax is thought to have the disadvantage that it would be more difficult to control an anastomotic leakage than it would be in the esophagogastrostomy of the Spitz procedure in the neck. So we always divide the distal esophageal stump in order to maintain a good blood supply before esophago-esophagostomy in order to decrease a chance of anastomotic leakage (Fig. 5).
Although pyloromyotomy is always performed simultaneously in our procedure, the appropriate gastric outlet is often disturbed because the whole stomach is vagotomized and atonic within the postoperative 3–6 months (Fig. 9A). However, frequent feeding with small amounts of food prevented postoperative severe respiratory distress and delay of gastric contents in all of our previous 5 patients, and they are eating well and do not have any respiratory problems in long-term follow-up.
Minimally invasive surgery has been introduced in many kinds of pediatric diseases. Thoracoscopic repair of esophageal atresia has already become a common procedure in neonates,5,6 and the short-term outcome of this procedure is excellent with quick postoperative recovery and better cosmetic results. Recently, a laparoscopic Spitz procedure has been reported from a few institutes,7–9 and a laparoscopic direct view of the middle mediastinum provides a better advantage compared to that of the original open Spitz procedure. 8 However, the laparoscopic Spitz procedure requires blunt digital dissection from the cervical incision toward the mediastinal dissection plane and dilatation using Hegar dilators in order to join the upper and lower dissection planes. 9 Our thoracoscopic procedure reveals more clearly both the upper esophageal pouch and lower esophageal stump that is pushed up via the esophageal hiatus from the abdominal cavity, and the thoracoscopic esophago-esophagostomy and the construction of the antireflux valve are easier and safer because of the visibility of all maneuvers. Also, our procedure requires just seven small incisions on both abdominal and thoracic walls without any cervical incision. Our patient had a postoperative left diaphragmatic hernia due to loose-anchoring sutures between the gastric antrum and thoracic inlet. The hiatus should be adequate in size so it does not constrict the pulled-up stomach, while, at the same time, it should be small enough to prevent herniation of intraabdominal organs into the thoracic space. Thus the precise suturing of the stomach and hiatus in order to prevent herniation should be carefully planned.
Our laparoscopic gastric pull-up and thoracoscopic esophago-esophagostomy with intrathoracic fundoplication is feasible and might be an excellent option in selected patients with LGEA. Long-term follow-up to gain more experience is mandatory.
Footnotes
Disclosure Statement
No competing financial interests exist.