
Abstract
Abstract
Background:
The procedure of inguinal herniorrhaphy is the most common procedure performed by pediatric surgeons today. Laparoscopy has proved to be both sensitive and specific for evaluating the contralateral inguinal region. Despite the attractiveness that transinguinal laparoscopy offers and the success it has seen, we report a series of hernias after the utilization of this tool.
Methods:
After IRB approval, a retrospective review of our institutions' experience from 1/2002 to 6/2010 with children who underwent unilateral inguinal hernia repair with contralateral evaluation with laparoscopy was completed. Data recorded included sex, age of initial presentation, laterality of initial hernia, age at second presentation, and operative time of initial surgery.
Results:
From 2002 to 2010, 1291 patients underwent unilateral inguinal hernia repair with negative laparoscopic evaluation of the opposite ring. There were 32 patients (2.5%) who subsequently presented with an inguinal hernia on the contralateral side. All were men. The average age of initial presentation was 42.7 months. The mean time to occurrence of the contralateral hernia was found to be 16.7 months with a median of 12.2 months. The mean operative time for the initial operation was found to be 25.6 minutes.
Conclusions:
When using laparoscopy to explore the contralateral inguinal region, the surgeon should be aware that a negative exam may still be associated with a small chance of clinically developing a hernia.
Introduction
Methods
After IRB approval, we conducted a retrospective review of our institutions' experience from 1/2002 to 6/2010 with children who underwent unilateral inguinal hernia repair with contralateral evaluation with laparoscopy. Data recorded included sex, age of initial presentation, laterality of initial hernia, age at second presentation, and operative time of initial surgery.
The general method of diagnostic evaluation in this cohort is to place 4-mm non-disposable cannula. The cannula is introduced into the ipsilateral hernia sac and guided through the internal ring followed by carbon dioxide insufflation of the peritoneal cavity. One surgeon's hand routinely insufflates with a red rubber catheter. A 2.7-mm rigid telescope with a 70° lens is then used to visualize the contralateral internal ring. Figure 1 represents a patient with no contralateral patent processus who subsequently developed an inguinal hernia. Patency is defined as an open tunnel into the contralateral inguinal region. If a peritoneal veil occludes the visualization, then a small probe or needle is introduced in the contralateral lower abdominal quadrant under direct visualization to retract the veil. After evaluation, the pneumoperitoneum is released, and a high ligation of the inguinal sac is completed. The contralateral groin is explored, and a high ligation is performed if laparoscopy revealed a patent processus.
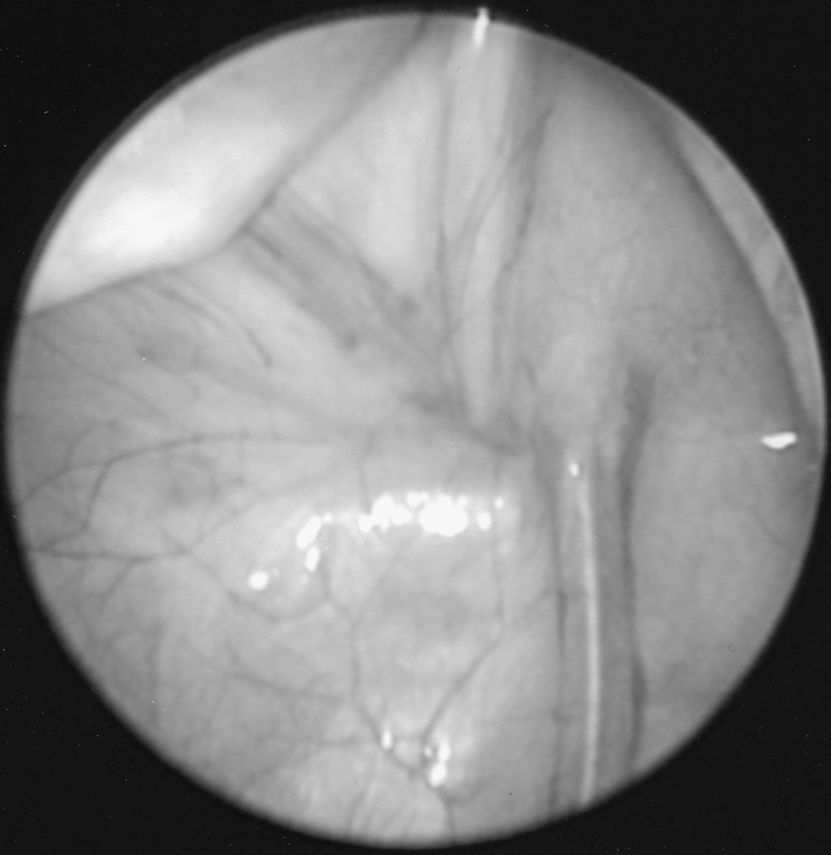
This photograph was taken at the initial repair and evaluation of the contralateral hernia. There is clearly no contralateral patent processus visible. The patient went on to subsequently develop an inguinal hernia on the contralateral region 7 months later.
Results
A total of 1291 patients underwent unilateral inguinal hernia repair with negative laparoscopic evaluation of the opposite ring from 2002 to 2010. There were 32 patients (2.5%) who subsequently presented with an inguinal hernia on the contralateral side. All were men. The average age of initial presentation was 42.7 months. Figure 2 represents the distribution of ages for initial inguinal hernia presentation. The mean time to occurrence of the contralateral hernia was found to be 16.7 months with a median of 12.2 months. The mean operative time for the initial operation was found to be 25.6 minutes.
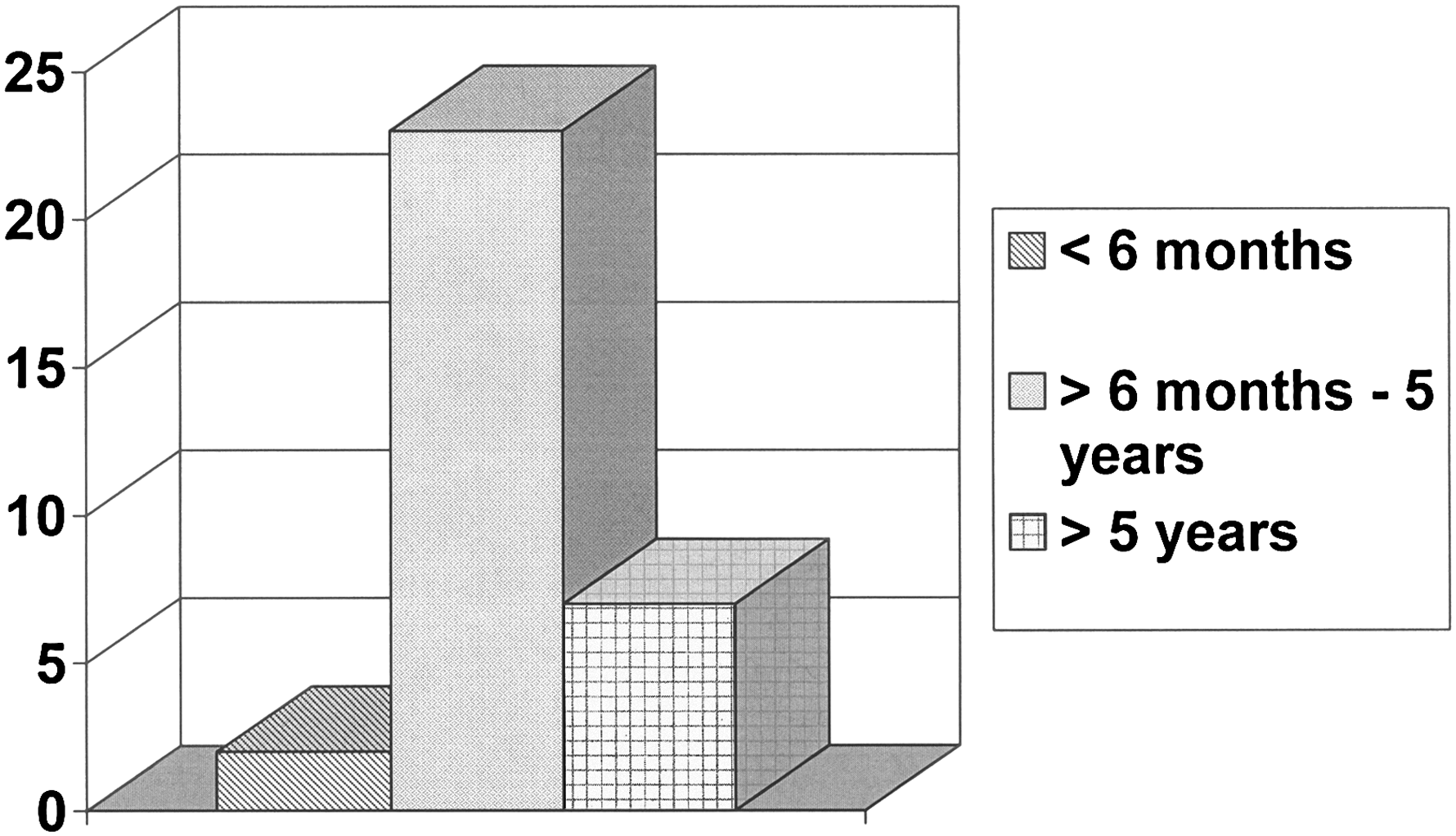
Age distribution of initial presentation of inguinal hernia.
Discussion
Over the years, several methods have been developed to determine the presence of a contralateral patent processus vaginalis. These include Bakes dilators, peritoneal insufflation, exam under anesthesia (“silk glove sign”), and, most recently, laparoscopy.4,10–13 Two methods of laparoscopy have been described: umbilical and transinguinal. The more commonly used technique is the transinguinal approach. This has been found to provide equivalent evaluation of the contralateral inguinal region while avoiding a second incision.11,12,14 Approximately 37% of pediatric surgeons now routinely employ laparoscopy. 15 This obviates the role for open contralateral exploration, which carries risks including reduction in testicular size, frank atrophy, damage to the vas deferens, and post-operative high riding testis.8,16,17
Despite these advances and success with laparoscopy, the natural history of patent processus vaginalis continues to be unknown. The frequency of contralateral patent processus vaginalisis' ranges between 20% and 50%.9,18–20 The incidence approaches 100% in premature infants. 21 Multiple studies have tried to address this risk and have found that 4%–30% of patients will develop a clinically symptomatic hernia requiring surgery.2,4,8,17,22 These studies are limited by biases including retrospective data collection and imperfect follow-up. Therefore, the presence of a contralateral patent processus is not equivalent to a hernia.
Our previously published data support laparoscopy as a safe, sensitive, and specific tool, but it does have limitations. This is due to the lack of understanding of the CPPV and the development of metachronous inguinal hernias. Our findings suggest that despite a negative CPPV found on laparoscopy, there does exist a tangible and under-reported percentage of children who will develop a contralateral hernia within 16 months of initial repair. We can only hypothesize why these hernias are occurring. The obvious hypothesis is that insufflation under pressure creates a parachute effect or over distention of the CPPV, which would appear to obliterate the potential tunnel effect of a shallow patent processus. However, the use of minimal inflation pressure with a hand-held red rubber catheter does not eliminate this risk.
Conclusion
Laparoscopic evaluation of the contralateral inguinal region continues to gain acceptance as noted in a recent review of the current literature from 1995 to date. 23 Unfortunately, when using laparoscopy to explore the contralateral inguinal region, the surgeon should be aware that a negative exam may still be associated with a small chance of clinically developing a hernia. Our series, a long-term prospective series, documents a 2.5% risk of a false negative exam which allows surgeons to inform families that this risk exists.
Footnotes
Acknowledgments
The authors would like to thank Dr. Susan Sharp, Ph.D., and Linda Jankowski for their help and support in procuring data for this article. In addition, they thank Jeannette Whitney for helping with preparation of the figures for this article.
Disclosure Statement
No competing financial interests exist.