
Abstract
Abstract
Background:
Laparoendoscopic single-site surgery (LESS) remains limited to a few relatively simple procedures in the field of pediatric surgery. We performed LESS pyeloplasty in children using conventional straight instruments and ports, and reviewed the perioperative data to evaluate the feasibility of this technique in pediatric patients.
Methods:
Twenty-two consecutive patients with unilateral pelvic ureteral junction obstruction underwent LESS pyeloplasty. Their ages ranged from 2 to 134 months (mean: 56.9 months). Two 3-mm and one 5-mm conventional ports were placed in the single incision inside the umbilicus. Conventional 3-mm laparoscopic instruments and a 30-degree 5-mm camera were used for Anderson-Hynes pyeloplasty. A F4.7 or F3 pigtail stent was introduced through one of the instrument ports. A drainage was placed next to the anastomosis, which exited via the umbilical ring incision. The stent was removed 6 weeks postoperatively.
Results:
All cases were successfully completed with no need for extra-umbilical incisions. The mean operative time was 198 minutes (range: 150–270 minutes). All patients could tolerate oral food intake on postoperative day 1. One case (4.5%) developed symptoms of anastomosis obstruction and required open renal stoma. No other significant complications occurred.
Conclusion:
LESS pyeloplasty is technically feasible in children. However, further experience and longer follow-up are necessary to appropriately evaluate the benefits and limitations of this technique.
Introduction
In adults, LESS has been used for complex procedures like pyeloplasty, prostatectomy, and others.4–6 However, reports in children have been mostly confined to relatively simple procedures such as varicocele 7 or simple nephrectomy. 8 We have performed 22 consecutive pyeloplasties for pediatric hydronephrosis using LESS. Here we review the perioperative data to evaluate the feasibility of this procedure in children.
Patients and Methods
Patients
From December 2009 to August 2010, 22 consecutive patients with hydronephrosis underwent laparoscopic pyeloplasty using LESS. Patients < 2 months old were not included in this assessment as open pyeloplasty was performed in these cases. The mean age of all 22 patients (18 boys and 4 girls) was 56.9 months (range: 2–134 months), 5 of whom were under 1 year of age. The mean body weight of the patients was 20.8 kg (range: 5–38 kg). The vast majority of hydronephrosis cases were on the left side (n=20). While 12 patients presented with recurrent flank pain, the others cases were detected by ultrasound. Pelvic ureteral junction obstruction was confirmed by ultrasound imaging study, diethylenetriaminepentaacetic acid isotope renograph, and magnetic resonance urography. Multiple ultrasounds measuring pelvic width were performed, and the smallest dimensions were recorded. According to ultrasound imaging, the pelvic width of patients was between 11.7 and 64.1 mm (mean=26.5 mm).
Surgical techniques
The patients were secured supine on the table with the affected side elevated by 30 degrees, accomplished by packing from underneath. A 2-cm semicircle incision was made on the circumference of the umbilical ring on the opposite side of the hydronephrosis. The 0.5-cm middle part of this incision was cut open with cautery alongside the navel canal to the peritoneum, with the muscle fiber pushed to its outside. A purse string was made on the fascia and peritoneal layer, and a 5-mm port was inserted and secured by the string. Pneumoperitoneum was established and a 30-degree straight camera was inserted. Two 3-mm ports were inserted at the ends of the semicircle incision. Straight 3-mm instruments were used for the procedures (Fig. 1).
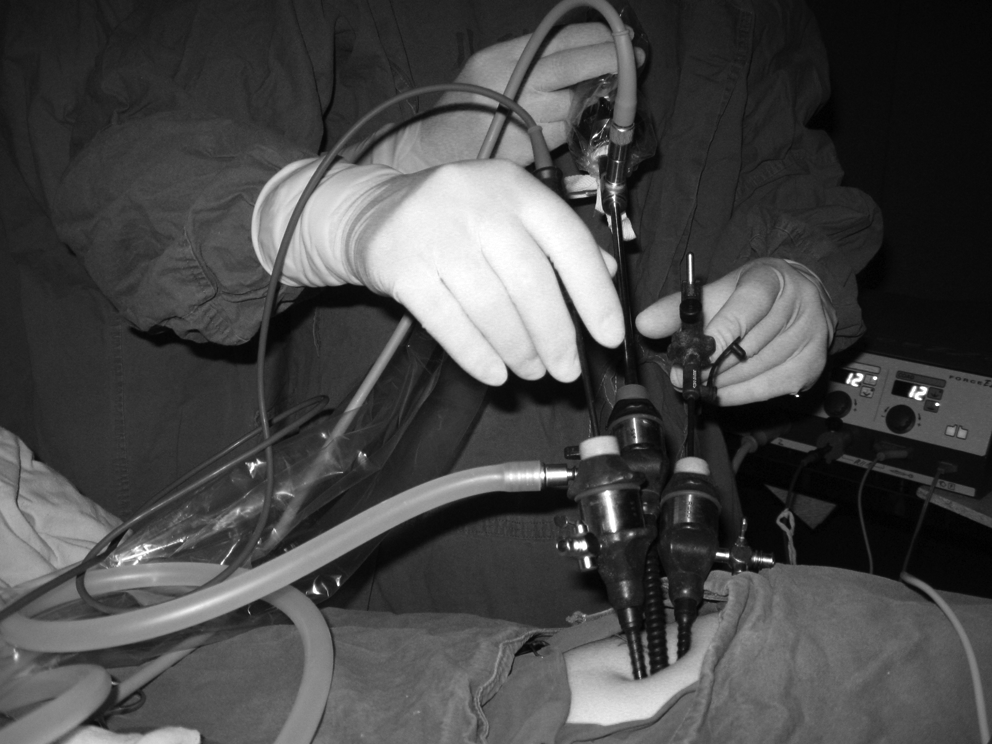
Conventional 3- and 5-mm ports and instruments were used in laparoendoscopic single-site surgery pyeloplasty in children.
When treating a left hydronephrosis, the kidney or pelvis could usually be seen underneath the mesocolon. A window was made at the avascular area of the mesocolon, which permitted the mobilization and elevation of the pelvis to the peritoneal cavity through this mesocolon window. 9 For patients in whom the pelvis or kidney could not be discerned through the mesocolon, the retroperitoneum was opened outside of the descending colon, mobilizing the colon toward the midline, and exposing the pelvis. During treatment of a right hydronephrosis, the retroperitoneum between the colon and the liver was opened, and the hepatic flexure of the colon was mobilized inferiorly and medially to expose the pelvis. After the pelvis was sufficiently exposed, it was elevated up to the abdominal cavity for further manipulations by a traction suture introduced through abdominal wall attached to the rostral side of the pelvis.
The pelvis and upper ureter were dissected free of the adipose tissue. Pyelotomy was carried out on the pelvis distal to the traction suture, leaving a width of approximately 2 cm of pelvis attached to the kidney. The pelvic ureteral junction was opened vertically by scissors, starting from the resected pelvis over the stenosis section to the normal part of the ureter. The distal pelvis remained attached to the ureter for grasping. Subsequently, the lowest point of spatulated ureter was sutured to the dependent point of the pelvis by 5-0 vicryl. The posterior side of the anastomosis (which faces the camera) was carried out first. The highest point of the distal ureteropelvic junction of the posterior side of the pelvis was sutured to the dependent part of the proximal pelvis, and closed by interrupted suture of 5-0 vicryl. Another traction suture was introduced through abdominal wall to pull up the anterior side of the pelvis. A F4.7 or F3 pigtail stent was introduced through one of the instrument ports to stent the ureter. The anterior side was closed in the same fashion from the lowest point up to meet the highest point of the anastomosis of the posterior side. The redundant distal pelvis was removed. The remaining pelvic opening is closed by a running suture. To complete the operation, a draining tube was placed beside the anastomosis, through the hole made by 3-mm port in the umbilical ring incision (Fig. 2). The stent was removed 6 weeks postoperatively.

Draining tube was placed in the umbilical incision after the completion of the procedure.
Results
All cases were successfully completed without the need for extra-umbilical incision and no cases of conversion. All patients could tolerate oral food intake on postoperative day 1. The mean operative time was 198 minutes (range: 150–270 minutes), while the mean postoperative hospital stay was 6.4 days (range: 4–10 days).
Perirenal drainage was kept for 4–9 days (mean=5.6 days). Most patients (19/22) had a minimal volume of drainage (<20 mL/24 hours), while the remaining 3 patients (13.6%) had a draining volume ranging from 21 to 47 mL per 24-hour period. Six patients (22.2%) had postoperative temperature over 37.5°C for a combined total of 14 days. In 2 of these 6 patients (9.1% of sample), the temperature exceeded 39°C for a total of 3 days; moderate extravasation was noted on ultrasound in both patients. However, by keeping the urethral catheter draining efficiently, the temperature swiftly returned to normal.
All patients eventually had the pigtail stent removed. Only one patient (4.5%) developed symptoms of anastomosis obstruction, for whom a renal stoma was placed through the flank incision. No other significant complications occurred in all cases.
Discussion
Recently LESS has been used for pyeloplasty in adults. One author has compared this new technique with traditional laparoscopic pyeloplasty, 10 reporting similar perioperative outcomes. At present there are few reports of LESS pyeloplasty in children. 4 One of the reasons for this dearth of data could be the lack of specially designed multichannel ports for children. Currently, commercially available ports usually have one 10-mm channel and two 5-mm channels, both of which are too large for younger children and infants. There are reports of using several low-profile ports in the single incision for LESS, which could minimize the clashing of the ports. We currently do not have this port and have used conventional ports of different length to place the thicker ends of each port at different heights to achieve this effect. The oldest patient in our group was an 8-year-old boy weighing 38 kg. In young or thin children, since the volume of abdominal cavity is small, a 3-mm instrument could easily reach the pelvis and was adequate in our series of patients. Additionally, usage of another 3-mm port and instruments could further increase the freedom of movement during the procedure.
Ponsky et al. 11 used LESS in children for various procedures. In their report, up to 4 ports were placed in the umbilical incision for splenectomy and cholecystectomy. In the current study, the use of two transabdominal sutures for the traction of the pelvis was helpful in exposing the target organ. With these 2 sutures, three trocars were sufficient for the procedure. For D-J stenting, as one 3-mm trocar was occupied by the stent, only one port was left for maneuvers. In case an F3 was necessary, it could be difficult to insert the D-J stent into the ureter. Recently, we treated a patient (not included in reported series) who had to have the D-J stent placed by retrograde fashion using a cystoscope. However, in the current series, all D-J stents were placed successfully.
Due to the parallel vision and the clashing of instruments, the anastomosis is the most difficult part of LESS. From our experience, starting the anastomosis from the side facing the camera (the posterior side) is easiest. As the posterior is facing the camera, a better view is possible, providing a direct approach to the tissue. After the completion of the posterior side, the second traction suture is made to pull up the anterior side of the pelvis higher than the line of the finished posterior anastomosis. Subsequently, the edges of the posterior side are closed.
In our group of patients, the draining tubes come out through the umbilical incision. As the drainage could be inefficient this way, postoperative temperature was analyzed to assess any possible extravasations, as urine extravasations will usually cause very high temperature. Indeed, among patients with fever, drainage was minimal while no urinary tract infection was present, thereby suggesting urine extravasations. Extravasations were not significant in our series as most patients did not have high fever. Additionally, postoperative infection was uncommon in our group of patients as urine examinations were performed regularly. Routine intravenous antibiotics were administered to all patients, but were continued until a normal temperature is resumed among patients with postoperative fevers. From our experience, mild degree of extravasation will not cause major problems. Ultrasound was performed at the readmission for D-J removal and no abnormality was detected in any of the patients. However, whether the occurrence of postoperative fever will have any effect on postoperative ileus requires further follow-up.
In our previous experience of retroperitoneal laparoscopic pyeloplasty, we encountered patients (mostly infants) whose drainage volume increased significantly after the urethral catheter was removed on postoperative day 3, but was quickly reduced after the reinstallation of a urethral catheter. Thus, in the current series, we preferred to be cautious and kept the draining tube and urethral catheter in place for a relatively long period postoperatively. Usually the urethral catheter will be kept in place until the drainage falls below 10 mL or body temperature becomes normal for patients with fever. For patients with no fever and minimum drainage, the urethral catheter was kept at least for 4 days postoperatively. The draining tube was removed the next morning after the removal of urethral catheter.
Postoperative recovery was uneventful in all of our cases. The immediate results were comparative to other minimally invasive modalities. The cosmesis results are even more impressive. The scar of the incision is concealed within the umbilicus, and the operation is effectively scarless (Fig. 3). Only one patient, a 13-month-old boy, developed symptoms of stenosis. In this case, renal stoma was performed by open surgery immediately after the removal of D-J, and a second open pyeloplasty was performed half a year later. The patient has since made a full recovery.

Appearance of the umbilical incision at the time when D-J was removed cystoscopically.
While complex operations of LESS have been well reported in the literature in adults, there are few such reports in children. From our experience, LESS in children is feasible and could have its own advantage compared to the adult. With a smaller abdominal cavity and the attachments of the target organ being not as tough, it would be easier to reach and maneuver the target organ. Also, smaller-sized conventional instruments are more applicable in children, which could provide even better maneuverability. Experience in conventional laparoscopy is critical for the success in LESS. We started our traditional laparoscopic pyeloplasty in a step-by-step process. Initially we did 20 cases of assisted retroperitoneal pyeloplasty. At that stage, the dissections were completed by laparoscopy and the pelvis was pulled out for an extracorporeal anastomosis. Subsequently, we completed more than 100 cases of retroperitoneal pyeloplasty and have now switched all our pyeloplasty to LESS procedures. It is our impression that the operative time is slightly shorter in retroperitoneal route. Although previously reported in the literature, possibly due to the younger age range of our patients, we did not encounter crossing vessels in our series. Relief of symptoms was regarded as the most important criteria of success. Isotope renograph follow-up was also recommended for all of our patients. Symptoms of anastomosis obstruction (e.g., pain and vomiting) and deterioration of split renal function in isotope were the criteria for reoperation.
Our initial data suggested that pediatric pyeloplasty in LESS is technically feasible. The procedures could be completed successfully within a reasonable time, and the immediate results are quite good. However, further experience and longer follow-up are necessary to appropriately evaluate the benefits and limitations of this technique in children.
Footnotes
Disclosure Statement
No competing financial interests exist.