
Abstract
Abstract
Aim:
The consequences of bariatric surgery on important metabolic and signaling pathways are still poorly understood. The aim of our study was to unravel the network of metabolic changes and obesity-related protein biomarkers in morbidly obese children and adolescents undergoing laparoscopic sleeve gastrectomy (LSG).
Methods:
In a prospective study, 6 children with morbid obesity who had failed a well-established conservative weight loss therapy underwent LSG. Pre- and 6 months postoperatively, a metabonomic profiling of 163 metabolites by mass spectrometry and protein profiling by ELISA (clusterin [CLU], pigment epithelium-derived factor [PEDF], retinol binding protein 4 [RBP4], paraoxonase 1 [PON1]) was performed to identify biomarkers of important pathways.
Results:
At referral for surgery, the mean age was 14.5 years (range 8–17), mean body mass index (BMI in kg/m2) was 48.13 (range 41.1–56.3). All patients showed various metabolic comorbidities. LSG was uneventful in all of them. At 6 months postsurgery, the mean BMI has dropped to 37.1 (range 28.4–40.6). Targeted serum metabonomics resulted in 7 metabolites, which were significantly affected by LSG. Among those, the amino acid phenylalanine was increased, and methionine decreased. The glycero-phospatidylcholine PCaaC38:5 were upregulated, and PCaaC40:2 and PCaaC42:1 were down regulated after 6 months compared with baseline. Further, sphingomyoline (SM) C26:0 and SM C26:1 were decreased after 6 months. The obesity-related biomarkers CLU, PEDF, and RBP4 were decreased, whereas PON1 levels were increased.
Conclusion:
LSG leads to changes in amino acids and in lipid metabolism indicated by glycerol-phosphatidylcholines and SM. The pattern of protein biomarkers and metabolites might provide measures for the induced physiological changes and for therapy monitoring.
Introduction
Since laparoscopic sleeve gastrectomy (LSG) can be seen as a drastic restriction of nutrition, the most obvious changes are expected to happen in the metabonome. Therefore, metabolite screenings are the method of choice for unraveling changes in the metabonome. 19 Especially the metabolites covering the central pathways of metabolism of amino acids, glycolysis, and fatty acids are suspected of being indicative for principal physiological changes. With the advent of high throughput methods based on mass spectrometry, it became possible to assess up to hundreds of metabolites in parallel. 3
Changes in the physiology are also supposed to affect protein biomarkers that are known to be associated with obesity. 36 In an earlier global serum proteomics approach, several markers were identified to be correlated with the loss of fat mass in adult patients who had undergone LSG. 23 Among them were the adipokines pigment epithelium-derived factor (PEDF) and retinol binding protein 4 (RBP4), as well as the lipoprotein clusterin (CLU) and the antithrombiotic protein paraoxonase (PON). 5
PEDF was found to be secreted by adipose tissue and is thought to cause insulin resistance. 22 Increased PEDF levels are correlating with metabolic syndrome, type 2 diabetes, and abdominal fat distribution.20,21,31
RBP4 was initially described to be associated with the metabolic syndrome. 9 It is well known that RBP4 is predominately produced and secreted from the adipose tissue. 17
CLU, also known as apolipoprotein ApoJ, was found to be present in high-density lipoproteins (HDL) and very high-density lipoproteins (VHDL). 30 In these complexes, the antithrombotic 14 and anti-inflammatory 18 protein PON1 is also found. For PON1, a reduction in patients with diabetes is reported. 5
The value of the circulating biomarkers for the assessment of physiological changes induced by LSG has so far been only partially analyzed for adults, and so, a thorough evaluation of these parameters for children and adolescent patients is mandatory. Since both metabolites and proteins are easy to measure in serum samples, they can putatively serve as markers in clinical diagnostics as well as for therapy monitoring.
Materials and Methods
We selected 6 patients (age 8–17) for whom every conservative treatment had failed and who had been identified for bariatric surgery according to present guidelines. 12 Assent and written informed consent were obtained from all subjects and/or from a legal representative before initiation of any study-related activities. The study was performed in accordance with the principles of Good Clinical Practice 13 and the Declaration of Helsinki. 1
An extensive preoperative work-up was performed including ECG, Chest X-ray, laboratory parameters (including blood count, electrolytes, metabolic parameters, thyroid function tests, clotting studies, and arterial blood gas), lung function tests, sleep study, upper GI contrast study, and abdominal ultrasound. Height was measured to the nearest 0.5 cm, and weight to the nearest 100 g by using a digital balance (BF 18; Beurer). Body mass index (BMI) of the children was calculated as weight (kilograms)/height (meters). 2 BMI SD scores (SDS: individual BMI value reference mean BMI value divided by SD to scale the data for comparison across ages and sex) were calculated and used in the analysis. All suffered from comorbidities as features of a developing metabolic-vascular syndrome such as dislipidemia, cholecystolithiasis, and arterial hypertension. 33 Moreover, in an 8-year-old girl, Prader-Willi-Syndrome had been genetically confirmed at the age of 2. The decision for bariatric surgery was unanimously taken by the patient, parents, and the obesity team. Anthropometric and metabolic data of all patients are presented in Table 1.
The 2-hour postprandial plasma glucose was measured by oGTT. Data were shown as mean±SD measured at baseline and 6 months after LSG. Significant changes are determined by dependent Student's t-test (P<.05).
γ-GT, γ-glutamyltransferase; ALAT, alanin-aminotransferase; BMI, body mass index; HDL, high-density lipoproteins; LDL, low-density lipoprotein; LSG, laparoscopic sleeve gastrectomy; SDS, SD score.
Sample collection
Twelve milliliters of blood, 2 mL into EDTA-containing tubes, was taken by venipuncture. All blood samples were collected between 8:00 and 10:00 a.m. after an overnight fast. The OGTT was performed after an overnight fast with 75 g standardized glucose solution (Glucodex Solution 75 g; Merieux). Venous blood samples were taken at 0, 60, and 120 minutes for measurements of plasma glucose concentrations. Fasting plasma insulin was measured with an enzyme immunometric assay for the IMMULITE-automated analyzer (Diagnostic Products Corporation). Serum high-sensitive CRP was measured by immunonephelometry (Dade-Behring). Serum total-, HDL-cholesterol, and triglycerides were measured as previously described. 17
Quantitative ELISA assays were performed for evaluation of detected proteins by mass spectrometry; proteome validation studies were performed by using the following immunoassays: Quantikine human RBP4 immunoassay (R&D Systems), human PEDF ELISA (BioVendor), human CLU ELISA (BioVendor), and human PON1 (Uscn Life Science, Inc.). All immunoassays were performed according to the manufacturer's recommendations.
Metabonome analysis
The metabonome analysis was performed by using the AbsoluteID.kit (Biocrates Life Science AG) according to the recommendations of the suppliers and as described in Enot et al. 7 by using an API 4000 (ABI Sciex).
Statistical analysis
Quantitative variables are expressed as mean±SD throughout the article unless otherwise stated. Comparisons between time points with regard to all quantitative endpoints were performed by two-tailed Student's paired t test. The significance level was set at P<.05. GraphPad Prism (GraphPad Software, Inc.) was used for all analyses and created figures.
Results
Anthropometric and metabolic data of the children, by weight classification, are shown in Table 1. At referral for surgery, the mean age was 14.5 years (range 8–17), mean BMI (in kg/m2) was 48.4 (range 40.6–56.3), and all patients depicted major co morbidities, including arterial hypertension, impaired glucose tolerance, elevated liver enzymes and steatosis hepatis, sleep apnea syndrome, cholelithiasis, and dyslipidemia. LSG was uneventful in all of them. At 6 months postsurgery, the mean BMI dropped to 37.1 (range 28.4–40.6). BMI-SDS, 2 hours postprandial Glucose, HDL-cholesterol, and the liver enzymes alanin-aminotransferase (ALAT), ASAT, and γ-glutamyltransferase (γ-GT) were significantly changed, and systolic blood pressure had dropped significantly into the age- and gender-specific normal range after LSG after 6 months (Table 1). Triglycerides decreased in trend 6 months after LSG (1.34±0.26 versus 0.89±0.33, P=.053) However, BMI, fasting plasma glucose, total cholesterol, and low-density lipoprotein-cholesterol did not show a statistically relevant change after bariatric surgery (Table 1).
MS/MS based quantitative profiling yielded significant changes of amino acids, glycerophospholipids, and sphingomyolines (SM) after 6 months as a consequence of LSG. Among those, the amino acid phenylalanine was increased, and methionine decreased (Fig. 1A, B). Further, SM C26:0 and SM C26:1 were decreased after 6 months (Fig. 1C, D). The glycero-phospatidylcholine PCaaC38:5 was upregulated (Fig. 1E), and PCaaC40:2 and PCaaC42:1 were down regulated after 6 months compared with baseline (Fig. 1F, D).

Significantly regulated serum metabolites 6 months after laparoscopic sleeve gastrectomy (LSG). The results were taken from metabolite quantification by qTRAP-MS analysis. Data are presented as mean±SD measured at baseline (white bars) and 6 months after surgery (black bars). Significant changes are indicated by asterisks (time effect determined by dependent Student's t-test).
With regard to proteins, PEDF, RBP4, and CLU were upregulated (Fig. 2A–C), whereas the concentration of PON1 was significantly reduced (Fig. 2D).
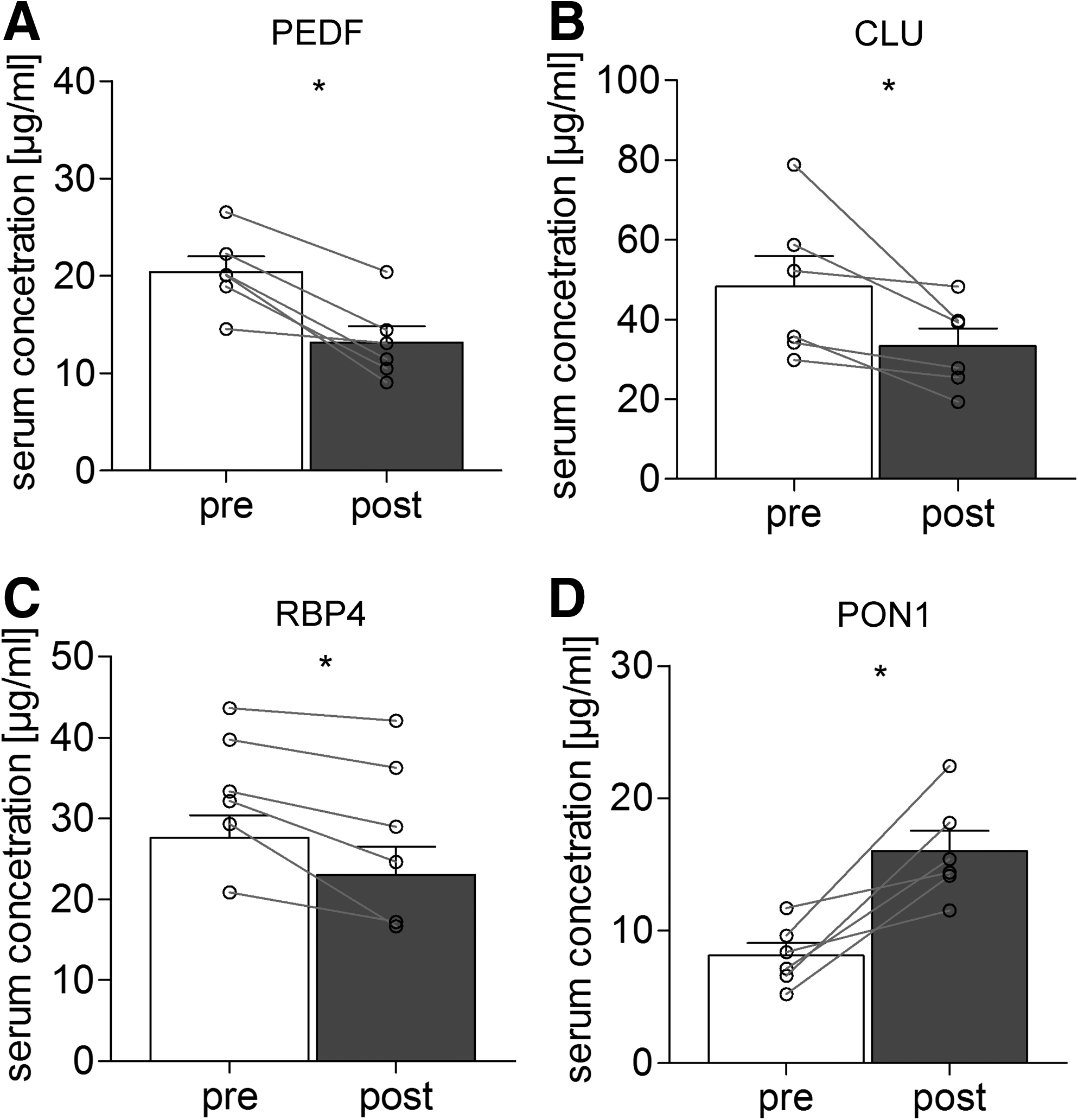
Significantly regulated serum protein abundance 6 months after LSG. Data are depicted as mean±SD measured at baseline (white bars) and 6 months after surgery (black bars). Significant changes are indicated by asterisks (time effect determined by dependent Student's t-test).
Discussion
Despite all the observations about the long-term effect of bariatric surgery, the understanding of the underlying mechanisms leading to such tremendous weight loss is poor. To predict the outcome, it is necessary to decipher the specific changes of the metabolism imposed by LSG. Therefore, it is mandatory to identify profiles from which biomarkers can be selected that can be used in clinical diagnostics to monitor the glucose and lipid metabolism. This applies especially to children and adolescents, because they have a longer life expectancy and a higher risk of suffering from long-term consequences.
In the current study, children and adolescents with obesity and metabolic syndrome were treated by LSG. Initially, the LSG had been established as a first-line operation for super obese adults to achieve an initial weight loss until they could be safely treated by a malabsorptive procedure such as the Roux-en-Y gastric bypass. 26 Recently, the LSG has gained increasing popularity even as a stand-alone technique, because the overall weight loss was sufficient in some patients. 34 Moreover, it could be demonstrated that LSG, which is technically considered a restrictive operation only, caused the resolution of metabolic comorbidities by itself.
The identified changes in the metabonome profile indicate effects on the metabolism of amino acids, SM, and glycero-phosphatidylcholines (PC). Human obesity is associated with increased serum phenylalanine concentration. However, this is probably caused by liver dysfunction related to liver steatosis, 32 which occurs more frequently in morbid obesity. Interestingly, our study yielded a decreased serum phenylalanine concentration after bariatric surgery after 6 months. Recently, other authors showed a strong positive correlation between serum phenylalanine and serum alanine transaminase concentrations. 32 This is in line with the observed lowering liver enzyme concentration and the significant correlation of phenylalanine and ALAT (data not shown) in our current study. Taken together, serum concentration of phenylalanine seems to be a valid biomarker of liver dysfunction associated with liver steatosis. 32 In our current study, the amino acid methionine was significantly increased after bariatric surgery. It was demonstrated that multiple metabolic abnormalities of methionine kinetics are present in type 2 diabetes with nephropathy and so it supports the finding of the altered levels of phenylalanine, which also points to pathologic changes in the liver. 24
PC are described to be crucially involved in lipid metabolism and lipid transport. They have been found to be associated with the accumulation of fat in the liver. 16 Besides their primary relevance for lipid metabolism, it is also reported that they are capable of alleviating inflammatory processes. 10
The decrease of two species of SM corresponds well with their reported higher levels in case of arteriosclerosis and other diseases. 29 Here, the loss of weight seems to have already caused decreased levels in serum. This has the potential of reducing the risk for coronary artery disease and related comorbidity.15,25
The decrease of the adipokines PEDF and RBP4 can be viewed as a consequence of the loss of body fat, as they are reported to be produced mostly by adipose tissue and the liver.27,35 Both factors are also described as being related to insulin sensitivity and disturbed glucose metabolism. Although it is unknown whether they are causative or resulting factors, the current results suggest that they can be used as markers to follow the success of LSG.
Both CLU and PON1 are associated with cholesterol metabolism and HDL and VHDL particle composition. 30 The decrease in CLU can be interpreted as coincidental to the increase of HDL metabolism. The dramatic restriction caused by LSG leads to a maximal metabolic turnover that is accompanied by a relative increase in oxidative stress. 4 To counteract this, the increase of antioxidant capacity might explain the increase of PON1.
Conclusion
The data show that LSG affects the amino acid and lipid metabolism. Our data suggest, in fact, that proteomic and metabolomic profiling is feasible and may yield information which will better enable investigators to phenotype cases and responses to surgery much more precisely than has been done in the past.
Footnotes
Acknowledgments
This work was supported by the Federal Ministry of Education and Research (BMBF), Germany (Integrated Research and Treatment Center IFB “Adiposity Diseases,” FKZ: 01E01001). The authors are grateful to David Petroff for looking over the manuscript. They would also like to express their gratitude to all children and their parents who participated in this project.
Disclosure Statement
No competing financial interests exist.