
Abstract
Abstract
Endoscopic fetal surgery is most commonly used for the treatment of twin-to-twin transfusion syndrome (TTTS), but the surgical techniques can be applied to other forms of fetal surgery. We present our experience with endoscopic fetal surgery over the past 10 years. From 2000 to 2010, 70 endoscopic laser ablations of placental vessels for TTTS were performed. Median number of placental vessels ablated was four. The incidence of preterm rupture of membranes (PROM) was 6%. Overall survival was 70%, with at least one twin surviving in 82%. Tocolysis was used in 73% of patients for a median of 12 hours. The combination of an open surgical approach, Seldinger technique, and uterine plugging led to outcomes similar to other reports, with a significantly lower PROM rate. Although TTTS is the most common application of endoscopic fetal surgery, this approach is applicable for other indications. Insertion and removal of tracheal occlusion balloons for severe congenital diaphragmatic hernia are currently being performed at our institution.
Introduction
With all of these restrictions, only a handful of indications for fetal surgery could be justified, among them bilateral lower urinary tract obstruction, congenital diaphragmatic hernia (CDH), and a few rare disorders, such as large cystic lung masses and sacrococcygeal teratomas. Whereas animal studies had established the feasibility of open fetal surgery and its ability to halt or correct the disease process, clinical application proved to be more difficult. Complications of open fetal surgery (direct access to the fetus via a generous maternal laparotomy and hysterotomy) included significant morbidity for the mother and high fetal morbidity and mortality. 11 In addition, the natural history of the diseases was poorly understood, leading to needless surgery in some and futile attempts in others.12,13 Most importantly, the advances in postnatal care of some of these conditions far outpaced the modest improvements in prenatal intervention. CDH, for example, was associated with a 70% mortality in the early 1980s. By the time open fetal surgery for CDH could achieve double-digit survival, the overall survival after postnatal therapy was increasing rapidly, to more than 70% today. 14
Today, endoscopic fetal surgery is most commonly used for the treatment of twin-to-twin transfusion syndrome (TTTS). 15 TTTS occurs in 1 of 6,000 pregnancies and causes fetal demise in 10% to 15%. It occurs only in monochorionic gestations, and is caused by unbalanced blood flow from one twin to the other through placental vascular communications. Left untreated, oligohydramnios, intrauterine growth restriction, and, ultimately, cardiac failure develop in the donor. The recipient experiences polyhydramnios and is at risk for high-output heart failure and hydrops. Either twin may die, placing the surviving twin at risk for severe brain or heart anomaly and death.16,17
If diagnosed before 24 weeks of gestation, the untreated syndrome often leads to dual fetal demise.
Endoscopic laser ablation is the treatment of choice for severe TTTS. By Quintero's classification, 18 patients with stage 1 TTTS (polyhydramnios in recipient, oligohydramnios in donor, and donor bladder still visible) are not offered surgical intervention at most centers because noninvasive treatment is equally successful. Surgical intervention is typically reserved for fetuses with evidence of stage 2 (same as stage 1, but donor bladder is not visible), stage 3 (abnormal Doppler signals suggestive of hemodynamic stress), or stage 4 (evidence of hydrops).
A second application of endoscopic fetal surgery is fetal tracheal occlusion for very severe CDH. Physiologic justification, indications, and patient selection are beyond the scope of this report and are published elsewhere.19,20
Surgical Technique
Consultation for TTTS includes a detailed anatomic ultrasonography of both fetuses, evaluation of placental location and cord insertions, and fetal echocardiography. Endoscopic laser ablation is offered for those pregnancies demonstrating persistent stage II, stage III, or stage IV disease.
Endoscopic laser ablation can be performed under general or regional anesthesia (spinal/epidural). Access to the uterine cavity can be through a large laparotomy (previously advocated by some for anterior placentas), mini-laparotomy (similar to an “open” laparoscopy approach), or percutaneously. While percutaneous endoscopy is used by most, we have been concerned that a cannula that is simultaneously anchored in the abdominal wall and the uterus creates a fulcrum that can cause shearing forces on the uterus. This in turn increases the risk of premature rupture of the membranes (PROM) and preterm labor. We therefore prefer direct observation of the anterior wall of the uterus, which also eliminates any shearing injury to the myometrium. We perform all procedures under general anesthesia. A mini-laparotomy incision (1–2 cm) is created. The subcutaneous tissues, fascia, and muscle layers are divided to enter the peritoneal cavity. Once the uterine surface is exposed, the recipient sac is accessed via Seldinger technique. A 12-F peel-away introducer is used as a cannula to accommodate a custom-curved 10F sheath containing a 2.0 mm semirigid fiber endoscope (Fig. 1). Concomitant endoscopy and ultrasonography is used to map the umbilical cord insertions and the plane between each twin's vascular territory. This avascular plane is carefully scanned and unpaired crossing vessels are evaluated for laser occlusion. Laser ablation is performed using a diode laser (wavelength 810 nm) at 5–15 W through a 550 μm fiber and nontouch mode, delivering a repeated pulse (0.1 second frequency) until the cessation of flow or a complete blanching and buckling of the vessel is noted. Once all identified unpaired vessels have been ablated, the cannula is removed while a gelatin sponge plug is placed to seal membranes and myometrium. 21
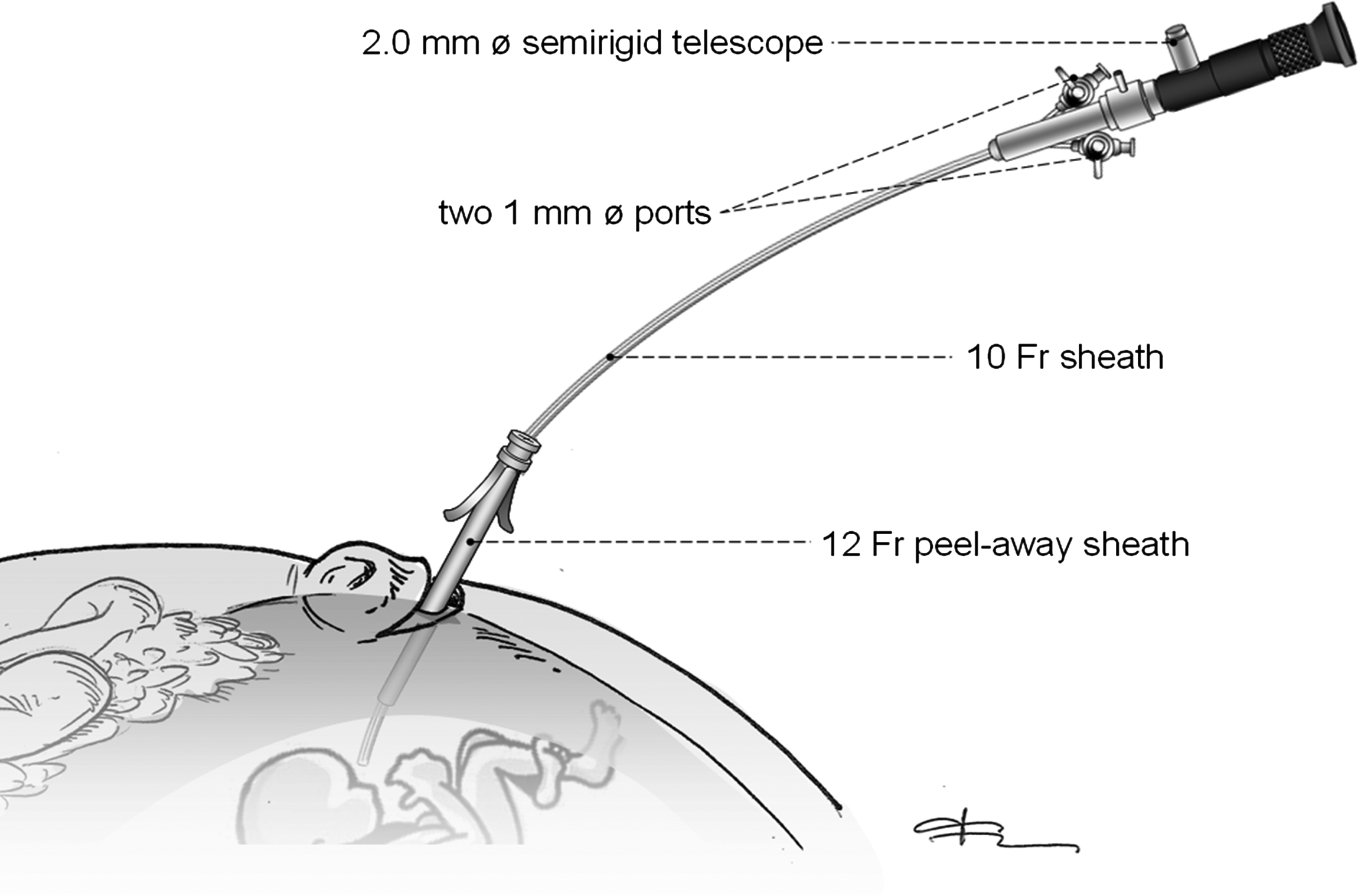
Schematic setup of endoscopic fetal surgery. A 10F sheath containing a 2.0 telescope and two additional working ports is inserted via an open approach into the gravid uterus through a 12F peel-away sheath, acting as an endoscopic cannula.
Postoperatively, patients are monitored for uterine contractions and treated with calcium channel blockers or magnesium sulfate tocolysis as needed for the first 24 hours. Follow-up ultrasonography examinations are performed daily and patients generally return home on postoperative day 2, with twice-weekly ultrasonography examinations for the first 2 weeks, and every 1–2 weeks thereafter to monitor fetal well-being and the effectiveness of the endoscopic intervention.
For the treatment of severe CDH, the same approach is used. Access to the uterine cavity is performed with the same technique as outlined above, and the same telescope and sheath are used. The fetal mouth is identified and the fetus is intubated with the 10F sheath, under direct endoscopic vision and ultrasonography control. A detachable balloon is deployed in the upper trachea (Investigational Device Exemption No. G080077, Food and Drug Administration 22 ). The device remains in the fetal trachea for 4–6 weeks and is retrieved endoscopically using the same surgical approach.
Results
From 2000 to 2010, 70 endoscopic laser ablations of placental vessels for TTTS were performed. Intervention was performed in 16% for stage 2 TTTS, in 65% for stage 3, and in 19% for stage 4. Median number of placental vessels ablated was four. Median operative time was 60 minutes (range 20–135 minutes). Mean gestational age at operation was 21.0 weeks, and mean gestational age at delivery was 32.1 weeks. Tocolysis was used in 73% of patients for a median of 12 hours. The duration of hospitalization was 2.4±0.8 days.
Overall survival was 70%, with at least one twin surviving in 82%. Both twins survived in 59%. PROM within 28 days of surgery occurred in 3.2%; the overall preterm PROM rate was 6.3%.
Discussion
We demonstrate successful utilization of endoscopic laser ablation of placental vessels for TTTS over 10 years. The combination of an open surgical approach, Seldinger technique, and uterine plugging led to outcomes similar to other reports, with a significantly lower PROM rate. 23 The decade-long experience with endoscopic fetal surgery has allowed us to move beyond the learning curve and to establish clear technical and programmatic guidelines for a safe and successful fetal surgery program. The endoscopic approach to the gravid uterus and the fetus can be applied to other indications, both current and future. Insertion and removal of tracheal occlusion balloons for severe CDH is currently being performed at our institution, under a Food and Drug Administration–sanctioned protocol. 22 The instruments and approach for this indication are identical to that for laser ablation in severe TTTS. Future applications of endoscopic surgery await improvements in diagnostic accuracy, the ability to establish clear differential diagnoses and stratify risks, and technical advances in minimally invasive technology. Recently, the MOMS showed that prenatal intervention for spina bifida may decrease the need for ventriculoperitoneal shunting of hydrocephalus, decrease the incidence of hindbrain herniation, and improve independent ambulation at 30 months, compared to traditional postnatal repair. 8 While prenatal repair was performed through open fetal surgical techniques and generous maternal laparotomy, some have attempted to perform the procedure through minimally invasive techniques.24,25 As was clear in these, and other initial attempts,11,25 the use of multiple ports greatly increases the complication rate of endoscopic fetal surgery, to levels comparable with open fetal surgery. In the future, the combination of microsurgical techniques, waterproof adhesive materials, and miniaturized endoscopic instruments may allow prenatal treatment of spina bifida through minimally invasive techniques. 26 In conclusion, honing one's endoscopic fetal surgery skills through the treatment of severe TTTS may pave the way for other applications of prenatal intervention.
Footnotes
Disclosure Statement
No competing financial interests exist.