
Abstract
Abstract
Background:
Single-incision laparoscopic surgery (SILS) is increasingly being used to treat acute appendicitis. Existing SILS techniques suffer from inefficient triangulation and poor ergonomics. In an effort to improve on existing SILS techniques, we developed the magnet-assisted single trocar (MAST) appendectomy.
Subjects and Methods:
We retrospectively analyzed all MAST appendectomies performed between March 2010 and February 2011. Outcomes included demographics, diagnosis, operative time, hospital stay, and complications.
Results:
Twenty-three MAST appendectomies were performed in 10 boys and 13 girls. The mean age at operation was 12.22 years (range, 5–19 years), and the mean weight was 46.5 kg (range, 25–82 kg). At presentation the mean white blood cell count was 15,000 with 74% polymorphonuclear neutrophils. The mean operative time was 61 minutes (range, 20–105 minutes), and length of stay was 3.6 days (range, 1–7 days). In total, 4 operations (17%) required one additional 5-mm trocar to complete the operation, and none was converted to an open operation. There were no intraoperative complications, nor were there any wound infections.
Conclusions:
MAST appendectomy is safe and effective in children. Magnetic instruments provide excellent triangulation and improve ergonomics. This technique uses a single 12-mm trocar and can be performed without the aid of a surgical assistant.
Introduction
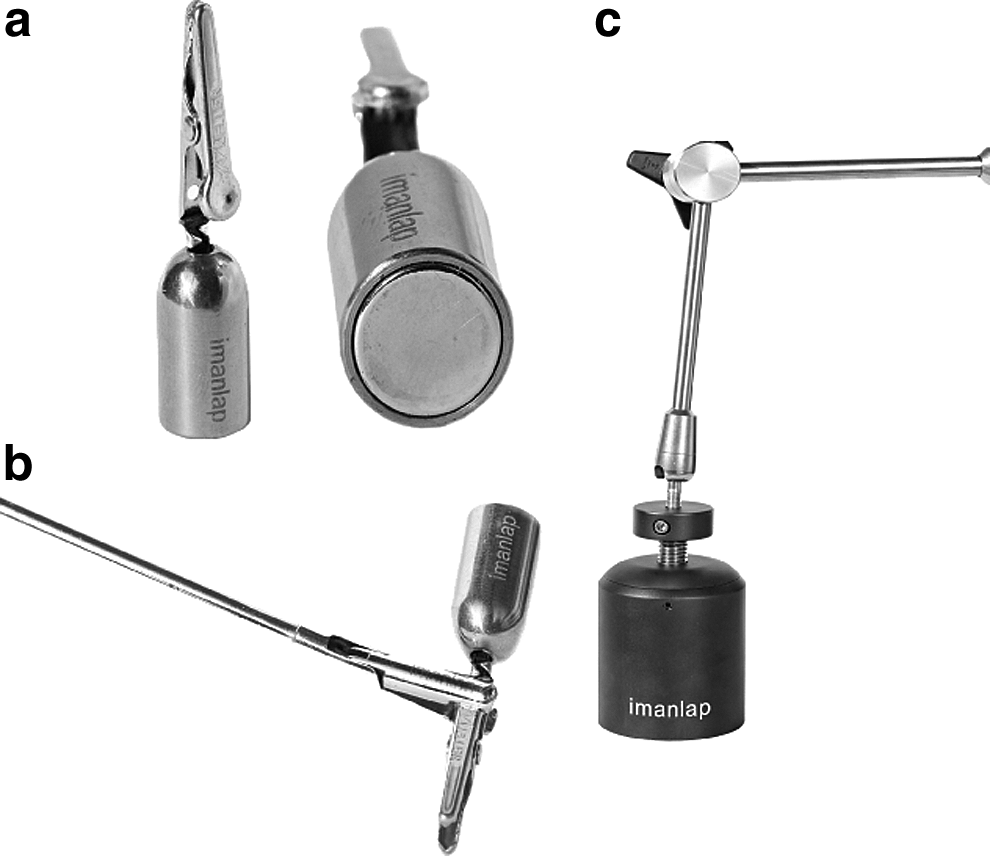
In an effort to improve on existing SILS techniques, the magnet-assisted single trocar (MAST) technique was developed. MAST surgery uses specialized magnetic graspers (Dominguez Magnetic Grasper® [DMG], Imanalap, Buenos Aires, Argentina) that are controlled by an externally coupled handheld magnet (Fig. 1). The magnetic graspers provide dynamic exposure by simply repositioning the external magnet while reducing the number of instruments entering the umbilical incision. The feasibility and safety of the MAST technique have been demonstrated in a variety of operations in adults.3,4 Here we describe our initial experience with MAST appendectomy in 23 pediatric patients.
Subjects and Methods
We conducted a retrospective review of all patients undergoing MAST appendectomy between March 2010 and February 2011. The diagnosis of acute appendicitis was made based on history and physical examination, and preoperative imaging was left to the discretion of the operating surgeon. In general, patients with prior abdominal operations or hemodynamic instability were not considered candidates for the MAST technique. Charts were reviewed for presenting history, patient demographics, intraoperative diagnosis, operative time, operative conversions, length of hospital stay, complications, and patient follow-up. Additionally, we reviewed the operative time of the last 23 consecutive conventional (three-trocar) laparoscopic appendectomies performed at our institution as a point of reference for comparison. Statistical analysis was performed with the Mann–Whitney test using GraphPad Prism.
Operative technique
One of the authors (G.D.) was present at all the operations to proctor the operating surgeon. With the patient under general anesthesia, a 12-mm trocar was inserted at the umbilical base using the Hassan technique, and the peritoneal cavity was insufflated to 10 mm Hg with CO2. An 11-mm, 0° laparoscope with a 27-cm-long, 6-mm working channel (Storz, Tuttlingen, Germany) was used. A spring-loaded alligator grasper attached to an 11-mm neodymium magnet (DMG) was introduced through the umbilical trocar. A powerful external magnet (Imanlap) controls the DMG by magnetic forces transmitted across the abdominal wall (Fig. 2). Next, a Thomas forceps introduced through the scope's working channel was used to open and close the jaws of the DMG. The DMG grasped the appendix and provided dynamic traction by repositioning the external magnet on the abdominal wall (Fig. 3). Varying the distance between the external magnet and the abdominal wall regulated the amount of force that was transmitted to the DMG. Once adequate exposure was obtained, the external magnet was fixed in place with a self-retaining retractor. The mesoappendix was transected using either monopolar electrocautery or a 5-mm LigaSure® (Covidien, Mansfield, MA). Next, the appendiceal base was doubly ligated with 3-0 chromic sutures or 5-mm Hem-o-lok® clips (Teleflex Medical, Research Triangle Park, NC). The appendix was transected and removed through the umbilical trocar. Lastly, the fascia and skin were closed in layers.

The operative laparoscope is introduced through a 12-mm trocar. With the external magnet mounted on a self-retaining retractor, the surgeon drives the camera and operates without an assistant.
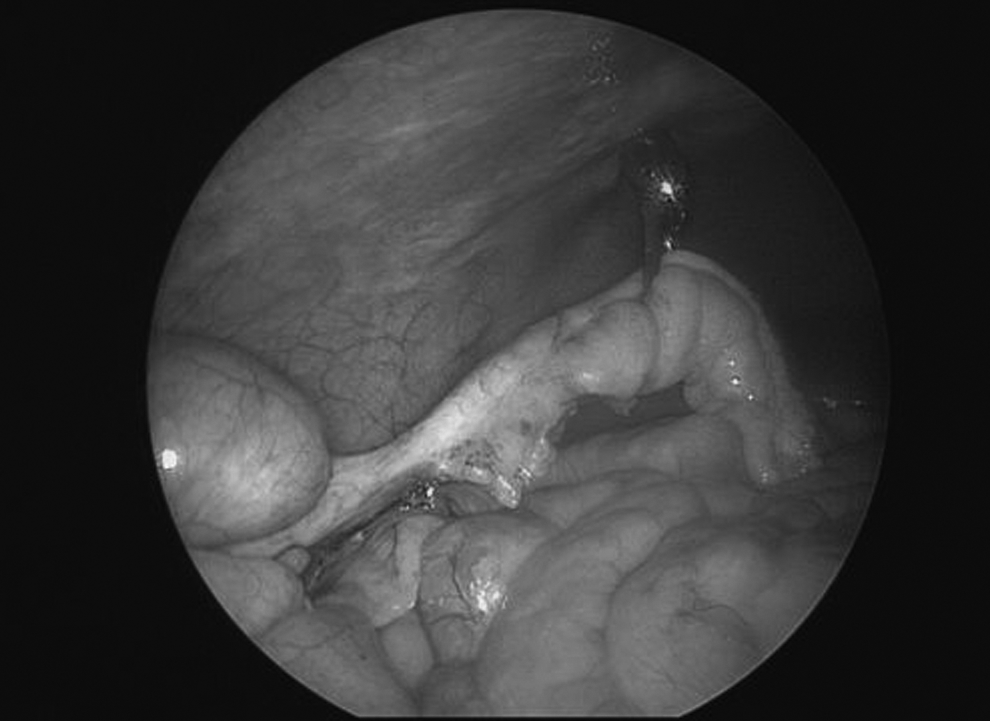
The Dominguez Magnetic Grasper grabs the appendix and provides dynamic traction by repositioning the external magnet.
Oral intake was resumed ad libitum, and early ambulation was encouraged. Requirements for discharge from the hospital were as follows: afebrile for 24 hours, eating a regular diet, and adequate pain control with oral analgesics. The wound was inspected every day during the hospital stay and on postoperative Day 7 at the outpatient clinic.
Results
In total, 23 patients (10 boys and 13 girls) underwent MAST appendectomy during the 11-month study period (Table 1). The mean age at operation was 12.2 years, with ages ranging from 5 to 19 years. The mean weight was 46.5 kg (range, 25–82 kg). At presentation, the mean white blood cell count was 15,000 with 74% polymorphonuclear neutrophils. The mean operative time for MAST appendectomy was 61±19 minutes, compared with that for conventional laparoscopic appendectomy of 39±26 minutes (P=.01). The mean length of stay for MAST appendectomy was 3.6 days (range, 1–7 days). The appendix was perforated in 4 patients (17%), gangrenous in 4 (17%), and retrocecal in 3 (13%). A total of 4 operations required an additional 5-mm trocar to complete the operation, and none was converted to the open approach. In three instances the 5-mm trocar was placed in the suprapubic position, whereas in one the umbilical skin incision was enlarged, and the 5-mm instrument was inserted without a trocar alongside the primary 12-mm trocar. Two operations were converted because the appendix was gangrenous and perforated, 1 because the appendix was in a retrocecal location, and 1 because the appendix was long and tortuous. There were no intraoperative complications, and no child had a postoperative wound infection.
Discussion
Laparoscopic surgery has become the gold standard for many operations due to faster recovery, less pain, and better cosmetic results compared with open surgery. 5 Several new techniques have emerged that minimize the number and size of the abdominal incisions, including natural orifice transluminal endoscopic surgery (NOTES) and SILS. Although NOTES initially received a great deal attention, surgeons have been slow to adopt this technique because it requires visceral injury to access the peritoneal cavity, and public demand has been limited. On the other hand, SILS is gaining in popularity perhaps because it is a stepwise progression from existing laparoscopic techniques. However, existing SILS techniques suffer from inadequate triangulation and poor ergonomics.1,2
Our report demonstrates the safety and efficacy of MAST appendectomy in the pediatric population. There are two fundamental components of the MAST technique: the magnetic retraction system and the operative laparoscope. The DMG uses magnetic force to provide dynamic traction at the point of dissection and removes the retracting instrument from the umbilical wound, thus reducing instrument crowding. Because the DMG is not fixed at the level of the fascia, it is free to cruise around the abdomen and eliminates the need for additional trocars. Unlike other magnetic retraction systems that are under investigation, the DMG easily releases and grasps tissue at a different location, thus increasing its utility.6,7 The other component of the MAST technique is the operative laparoscope, which functionally combines the dissecting instrument and laparoscope into a single instrument. Thus the instrument and laparoscope are fixed in the same axis, and the visual field is always directed at the point of dissection. This configuration allows the surgeon to drive the camera and operate simultaneously without the need for a surgical assistant, all through a single 12-mm trocar. Furthermore, the MAST technique eliminates hand crossing, instrument collision, and the need for reticulating instruments.
Our results using the MAST technique compare very favorably with those recently reported by Hansen et al. 1 using the SILS technique. In their series of 120 appendectomies in pediatric patients, 15% required at least one additional trocar, and 9% required two or more trocars. Although our series is considerably smaller, a single additional trocar was required in 17% of cases. Most of the cases requiring an additional trocar were for perforated appendicitis or a rectrocecal appendix. However, perforated and retrocecal appendicitis cases do not preclude MAST appendectomy, as less than half (3 of 7) such cases required an additional trocar. While Hansen et al. 1 reported a median operating time of 37 minutes, the operative time for MAST appendectomy is comparable to other early experiences of SILS appendectomy. Oltmann et al. 8 recently published a series of 19 SILS appendectomies in pediatric patients in which the mean operating time was 58 minutes. The significantly longer operative time for the MAST technique compared with conventional laparoscopy is expected and is likely due to the learning curve of the operating surgeons and operating room staff. This is reflected in the wide variation in operating times (20–105 minutes) for MAST appendectomy.
Koontz et al. 9 previously reported the use of the operative laparoscope in 111 pediatric appendectomies. However, their technique used the operative laparoscope to exteriorize the appendix at the umbilicus and perform the appendectomy extracorporeally. Superficial wound infections occurred in 6% of cases. Chandler and Danielson 10 reported a superficial wound infection rate of 10% in their series of SILS appendectomies using a technique that required a fascial incision large enough to accommodate two 5-mm and one 12-mm trocars. Our series compares very favorably to these studies, as we saw no superficial wound infections. The lower incidence of wound infections is likely due to transection of the appendix intra-abdominally, extraction of the appendix through the 12-mm trocar, and minimal manipulation of the umbilical wound.
A drawback of the MAST technique is that it requires specialized magnetic instruments and a dedicated operative laparoscope. We used an operative laparoscope with a 27-cm-long working channel. Because of the long working length, we used 42-cm-long, 5-mm laparoscopic instruments. Additionally, the Thomas forceps and Hem-o-lok clip applier we lengthened to allow for adequate reach through the scope. Others have reported the use of an operative laparoscope with a 20-cm-long working channel that accommodates standard 36-cm-long instruments.11,12 However, this laparoscope is not yet commercially available. Another potential drawback of the MAST technique is its application in the small pediatric patient. The small working space might not accommodate the DMG while still allowing for adequate traction on the appendix. However, this did not prove to be a problem in our present series that included patients as small as 25 kg.
In conclusion, MAST appendectomy is safe and effective in children. MAST appendectomy is a streamlined, minimally invasive approach that allows the surgeon to operate independently through a single 12-mm trocar. The technique recapitulates the triangulation that is achieved in conventional laparoscopy and is a practical solution to the poor ergonomics that is common in other SILS techniques.
Footnotes
Acknowledgments
We would like to thank Dr. Mariano Albertal for his assistance in preparing this article.
Disclosure Statement
Guillermo Dominguez is the owner of IMANLAP, Buenos Aires, Argentina.