
Abstract
Abstract
Aim:
We tested our laparoscopy-assisted “open” ligation (LOL) technique on testicular vessels.
Methods:
We ligated the left testicular artery and vein (TAV) in 8-week-old male Wister rats using LOL (LOL group; n=10) or laparotomy (open group; n=10). In LOL, a 0-degree laparoscope was introduced through a 5-mm epigastric trocar. A 3-mm grasper was used to expose the left TAV. A lapa-her-closure (LHC) needle loaded with 3-0 SurgiPro was directly inserted into the left lower quadrant where the left TAV should be and advanced under the vessels, and the suture material was released leaving one end outside. The LHC was then withdrawn a little and advanced again over the vessels to grasp the end of the suture material just released to bring it outside. This was proximally repeated. The two ends of both sutures were conventionally tied outside, and the knot was passed through the insertion site and tightened around the vessels. In the open group, the left TAV were ligated using two 3-0 SurgiPro ties. In both groups, the right side was left intact. All rats were sacrificed 2 weeks postoperatively, and both testes were examined with hematoxylin and eosin.
Results:
Treatment time was 5–7 minutes for LOL and 7–8 minutes for the open group. Postoperative recovery was uneventful. No adhesions were present between the ligated vessels and bowel in any rat. Histopathology of all left testes showed coagulative necrosis of germinal cells and seminiferous tubules; all right testes were normal.
Conclusion:
LOL appears to be as effective as open ligation and may find application for treating varicocele.
Introduction
Materials and Methods
Twenty male, 8-week-old Wister rats were the subjects for this study. All animals had unrestricted access to food and water preoperatively. The rats were placed supine and anesthetized with 2% isoflurane. The fur of the anterior abdominal wall was removed and the skin was prepared with 1% povidone–iodine solution. In the LOL group (n=10), a 5-mm trocar was inserted in the epigastrium using the open Hasson technique, and carbon dioxide was insufflated to 3 mmHg. A 0-degree laparoscope was introduced through the epigastric trocar. A 3-mm grasper was inserted into the right lower quadrant without a trocar to expose the TAV by retracting fat near the left inguinal ring toward the contralateral side, if necessary. A lapa-her-closure (LHC) needle loaded with 3-0 SurgiPro was directly inserted into the left lower quadrant at the point where the TAV should be and advanced under the vessels, and the suture material was released leaving the other end outside at the insertion site. The LHC was then withdrawn a little and advanced again, but this time over the vessels to grasp the end of the suture material just released and to bring it outside at the insertion site (Fig. 1). This was proximally repeated again. The two ends of both sutures were then conventionally tied as in any open procedure and the knot was passed through the insertion site and tightened around the vessels. The scope was then used to confirm that each tie was adequate before the vessels were ligated under laparoscopic control (Fig. 2). In the open group (n=10), laparotomy was performed through a lower midline abdominal incision. The left TAV were tied with two 3-0 SurgiPro ties and then ligated between the ties. In both groups, the right TAV were left intact. All rats were sacrificed 2 weeks postoperatively, and both testes were examined with hematoxylin and eosin to observe whether there was necrosis of germinal cells and seminiferous tubules. At sacrifice, the abdominal cavity was also macroscopically examined.
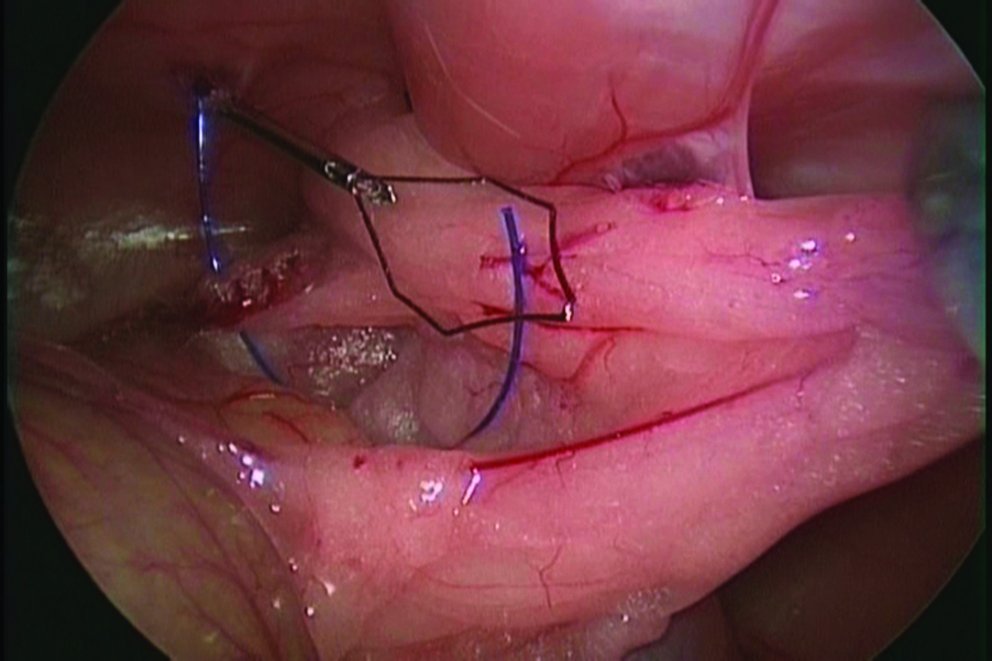
Lapa-her-closure (LHC) being used to ligate testicular artery and vein (TAV). An LHC needle loaded with 3-0 SurgiPro has been inserted and advanced under the vessels, and the suture material has been released. The LHC will then be withdrawn a little and advanced again, but this time over the vessels to grasp the end of the suture material just released and to bring it outside at the insertion site.
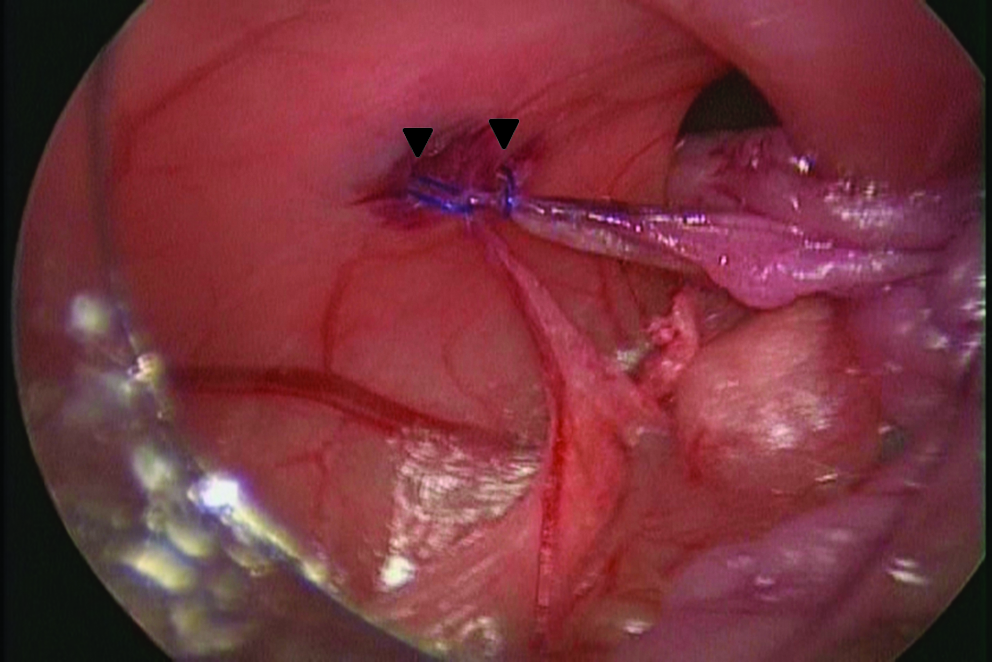
Double TAV ligation. Both ends of both sutures (arrowheads) are conventionally tied as in any open procedure, and the knot is passed through the insertion site and tightened around the vessels, under laparoscopic guidance.
Results
Treatment time, from skin incision to skin closure, ranged from 5 to 7 minutes for the LOL group and 7 to 8 minutes for the open group. There were no intraoperative complications and postoperative recovery was uneventful. At sacrifice, macroscopic examination of the abdomen failed to identify any adhesions between the ligated TAV and the small bowel in any rat. Histopathology of the treated left testis showed coagulative necrosis of the germinal cells and seminiferous tubules in all rats in both groups (Fig. 3). No histopathologic changes were observed in the untreated right testis in any rat in both groups.
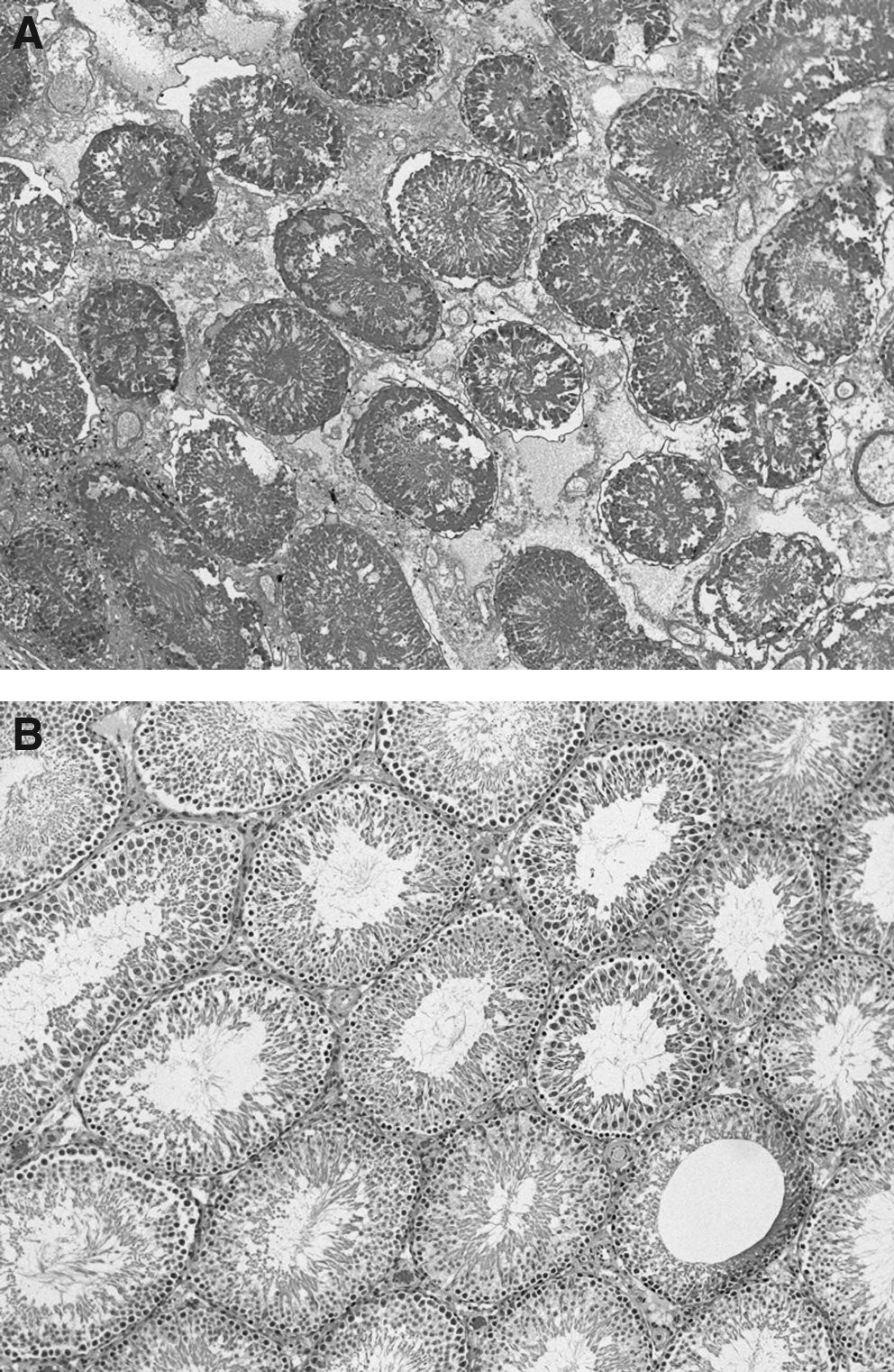
Hematoxylin and eosin histopathology of laparoscopy-assisted open vessel ligation treated left
Discussion
Minimally invasive surgery has been applied to a wide variety of urological procedures. The principal disadvantages of retroperitoneoscopy for the treatment of varicocele include insufficient space and difficulty in orientation. 5 Laparoscopic transperitoneal approach (LTP) is universally used despite an emphasis on extraperitoneal access for urological procedures. However, LTP carries the risk of serious injury to small bowel, sigmoid colon, nerves, and vessels.6,7 Use of energy sources during LTP is also associated with burns to bowel and neuropraxia. 6 In conventional LTP, a grasper and scissors are used to make two perpendicular incisions in the peritoneum overlying the TAV and the vessels must be lifted to make a space for ligation using clips. However, in our LOL, the TAV do not need to be lifted from the retroperitoneal wall, because the LHC device with suture is inserted from the outside through the abdominal wall, and ligation is performed outside the peritoneum, thus ensuring that our LOL is truly minimally invasive. Because our LOL does not involve any dissection, no energy source is required, so there is no risk for thermal injury. In addition, compared with LTP, our LOL is quicker and involves less expense, because fewer ports and trocars are used, with improved cosmesis. That is, we use one trocar for the scope and insert one other instrument directly without a trocar, compared with three trocars that are required for conventional LTP.
One issue that is important in relation to this study is that the anatomy of the TAV differs between humans and rats. In humans, the TAV are fixed in the retroperitoneal space, but in rats they lie in the intraperitoneal space connected to the retroperitoneum by mesentery, which can be easily mobilized. Just as laparoscopic-assisted percutaneous extraperitoneal closure (LPEC) 8 is being used more often for inguinal hernia repair, our LOL may find application for general vessel ligation using LHC in the way that a procedure similar to our LOL is used during LPEC.
Risk for postoperative hydrocele after LTP is reported to be from 3% to 25%,4,9 and risk for postoperative recurrence is 6.6% to 18%.10,11 As our study lacks follow-up, we cannot make any conclusion about the incidence of hydrocele and recurrence. But, in the short term, there was coagulative necrosis in both groups, without any complications, indicating that our LOL is as effective as open ligation, which allows us to progress to the next level of evaluating our LOL in larger animals.
We found our LOL to be as effective as open ligation for ligating TAV, and it is quicker and far less invasive. Thus, it could find practical application for the treatment of varicocele, and as a technique, our LOL could be adapted as a simpler way to ligate vessels laparoscopically.
Disclosure Statement
No competing financial interests exist.