
Abstract
Abstract
Objective:
To present our experience and the feasibility of retroperitoneal laparoscopic ureteroureterostomy (LUUS) for treatment of retrocaval ureter (RCU).
Patients and Methods:
A total of 12 patients with RCU underwent LUUS. To evaluate the retrocaval segment, we calibrated retrocaval segment by a number 8F catheter segment before laparoscopy. A three-port, finger-dissecting removal of the retroperitoneal fat, retroperitoneal approach was used. In all 12 cases, after the ureter had been released from the inferior vena cava (IVC), the ureter was transected at the lower part of the dilated ureter and positioned anterior to the IVC. A tension-free ureteroureteral anastomosis was completed with the intracorporal freehand suturing techniques. Follow-up studies were performed with intravenous urography and renal ultrasonography at 3 and 6 months postoperatively.
Results:
All operations were laparoscopically completed with no open conversion. The mean operating time was 112 minutes (range 89–158), and the mean anastomosis time was 42 minutes, for all cases. The mean blood loss was 35 mL (range 21–60). The retrocaval segments of the ureter were resected in 2 of 12 cases, because the 8F catheter could not negotiate the segment. No intraoperative complications occurred. Hydronephrosis in all patients was decreased substantially after surgery, and all patients were symptom free.
Conclusion:
Our results have demonstrated that retroperitoneal LUUS was a safe and effective procedure, and an excellent minimally invasive treatment option for RCU.
Introduction
Materials and Methods
Patients
Between January 2002 and June 2010, RCU was diagnosed in 12 patients (8 men and 4 women) at our institution, with a mean age of 35 years (range 19–45). Of the 12 patients, 10 were symptomatic, presenting with mild-to-moderate intermittent right-side flank pain and 2 patients were asymptomatic and were incidentally discovered to have right hydronephrosis by renal ultrasonography during health examinations. Three patients had concomitant urinary tract infection. All patients were preoperatively evaluated with renal ultrasonography, intravenous pyelography (IVP), and/or reconstructed spiral computed tomography. The diagnosis was made on IVP and/or reconstructed spiral computed tomography, which demonstrated a typical S-shape deformity of the ureter at the level of either the third or fourth lumbar vertebrae, as well as a moderate hydronephrosis and a dilated proximal ureter in all patients. All patients demonstrated type 1 of RCU, according to the classification scheme proposed by Bateson and Atkinson. 4 To evaluate the retrocaval segment, we calibrated retrocaval segment by a number 8F catheter segment before laparoscopy. IVU and renal ultrasonography were performed 3 and 6 months postoperatively. Thereafter, yearly follow-up was performed with either IVU or renal ultrasonography.
Laparoscopic techniques
Under general anesthesia and with the patient in the lithotomy position, a cystoscopy was performed, and a 8F ureteral catheter was placed to evaluate the retrocaval segment. Then, the patient was placed in a full lateral decubitus position. A retroperitoneal LUUS was routinely performed with three ports. A 2-cm skin incision was made below the 12th rib in the posterior axillary line (point A). The muscular layer and lumbodorsal fascia were bluntly divided by using vascular forceps; and then, an index finger was inserted to bluntly separate the retroperitoneal space. Retroperitoneal fat and peritoneal reflection were pushed laterally, and retroperitoneal working space was widened as far as possible by the index forefinger. Then, under the guidance of the index finger extending into the retroperitoneal space through the incision, a 10-mm trocar was inserted 2-cm above the superior border of the iliac crest in the midaxillary line (point B) for the laparoscope, and a 5-mm trocar was inserted below the costal margin in the anterior axillary line (point C). Another 10-mm trocar was inserted at point A, and the skin incision was sutured to avoid gas leakage. The pneumoretroperitoneum was established by carbon dioxide insufflation at 12–14 mmHg. Basically, our technique was as follows: after the retroperitoneal fat had been freed and removed out through the point A, Gerota's fascia was then incised longitudinally. The perirenal fat was dissected to reveal the posterior surface of the mid and lower pole of the kidney. The dilated ureter was fully mobilized using both blunt and sharp dissection, followed by the upper ureter (Fig. 1). The upper ureter was then mobilized behind the vena cava, and the distal segment of the dilated ureter should be enough to facilitate tension-free ureteroureteral anastomosis (Fig. 2). Then, the ureter at the lower part of the dilated ureter was transected (Fig. 3), and the ureter was repositioned to lie anterior to the vena cava. If the previous 8F catheter could not negotiate the retrocaval segment before laparoscopy, the retrocaval segment would be excised. The posterior ureteroureteral anastomosis was made with several interrupted 4-0 Vicryl sutures. The Double-J ureteral stent assembly was prepared. A 4F ureteral catheter with appropriate length as the guide wire was passed into the Double-J ureteral stent from the consecutive side holes into the stent to straighten the stent. The length from the side holes of the stent to its proximal end was approximately equal to that from the proximal ureteral stump to the renal pelvis. The stent assembly was grasped by two forceps, and the distal end of the stent with the guide wire was pushed into the ureter and bladder in an antegrade manner (Fig. 4). Then, the proximal end of the stent with the guide wire was pushed into the ureter and renal pelvis in a retrograde manner (Fig. 5); and after the proper position of the stent, the 4F ureteral catheter was pulled out from the side holes of the stent (Fig. 6). Fluoroscopy was performed if there were any concerns regarding positioning. The anterior ureteroureteral anastomosis was closed with an interrupted suture (Fig. 7). Hemostasis was checked carefully after lowering the pressure of the pneumoretroperitoneum. A closed suction drain was placed through the port B into the retroperitoneal space adjacent to the repair.
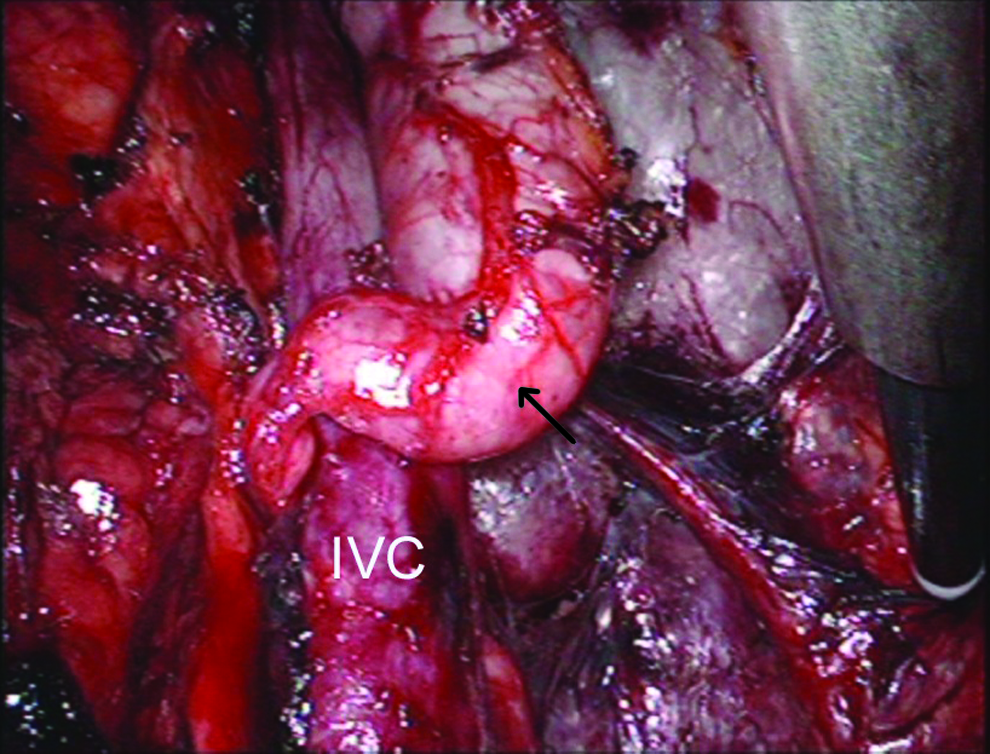
The dilated ureter are fully mobilized using both blunt and sharp dissection, followed by the upper ureter (arrow pointing to the proximal dilated ureter). IVC, inferior vena cava.
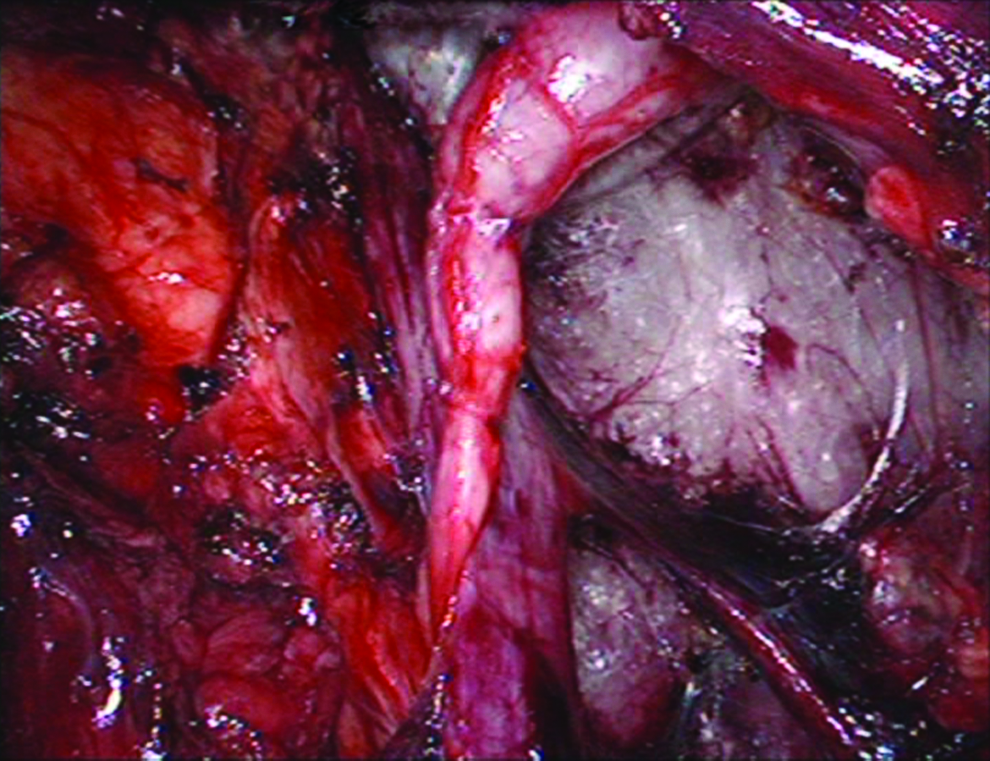
The upper ureter is then mobilized behind the vena cava.
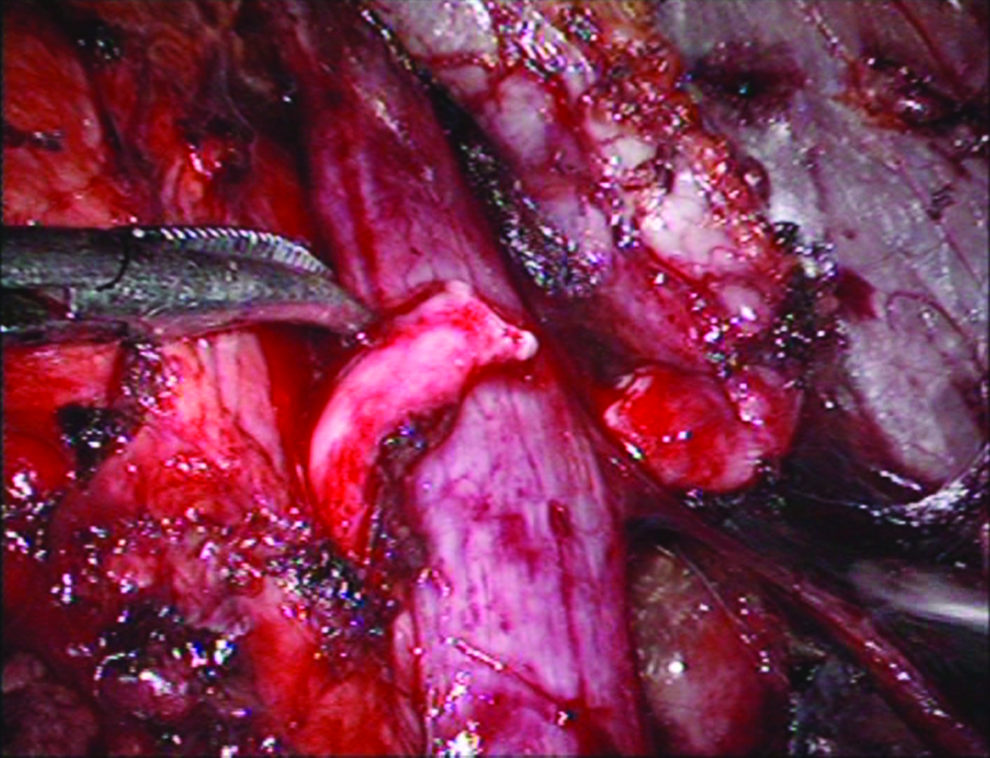
The ureter at the lower part of the dilated ureter is transected.
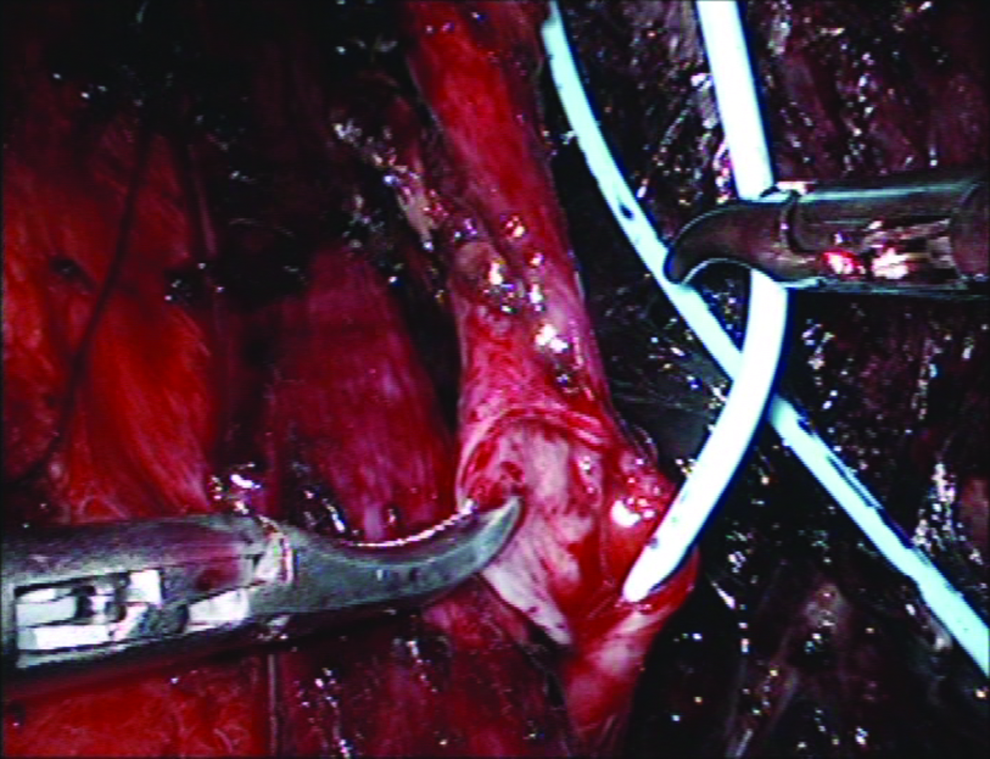
The distal end of the stent with the guide wire is pushed into the ureter and bladder in an antegrade manner.

The proximal end of the stent with the guide wire is pushed into the ureter and renal pelvis in a retrograde manner.

The 4F ureteral catheter is pulled out from the side holes of the stent.
Anastomosis is completed.
Results
All procedures were laparoscopically completed with no open conversion. The mean operating time was 112 minutes (range 89–158) for all cases, 158 minutes for the first case, and the mean anastomosis time was 42 minutes for all cases. The mean blood loss was 35 mL (range 21–60). The use of analgesics postoperatively was minimal. None of the patients required blood transfusion. No intraoperative complications occurred. The retrocaval segments of the ureter were resected in 2 of 12 cases, because the 8F catheter could not negotiate the retrocaval segment. The Foley catheter was removed 3–5 days postoperatively. The closed suction drain placed in the retroperitoneal space was removed 3–5 days postoperatively. The Double-J ureteral stent was removed 4–6 weeks postoperatively. The mean postoperative hospital stay was 6 days (range 5–7). No patient had problems in the early postoperative period. All patients achieved a rapid and uneventful recovery. Within the follow-up period, patients were tracked by IVU and renal ultrasonography at 3 and 6 months postoperatively and questioned for the presence of preoperative symptoms. Hydronephrosis in all patients was decreased substantially after surgery, and all patients declared that they were symptom free.
Discussion
RCU, also known as circum caval ureter, is a rare congenital anomaly in which the ureter passes behind the IVC, with an incidence of 1 in 1000 live births. The failure of the supracardinal vein to develop into the infrarenal IVC seems to be responsible for a retrocavally positioned right ureter. 5 The RCU usually manifests in the third or fourth decade. However, in our series, a 19-year-old man and a 21-year woman were included. The recent developments in imaging (such as reconstructed spiral computed tomography) and better accessibility to medical care could be responsible for the diagnosis and treatment of this anomaly more common at an early age. We believe that all patients suspected of having RCU after ultrasonography and IVU demonstrating hydronephrosis of the right kidney and an S-shape deformity of the ureter should undergo reconstructed spiral computed tomography or retrograde pyelography to rule out any concomitant disease or accompanied congenital abnormality.
To facilitate a tension-free anastomosis, adequate dissection and mobilization of the ureter and periureteral tissue is required. However, unnecessary dissection should be avoided to preserve the blood supply of the ureter. Although the retrocaval segment could be easily freed from the vena cava laparoscopically, the decision of whether to resect or preserve the retrocaval segment of the ureter has been controversial. 6 Singh et al. 7 and Li et al. 8 suggested that the retrocaval segment of the ureter was reserved when they had a grossly normal appearance without obvious stenosis, and the obvious stenotic retrocaval segment of the ureter was excised. Zhang et al. 9 suggested excising the retrocaval segment if a 8F catheter could not pass through the segment easily. To evaluate the retrocaval segment, we also calibrated a retrocaval segment by a number 8F catheter segment before laparoscopy. The reason that we chose the number 8F catheter for evaluating the retrocaval segment was that this method could be more objective and reliable compared with the appearance of the retrocaval segment observed through laparoscopy during the procedure. Our results showed that the retrocaval segment could be negotiated easily in the majority of the patients, thus being reserved in 10 of 12 cases. This is similar to what is recommended recently that in all of the cases (6 out of 6 cases), there was no need to remove the retrocaval segment. 1
Conventionally, open ureteroureterostomy has been the gold standard for the surgical correction of RCU for many years. Over recent years, however, technological breakthroughs coupled with the intensive growth of minimally invasive laparoscopic procedures have almost replaced open surgery. 10 In 1994, Baba et al. reported the first case of laparoscopic pyeloureterostomy for an RCU in 560 minutes. 11 Then, Matsuda et al. performed the LUUS by using the five-port approach in 450 minutes. 12 In 1999, Salomon et al. first did the laparoscopic retroperitoneal ureteroureterostomy of an RCU in 270 minutes, and suggested that this was a more direct approach with greatly reduced operative time. 13 In 2003, Bhandarkar et al. reported one case treated by laparoscopic pyelopyelostomy without excising the retrocaval segment in 250 minutes. 10 However, Nagraj et al. in 2006 reported the shortest operative time of only 100 minutes with LUUS by using a standard transperitoneal three-port approach. 14 Then, Simforoosh et al. reported a series of 6 cases who underwent laparoscopic pyelopyelostomy for RCU without resection of the retrocaval segment, with advantages of excellent outcome, minimal postoperative morbidity, short hospital stay, and highly satisfactory cosmetic results. However, the mean operative time in their study was 3 hours. 1 Although laparoscopic dismembered pyelopyelostomy,1,7,10,15,16 LUUS2,7,8,12–14,17–22 and pyeloureterostomy 11 were successfully performed in treatment of RCU, the very limited number of cases reported worldwide did not provide sufficient knowledge about the preferable surgical technique to correct this rare disease. Most case reports describe prolonged operative times, largely because of the initial difficulties with intracorporeal suture techniques. In our series, the mean operating time was only 112 minutes. The reduction of mean operating time may be explained by two reasons. First, our extensive experience with many retroperitoneal laparoscopic procedures that also required proficient intracorporal freehand suturing techniques, which overwhelmingly increased our self-confidence, could result in this change. Second, compared with transperitoneal approach, the retroperitoneal approach provided rapid and direct access to the urinary tract and avoided mobilization of intraperitoneal organs or retraction of organs, such as the liver. Our opinions were similar to those of Gupta et al., 18 who believed that the retroperitoneoscopic approach was safer, easier, and less time consuming, and it provided direct access to the ureter and IVC.
The placement of the Double-J ureteral stent is another technical challenge in LUUS for RCU. Some surgeons preferred to place the Double-J ureteral stent in a retrograde manner preoperatively using cystoscopy.10,13,18 Other surgeons preferred to place the Double-J ureteral stent in a conventional antegrade manner using a ureteral catheter or guide wire during the procedure.11,19,22–24 However, earlier the ureteral stent would hinder trimming of the ureter and suture of the posterior anastomosis. 8 Further, if the placement of the Double-J stent was performed in a conventional antegrade manner in LUUS, it could be difficult to place the proximal end of the Double-J stent into the renal pelvis after the ureteral catheter or guide wire was removed. In our procedure, a transanastomotic manner using one segment of 4F ureteral catheter with appropriate length was preferred to facilitate the placement of the Double-J ureteral stent during procedure, which was similar to the technique reported by Li et al., 8 who used two segments of 4F ureteral catheter passed into the stent from the side holes of the Double-J ureteral stent serving as the guide wires. However, the caudal ends of two segments of 4F ureteral catheter outside the stent could make it difficult to pass through the trocar.
Recently, the robotic technique has become incorporated into certain areas of urology, as in robotic ureteroureterostomy, and has become well accepted.25,26 The main advantage of this technique is that the movement of the articulated arm of the robot reproduces the action of the human wrist. Therefore, it provides more free mobility, which greatly aids intracorporeal suturing. 25 This may contribute to decreasing the complexity and length of operative time performing the anastomosis. However, a potential disadvantage of this technique is the costs, which may limit its development, especially in the developing countries.
Conclusion
Our results have demonstrated that retroperitoneal LUUS was a safe and effective procedure, and an excellent minimally invasive treatment option for RCU.
Footnotes
Disclosure Statement
No competing financial interests exist.