
Abstract
Abstract
Background:
Single-incision laparoscopy is an emerging technique that brings new challenges to laparoscopy and introduces new skills that a surgeon must learn. The learning needs for single-incision skills acquisition are unknown and no current guidelines exist for training or for its safe adoption.
Methods:
We developed an approach to adoption of new surgical techniques and applied it to single-incision laparoscopy. It is based on the following principles: a defined training algorithm, dry and wet-laboratory practice, a graded clinical introduction, and careful review of early outcomes. We analyzed its impact in our initial 40 patients.
Results:
Our training paradigm consisted of the following: attending a formal course, developing a simulation model, and animal laboratory training, followed by graduated clinical adoption. A 20% conversion rate to standard laparoscopy or open surgery occurred.
Conclusion:
Introducing a new surgical technique may not only offer potential advantages but also present significant risks. We developed a thoughtful approach to adoption that includes simulation-based training, progressive clinical adoption, and early review of outcomes. This approach may be applied to various new clinical applications.
Introduction
With the adoption of any new technique or new technology comes the risk of injury to the patient. A prime example of this was the rise in common duct injuries that was associated with the adoption of laparoscopic cholecystectomy. 3 Simulation has been proposed as a means of training physicians in practice in new techniques. 4 Simulation has also proved useful in the training of residents, to move as much of the learning curve to the preclinical arena. 5 Our goal in this project was to build on these existing concepts of simulation to develop an approach to adopting single-incision laparoscopy that would minimize the risk of patient injury through simulation, graduated adoption, and careful review of early clinical outcomes.
Materials and Methods
Planning and preclinical training
Prior to beginning our program in single-incision laparoscopy, we held meetings to define our goals, identify resources, and make plans for a careful clinical introduction of this new technique. These discussions included the two surgeons who were going to start the program (A.W. and B.O.) as well as divisional and departmental heads (C.P.). The two surgeons are both fellowship-trained in minimally invasive surgery, routinely perform advanced laparoscopic surgery, and have extensive laboratory experience with development of new techniques (including NOTES). Both surgeons and the institution at large have substantial involvement with simulation and education. Preclinical training was, therefore, carried out at the Institute for Simulation and Interprofessional Studies (ISIS) at the University of Washington. ISIS is a multidisciplinary center for simulation-based training and education. It has resources that include a simulation laboratory with multiple laparoscopic towers, fundamentals of laparoscopic surgery (FLS),6,7 and virtual reality–based laparoscopy trainers. It is also affiliated with the Center for Videoendoscopic Surgery (CVES), where all animal procedures were carried out. All animal training was carried out in accordance with the U.S.D.A. Animal Welfare Act and was approved by our institution's Animal Care and Use Committee. All animal procedures were terminal, and all were performed in animals already anesthetized for other laboratories to conserve resources.
Clinical case series
All cases were performed by one of two surgeons (A.W. and B.O.) at a single academic medical center. Although residents and/or fellows were involved in all cases, the attending surgeon was the operating surgeon for the entirety of each case. Regular discussions were held at our weekly CVES research meetings, discussing technical issues and complications. After the first 40 cases, we obtained Institutional Review Board (IRB) approval for a retrospective chart review of our series. Analyses were performed using descriptive statistics.
Results
Preclinical training
We established a paradigm of preclinical education followed by simulation-based training in both the dry and wet labs. This began with a review of the available literature, followed by attendance by one surgeon (A.W.) at a formal course. This course consisted of didactic sessions and observation of live cases in humans, but no laboratory experience. We then developed a single-incision laparoscopy simulator based on the FLS training program. A laparoscopic tower with a trainer box was modified with a single-incision laparoscopy port configuration using commercially available low-profile 5 mm ports. Dry-lab simulation with the modified FLS trainer box was utilized until both surgeons could comfortably perform the prescribed FLS tasks using the single-incision laparoscopy configuration and achieve similar completion times and rates of success. Intracorporeal suturing was not used as a benchmark because of the difficulty in performing this task with single-incision port configuration and currently available instruments. Simulator training was conducted using conventional straight instruments and commercially available articulating instruments from a variety of companies (Covidien Rotic Instruments, Norwalk CT; Cambridge Endoscopic Instruments, Framingham MA; Novare RealHand, Cupertino, CA).
In addition to dry-lab training, both surgeons participated in a series of four animal laboratories using a live nonsurvival porcine model. The porcine model was used to simulate and train for cholecystectomy and appendectomy, with the latter simulated by uterine horn mobilization and resection. A midline single incision was made, through which multiple low-profile ports were placed, simulating the anticipated port placement and configuration in human subjects. Various articulating dissectors and graspers were used until each surgeon settled on his choices and subsequently mastered their use. Both surgeons performed multiple single-incision laparoscopic cholecystectomy and appendectomy simulations on the live porcine models.
In addition to training with modified single-incision instrumentation, retraction was simulated and practiced as well. Pretied suture loops (Surgitie™; Covidien Rotic Instruments) were used to encircle and retract the uterine horns and fallopian tubes in the porcine model, simulating appendiceal retraction. Retraction of the gallbladder using percutaneously passed sutures on Keith needles was used to simulate and refine this retraction technique prior to clinical use in humans.
Graded clinical adoption
The principle of graded clinical application was applied with four elements in mind: selection of patients expected to be simpler, progressive elimination of ports, introduction of new retraction techniques, and low threshold for conversion. Laparoscopic cholecystectomy was chosen as the index single-incision laparoscopic operation, because it has a clear technique, there was consistency among surgeons with regard to port placement and retraction, and there were technical benchmarks with which to compare the single-incision technique, including obtaining the “critical view of safety” as described by Strasberg. 8 The technique itself was implemented with a gradual, stepwise reduction in ports until a true single-incision method was achieved. Patients were carefully selected for the single-incision laparoscopic approach, with our initial cases being those patients with symptomatic cholelithiasis without prior evidence of significant inflammation or biliary obstruction. Those patients with long torsos or obese abdomens were initially excluded because of the potential technical limitations with the instruments in their ability to reach or to utilize the abdominal wall as a fulcrum, respectively. Indications were broadened and patient selection was liberalized as experience grew.
We began our transition by using single-incision techniques for gallbladder retraction during standard laparoscopic cholecystectomy, using one less port in the right upper quadrant. Retraction was achieved with percutaneous placement of two to three sutures, placed intracorporeally with straight (Keith) needles, through the gallbladder fundus and infundibulum, to provide lateral and cephalad retraction (Fig. 1). This technique was identical to the one we used during our live animal porcine model simulation. After successful adoption of single-incision percutaneous suture retraction techniques, we began reducing the number of ports used, going to two-port cholecystectomy and finally arriving at a true single-incision technique. Early in our series we used 2–3 low-profile 5-mm ports through a transumbilical incision (Fig. 2a). We moved to a single port, multiple trocar system (SILS Port; Covidien Rotic Instruments) once it became commercially available (Fig. 2b).
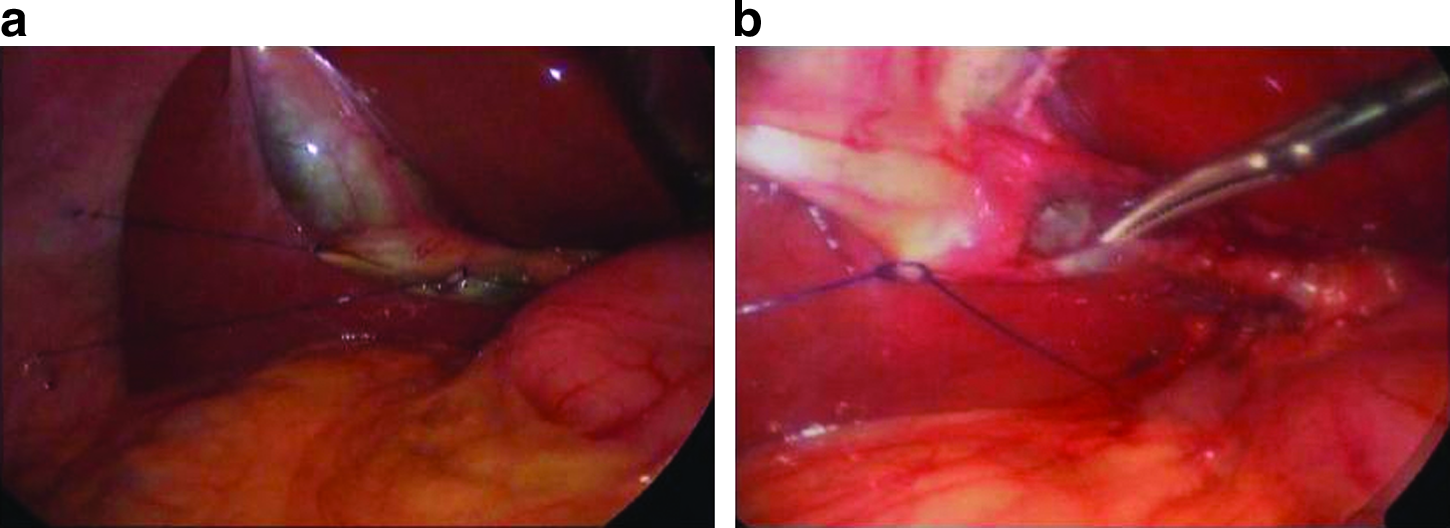
Single-incision cholecystectomy using transabdominal fixation sutures for retraction. (
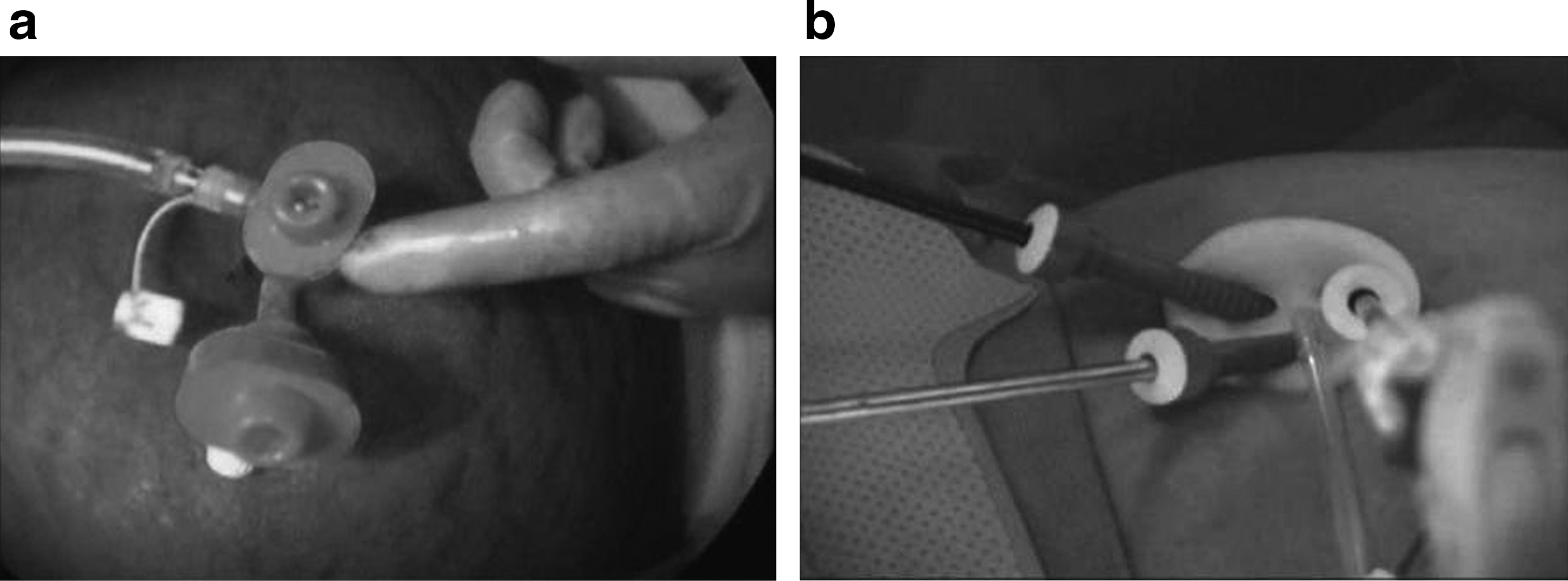
Access for single-incision laparoscopy.
After successful transition to a single-incision technique for laparoscopic cholecystectomy, we introduced the single-incision technique to appendectomy, laparoscopic adjustable gastric band (LAGB), and several other general surgical procedures. For the LAGB procedures, stay sutures on the gastric fundus were used for retraction. Appendiceal retraction was either through use of a laparoscopic grasper or through placement of a pretied suture loop around the appendix.
Informed consent was obtained from all patients and included a candid discussion of the novel nature of the single-incision technique and the potential for conversion to standard laparoscopy or open surgery. It was clearly discussed with patients that the potential benefits of this technique had not been yet demonstrated in any studies. Prior to clinical adoption, the new technique was discussed with the medical center's chief of general surgery and the chair of the department of surgery. As an extension of standard technique, single-incision laparoscopy was not felt to require separate credentialing or IRB approval as an experimental procedure.
Early clinical experience
Between August 2008 and May 2009, a total of 40 cases were attempted with single-incision laparoscopy, as summarized in Table 1. These included cholecystectomy, appendectomy, LAGB placement, jejunostomy-tube placement, and lysis of adhesions for small bowel obstruction. Our results and transition methods are shown in the following tables. All values, unless otherwise noted, represent averages±standard deviation.
Prior to performing a true single-incision laparoscopic cholecystectomy, we performed five transition cases, in which we used suture retraction techniques and evolved from four to two incisions, with one in the epigastrium and one at the umbilicus. No complications were observed in these five transition cases. As our technique improved with suture retraction, the epigastric port was eliminated and a true single-incision method was then used. Nineteen single-incision laparoscopic cholecystectomies were attempted (Table 2), with four cases requiring placement of additional ports (21%). In two of these cases, one additional trocar was utilized for difficulties with retraction or inflammation. Two cases required conversion to standard four-port laparoscopic cholecystectomy because of significant inflammation and adhesions. One of these was subsequently converted to an open procedure and resulted in a common bile duct injury. In this procedure, we first converted to standard laparoscopy immediately after entry into the abdomen because of the presence of severe, unsuspected inflammation. After a brief trial of standard laparoscopy, it was felt that the level of inflammation required conversion to open. During the open portion of the procedure, an injury to the common bile duct occurred. Intraoperative consultation by a hepatobiliary surgeon was obtained. It was discovered that the patient had unsuspected Mirizzi's syndrome requiring a hepaticojejunostomy for management. As the common duct injury occurred after laparotomy was performed, it was not felt to be due to the single-incision laparoscopy technique.
A total of 17 appendectomies were performed using single-incision methods (Table 3). All operations were performed through one skin incision in the umbilicus. All cases were successfully completed without conversion to an open procedure. Additional ports were required in 18%. Perforated appendicitis was observed in 2 patients, of which one required additional port placement for exposure. One patient had a retrocecal, inflamed appendix that required an additional port for retraction and exposure. One patient was found to have an appendiceal mass on exploration, which required additional port placement to perform partial cecectomy. (The frozen section pathology revealed endometrial implantation at the base of the appendix.) A technical instrument mishap occurred in 1 case, where a disposable, articulating grasper fractured and split within the abdomen. The shards of plastic were retrieved without injury to the patient and the case was successfully completed in single-incision fashion. No intraoperative complications were observed. Two patients developed postoperative pelvic abscesses, of which one required percutaneous drainage.
Our experience with single-incision laparoscopic adjustable band placement is limited to two procedures. No immediate intraoperative complications were noted. However, 1 patient suffered from an unrecognized gastric perforation, which led to significant morbidity and prolonged hospital stay from sepsis, enterocutaneous fistula formation, open abdomen, and ventral hernia formation. This perforation was on the anterior fundus, near or at the location of the fundus retraction suture. Because of the significant morbidity incurred in the 1 patient undergoing gastric band placement with single incision, we made a decision to put the single-incision gastric band initiative on hold. Two other general surgical procedures have been successfully performed at our institution using the single-incision laparoscopic technique. A jejunostomy tube was successfully placed in a patient with superior mesenteric artery (SMA) syndrome and intolerance to oral intake. A second patient was explored for small bowel obstruction with successful lysis of adhesions using the single-incision technique. Both cases were performed without additional ports and without complications.
Discussion
It is well established that the introduction of laparoscopy in the early 1990s was associated with an early rise in the number of surgical complications.3,9,10 Surgeons initially learned laparoscopic technique, typically through industry-sponsored courses, and then returned to their own institutions to begin a laparoscopic practice without formal certification, credentialing, supervision, or proctoring. The initial learning curve was associated with up to a 2% incidence of biliary tract injuries, a rate that fell to 0.1% after the initial learning curve. 9 A recent survey of more than 1400 surgeons showed that surgeons trained in laparoscopic cholecystectomy during residency were significantly less likely to have a common duct injury, showing the importance of a formalized training program. 11 Although perhaps not as revolutionary as the introduction of laparoscopy, single-incision laparoscopy presents many of the same issues. The procedures are technically more difficult, new instruments and techniques are in use, there is an as-yet-unknown learning curve, and the clinical benefits remain unclear. There are anecdotal reports and rumors of common duct injuries due to single-incision laparoscopic cholecystectomies, but none have been yet reported in the literature.
Keen about avoiding the errors of the past, our department developed a philosophy centered in the principle of primum non nocere (First, do no harm). With that in mind, and helped by the substantial progress in the science of simulation and modeling as a means to education, we developed a series of principles that we believe help in the introduction of a new technique. In this article, we discuss our experience using these principles during the introduction of single-incision laparoscopy. Thoughtful discussion of whether or not to adopt a new technique and careful selection of a few surgeons who will champion it and become the teachers of it, in combination with a carefully laid out training plan and a progressive introduction into clinical practice, proved to be beneficial in this particular case (single-incision laparoscopy), but can also be certainly applied to other new surgical techniques and technologies, including NOTES, endoluminal surgery, and robotics.
Single-incision laparoscopy is technically more challenging than traditional laparoscopy. Most practicing surgeons are familiar with the basic tenets of laparoscopy including the importance of port placement and appropriate instrument triangulation, methods for retraction and dissection, obtaining appropriate visual and tactile feedback, and correct perception of anatomic structures. Single-incision laparoscopy presents a challenge to each of these tenets. Instruments are inserted in-line, resulting in loss of triangulation internally and causing conflicts between the instruments and laparoscope externally (Fig. 3). The instruments are also in-line with the camera, changing the angles at which dissection is performed and possibly affecting visualization and perception of anatomy. Retraction is frequently impaired, as fewer instruments are available for insertion through one incision when compared with traditional multiple incision laparoscopy. To rectify some of these issues, many surgeons performing single-incision laparoscopy use articulating instruments, recreating triangulation for retraction and dissection (Fig. 3). These instruments, however, create their own problems with loss of dexterity, often requiring the surgeon to work with crossed instrument tips, that is, with the right hand controlling the screen-left instrument tip.

Internal and external conflicts caused by single-incision techniques.
It became clear throughout this experience that the substantial series of obstacles that needed to be overcome would, by common sense, lead to a higher risk of injury. Single-incision laparoscopy, we believe, is a field where clinical adoption should be preceded by a rigorous training process that includes didactic education and technical skill acquisition. This is ideally suited to training in a simulated environment. Technical difficulties and unfamiliarity with in-line instrumentation, articulating instruments, and crossed-hands are best overcome in a dry lab environment. We developed a single-incision laparoscopy trainer box by adapting the existing FLS program for several reasons. It is simple to set up and can be easily modified for single-incision tasks. The FLS trainer is a widely available, well-validated model for laparoscopic skills assessment. Its use in residency training programs is ubiquitous, and indeed, starting this year, FLS certification will be part of the American Board of Surgery's requirements for General Surgery certification. 12 Performance benchmarks for FLS tasks exist and can serve as a target for single-incision performance. We are currently using this modified FLS station to develop specific benchmarks and to establish learning curves for single-incision laparoscopy. The dry lab environment, however, does not adequately simulate retraction and in vivo manipulation of tissues. We therefore feel that live animal or cadaveric human training should be a very important component of training for surgeons prior to clinical implementation of single-incision laparoscopy.
Whenever any new procedure is introduced, surgeons should carefully follow and evaluate clinical results. In our practice, single-incision techniques were introduced for one procedure (cholecystectomy) by two highly trained surgeons using a graded process of adoption. Weekly research meetings allowed for technical pearls and pitfalls to be shared between the two surgeons and also encouraged early recognition of any problems or clinical issues. There were two major complications in this series, one of which we feel was due to the introduction of single-incision laparoscopy. In that case, retraction of the fundus of the stomach during LAGB was with a suture rather than our standard technique of using a grasper. Although we cannot be certain that the missed gastric perforation was due to suture retraction, as opposed to cautery injury or some other cause, it is certainly the leading suspect. Early recognition of the potential danger of suture retraction in LAGB led to us deciding to stop our single-incision LAGB program.
Despite careful patient selection, we observed that we needed additional ports in nearly 20% of cases. Common reasons for needing to add additional ports or convert to an open procedure included difficulty with retraction or with dissection, especially in the face of inflammation and adhesions. It is important to note that placement of additional ports should not be considered a complication or failure of technique, but reflects prudent surgical judgment. Although this study did not compare single-incision technique with standard laparoscopic techniques, it became clear to us that our operative times for single-incision laparoscopic cases were longer than our typical operative times for standard laparoscopic procedures. We accepted those longer times for the sake of patient safety and appropriate learning, and like the placement of additional ports, did not pressure anyone who took longer.
We have not made comparisons between single-incision and standard laparoscopy in terms of outcomes, as this study was not meant to answer questions regarding clinical effectiveness of this new approach. Instead, we present a relatively new approach to the safe introduction of a new surgical option. This path, an expression of a new philosophy and one that is applicable well beyond single-incision laparoscopy, will not only improve outcomes and prevent complications associated with the learning curve of a new procedure, but also provide preliminary data that may result in a broader adoption of the technique or the decision to abandon it. The American College of Surgeons has commented on and provided guidelines for surgeons as they acquire new skills and provided guidance on implementation of new technologies. These guidelines on adoption of new technologies include assessment of their safety, efficacy, and need, obtaining appropriate training and mentoring prior to clinical adoption, and continual reassessment of outcomes to ensure that appropriate care is being delivered to patients.13,14 We agree with these recommendations and they were the guiding principles for our adoption strategy.
Conclusion
Single-incision laparoscopy is technically more difficult than standard laparoscopy. No standard curricula exist for training or certifying surgeons in single-incision laparoscopic procedures. The learning curve for single-incision laparoscopy still needs to be determined, as are the processes to accredit surgeons in its use. Based on the results of our study, we recommend extensive preclinical training in a simulation center and animal laboratory, as well as participation in a formal training course. We also recommend a graduated, careful clinical adoption, beginning with relatively simple cases and progressing to more challenging patients and procedures. One should have a low threshold for conversion to standard laparoscopy or even open surgery. Early postoperative outcomes must be assessed and compared with historical standards. This paradigm can serve as a model for surgeons adopting single-incision laparoscopy as well as for future clinical adoption of other new procedures and technologies.
Footnotes
Disclosure Statement
No competing financial interests exist.