
Abstract
Abstract
Introduction:
Abdominoscrotal hydroceles (ASH) represent a difficult surgical problem in which a large scrotal hydrocele extends through the inguinal canal into the intraabdominal, extraperitoneal space, creating a widened internal ring that may be associated with an inguinal hernia.
Subjects and Methods:
Patients with ASH were repaired using a combined laparoscopic–inguinal approach. Laparoscopic exploration was used to confirm the diagnosis, rule out associated hernia, assess for contralateral pathology, and confirm adequate peritoneal closure at the level of the internal ring, after a standard inguinal approach was used to repair the ASH.
Results:
Eight patients are described with a median age of 13 months. One patient presented with bilateral ASH, and 5 patients had contralateral pathology, including simple hydrocele (n=3), undescended testicle (n=1), and inguinal hernia (n=2). Three patients were confirmed to have an ipsilateral inguinal hernia associated with their ASH. Postoperative complications included hematoma (n=2) and recurrent hydrocele (n=1). No patient developed ipsilateral or contralateral hernias following ASH repair (median follow-up, 3.2 years).
Conclusions:
Although laparoscopy is not essential, we have found it to be a useful adjunct to ensure accurate diagnosis and repair of abdominoscrotal hydroceles in children.
Introduction
The treatment of ASH is surgical, with inguinal, scrotal, abdominal, and laparoscopic approaches described. In this article we review our institution's experience with a combined laparoscopic–inguinal approach to demonstrate its usefulness in the repair of ASH and the assessment of associated pathology.
Subjects and Methods
We performed a retrospective chart review of 8 patients who underwent laparoscopic assisted ASH repair from January 2000 to March 2011 at the Montreal Children's Hospital, McGill University Health Centre, Montreal, QC, Canada. Patient demographics, preoperative imaging, operative details, and postoperative complications are described. Ethics approval was granted by the Director of Professional Services at the Montreal Children's Hospital, McGill University Health Centre (Project 2010-44), as per provincial regulations.
Surgical technique
A combined laparoscopic–inguinal approach was used to repair the ASH. A single umbilical port was inserted to allow evaluation of the abdominal component of the ASH and to assess for related pathology such as ipsilateral or contralateral indirect inguinal hernias or undescended testicles (Fig. 1). The laparoscope was then removed, the abdomen was deflated, and our attention turned to the groin, where a standard inguinal approach was used to isolate the spermatic cord and associated hydrocele. The anterior wall of the hydrocele was opened to allow for decompression. The abdominal component was then delivered through the groin incision where the hydrocele sac was carefully dissected off the spermatic cord and excised. The indirect hernia sac was then transfixed and tied. Laparoscopy was then used to confirm complete peritoneal closure at the level of the internal ring. If necessary the internal ring was narrowed, and orchiopexy was performed.
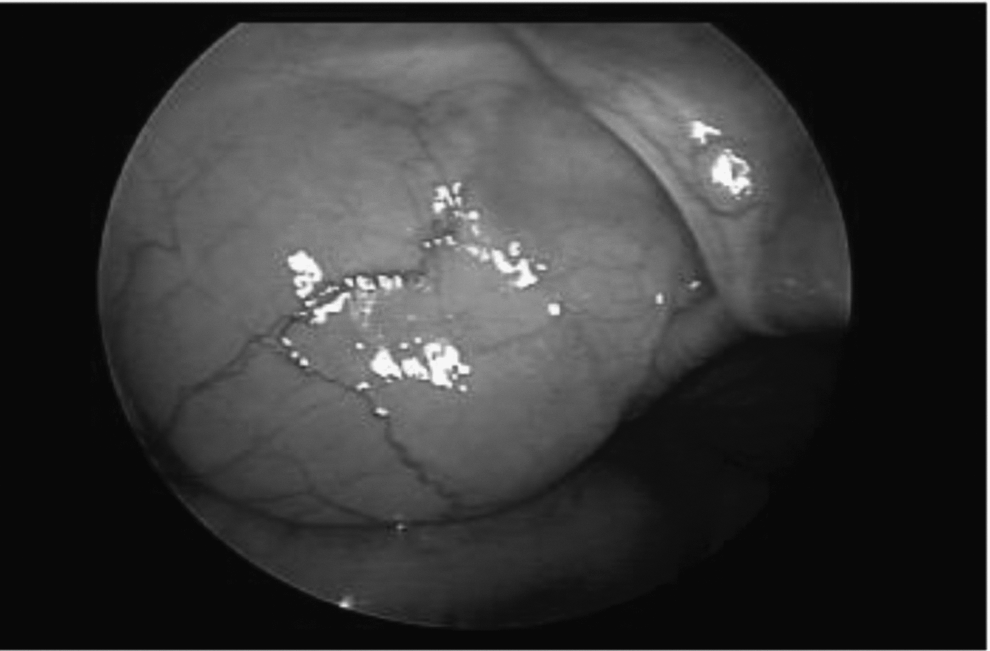
Laparoscopic view of an abdominoscrotal hydrocele.
Results
Eight patients with ASH were operated on using the combined laparoscopic–inguinal approach. The median age at time of repair was 13 months (minimum, 9.2 months; maximum, 21.9 months). Ultrasound was used in the diagnostic evaluation of 3 patients (Fig. 2). Patient characteristics including diagnoses and surgical outcomes are listed in Table 1. One patient was found by laparoscopy to have a breach in the peritoneum at the level of the internal ring following inguinal repair; this was sutured closed via the groin incision. The median length of follow-up was 3.2 years (minimum, 13 days; maximum, 11.2 years). Early postoperative complications included inguinal swelling (n=6), hematoma (n=2), recurrent contralateral hydrocele (n=1), and postoperative vomiting (n=1). All early complications resolved except for a small contralateral hydrocele in 1 patient. No patient developed ipsilateral or contralateral hernias following laparoscopic-assisted ASH repair.

Ultrasound of an abdominoscrotal hydrocele with a large preperitoneal component. ABD, abdomen; SCRO, scrotum. RT LG ING CANAL, right longitudinal inguinal canal.
ASH, abdominoscrotal hydroceles.
Discussion
ASH represent 0.4 to 3.1% of all infantile hydroceles.4,6 They may be bilateral or associated with contralateral simple hydroceles, indirect inguinal hernias, or testicular abnormalities.2,6 ASH are suspected clinically in children with large hydroceles that appear completely reducible on examination but recur immediately upon release of the scrotal pressure. A suprapubic mass may also be appreciated in a cooperative child while the scrotal component is being reduced. Ultrasound examination is useful to confirm the diagnosis but is not essential (Fig. 2). Young infants may be initially managed with observation as with regular hydroceles, but complete resolution is uncommon.
In our series of 8 patients, 1 had a bilateral ASH, 3 had ipsilateral inguinal hernias, 2 had contralateral inguinal hernias, and 1 had a testicular abnormality. The use of laparoscopy allowed for assessment of the intraabdominal component, as well as visualization of the internal inguinal ring before and during repair. This allowed confirmation of the adequacy of hernia repair at the time of hydrocelectomy. Furthermore, one patient without an associated hernia had a breech in the peritoneum created during removal of the abdominal portion of the ASH. This was seen on final laparoscopic assessment and repaired to prevent future herniation of abdominal contents through the widened inguinal canal.
There are many different surgical repairs for ASH described in the literature.8–12 We use laparoscopy as an adjunct to the traditional inguinal approach in which the hydrocele sac is dissected off the spermatic cord and removed in its entirety. This is not a simple procedure as the sac is often adherent to the spermatic cord, making identification and dissection of the vas deferens and spermatic vessels difficult.
Abel et al. 8 used a similar laparoscopic approach in which they assessed the abdominal portion of the ASH prior to inguinal repair. In their series they used three ports and decompressed the abdominal component prior to inguinal repair. We chose to use only one port and decompressed the ASH through the inguinal incision, delivering the intraabdominal, extraperitoneal portion through the internal ring before complete resection.
In 2001 Belman 10 reported a primary scrotal approach for ASH. In his repair a midline scrotal incision is made, exposing the tunica vaginalis. The hydrocele is drained via aspiration, and the tunica vaginalis is opened anteriorly. A clamp is then used to grasp the proximal portion of the sac, which is pulled into the field of vision. The tunica is then plicated without excision of the sac as in the repair of noncommunicating hydroceles.10,11 In this report, 2 patients with associated pathology required a second operation: one orchidopexy for an undescended testicle and another ipsilateral hernia repair. 10 Both these operations could have been avoided with the use of the laparoscopic–inguinal approach.
This series is limited in its small sample size and lack of long-term follow-up on fertility outcomes. We have demonstrated resolution of postoperative swelling without recurrence of ipsilateral hernias or hydroceles at median follow-up of 3.2 years. Longer follow-up is needed to comment on fertility outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.