
Abstract
Abstract
Objective:
Herein, we report our experience with retroperitoneoscopic partial nephrectomy (RPN) without hilar occlusion by the use of a laparoscopic clamp to induce selective regional ischemia.
Methods:
A 48-year-old woman was referred for a left upper polar renal mass, which was suspected to be malignant. The contralateral kidney revealed severe atrophy, and she was scheduled to undergo RPN using a laparoscopic clamp to induce selective regional ischemia. At first, the kidney is fully mobilized within the retroperitoneal space. Thereafter, the laparoscopic clamp is applied directly to the kidney, about 1 cm below the resection line. When closed, the renal parenchyma is compressed, so that blood supply to the tumor is interrupted. The preserved portion of the kidney is perfused normally, and it is possible to remove the tumor in a bloodless field without involving warm ischemia.
Results:
Renal hilar clamping was avoided, with minimal estimated blood loss. There was no perioperative complication, and the final pathology revealed a hemorrhagic renal cyst. The radioisotope absorption of the enucleated kidney was well maintained, except for the marginal area of the enucleated site. The renogram pattern was found to be equivocal when compared with the preoperative renogram.
Conclusion:
Regional renal parenchymal clamping during RPN can be safely and effectively used to create a bloodless operative field. Moreover, our preliminary experience demonstrates that this technique facilitates maximal nephron-sparing surgery for patients with an anatomically or functionally solitary kidney, without involving warm ischemia.
Introduction
The laparoscopic Simon clamp (Aesculap AG, Tuttlingen, Germany) is a newly developed laparoscopic clamp with a standard locking ratchet handle and an open jaw diameter of 70 mm. 4 The clamp can be placed along the renal parenchyma immediately surrounding the optimally located renal masses, thus creating regional renal ischemia and limiting injury to the unaffected portions of the kidney. Viprakasit et al. 5 reported their initial experience using a laparoscopic Simon clamp to induce selective regional ischemia during robotic-assisted PN without hilar occlusion for 3 cases of elective indication. In our opinion, regional renal parenchymal clamping during PN would be more significant and favorable for patients with an anatomically or functionally solitary kidney. Creating regional renal ischemia could avoid potential injury to the unaffected portions of the kidney, but its effect on the renal function and recovery for patients with an anatomically or functionally solitary kidney is not known. Here we describe our experience with retroperitoneoscopic PN (RPN) by using the laparoscopic Simon clamp to induce selective regional ischemia, without renal hilar clamping, for a patient with a functionally solitary kidney.
Materials and Methods
Patient
A 48-year-old woman was referred for a single renal mass, which was suspected to be malignant, and was incidentally detected by ultrasound examination. She had been diagnosed with systemic lupus erythematosus and treated with a prednisone. Subsequent evaluations, including magnetic resonance imaging and computed tomography, revealed a solid exophytic tumor (maximum diameter, 27 mm), located on the left upper polar kidney adjacent to the collecting system (Fig. 1). The contralateral kidney revealed severe atrophy, probably due to reflux nephropathy. Laboratory tests and the glomerular filtration rate (GFR) measured by 99mTc-diethylene-triamine-pentacetate renogram revealed chronic renal insufficiency (creatinine=2.6 mg/dL; GFR, right=5.6 mL/minute, left=8.8 mL/minute, total=14.4 mL/minute). We presented her with the options for managing this complicated renal mass, namely, radiographic surveillance or PN. She hesitated to proceed with radiographic surveillance because if the mass enlarges, radical nephrectomy emerges as an oncological view. After discussion of the options, the patient elected for RPN.

Computed tomography scan showing the 2.7-cm renal tumor in the upper pole of the left kidney (arrowheads). The contralateral kidney revealed severe atrophy (arrow).
Operative technique
After administration of general anesthesia, the patient was placed in the lateral decubitus position. The first incision was made 2 cm below the tip of the 12th rib, and a retroperitoneal space was created with a preperitoneal distention balloon system. We then inspected the working space through the balloon to ensure that we were in the correct plane. Subsequently, the balloon trocar was replaced with a blunt-tip trocar, and the insufflation pressure was maintained at 10 mm Hg. Two 12-mm ports were visually placed in the posterior axillary line. Another two 5-mm ports were placed in the anterior axillary line, taking care to avoid the peritoneum (Fig. 2). The plane anterior to the psoas muscle was developed. Thereafter, the kidney was dissected circumferentially and fully mobilized within the retroperitoneal space. After incision of Gerota's fascia to expose the renal mass, the surrounding perinephric fat was removed, except for the portion overlaying the tumor, which could be grasped during manipulation. Laparoscopic ultrasonography using a 5–10-mHz flexible laparoscopic transducer (Aloka, Wallingford, CT) was used to identify the tumor location and the surgical margins. The incision line, which was 1 cm from the tumor margin, was marked circumferentially on the renal capsule by using electrocautery scissors. After intravenous administration of 25 g of mannitol, the laparoscopic Simon clamp was introduced through the posterocaudal 12-mm port to allow for closure and placed adequately along the tumor margin (Fig. 3a). At first, the clamp was locked into place approximately 1 cm from the tumor margin in order to create regional renal ischemia and to minimize ischemic injury to the unaffected portions of the kidney. As mass excision by the laparoscopic scissor advanced deeper, the Simon clamp was unlatched and shifted 1 cm proximally. Because the kidney was fully mobilized within the retroperitoneal space, once the Simon clamp was closed, it allowed rotation of the kidney for optimal tumor visualization and supported excision of the tumor. The preserved portion of the kidney was perfused normally; therefore, the tumor could be removed without involving warm ischemia (Fig. 3b). After complete excision, biopsy specimens from the tumor bed were sent for frozen-section study. During hemostasis, the jaw pressure was temporarily reduced to better visualize the arterial bleeding site, which was then cauterized with standard reusable bipolar electrocautery (Fig. 3c). After good hemostasis was achieved, the Simon clamp was removed. The presence of urine leakage was investigated by intravenous injection of indigotindisulfonate sodium; however, no entry into the collecting system was noted. Parenchymal sutures using 2-0 Vicryl (Ethicon, Inc., Johnson & Johnson, Somerville, NJ) sutures on an SH needle were placed for cross-compression along the defect. Rolled Surgicel® (Ethicon, Inc.) bolsters were then applied to the tumor bed, and the pledgeted parenchymal sutures were tied down across the bolsters to provide additional compressive hemostasis. After confirmation of the margin status, a drain was placed, and the port sites were closed in the routine manner.

Port placement. Three 12-mm (▪) and two 5-mm (○) ports were used. Port C was for the laparoscope, and port S was used to insert a laparoscopic Simon clamp.
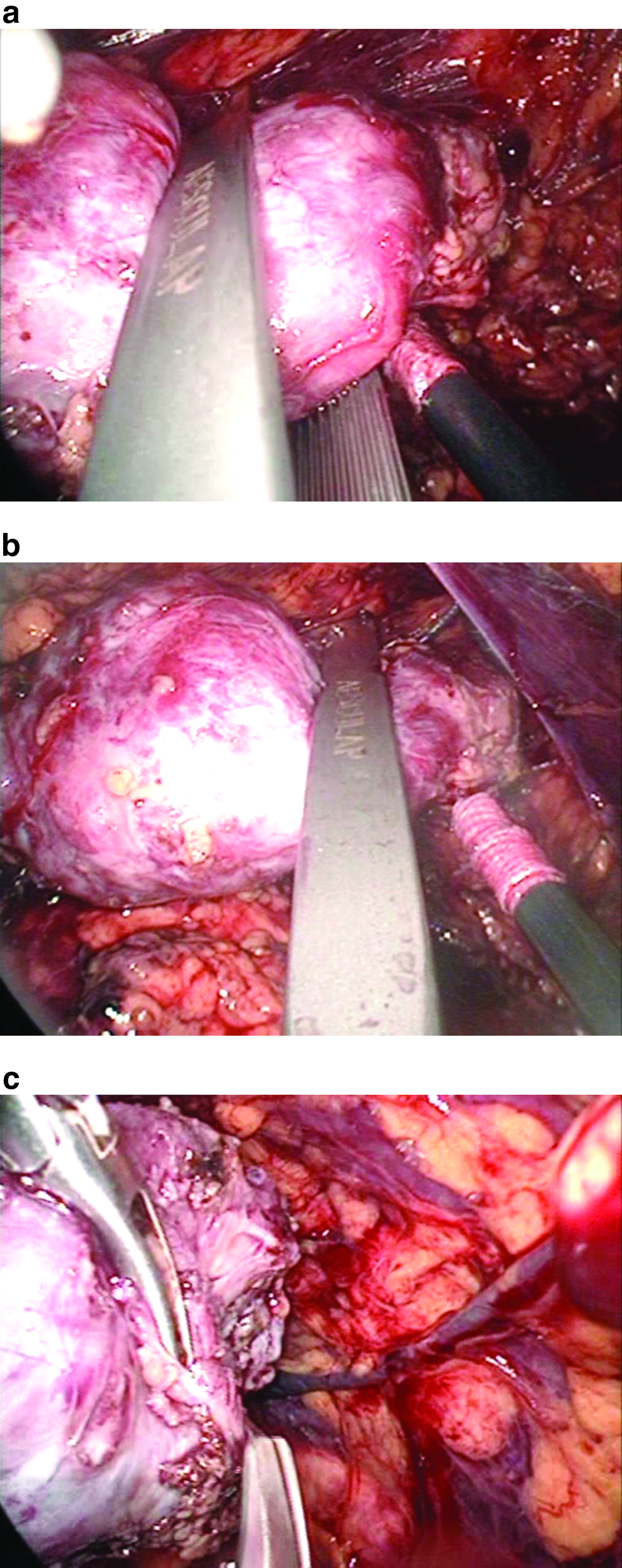
Operative view of the retroperitoneoscopic partial nephrectomy.
Results
The total operative time was 270 minutes, and the selective clamping time was 25 minutes. The estimated blood loss was minimal, and no blood transfusion was necessary. No complications were noted intraoperatively or postoperatively. Final pathology revealed a hemorrhagic renal cyst; it was negative for malignancy. To investigate the postoperative renal function damaged by PN, a 99mTc-mercapto-acetylglycyl-glycyl-glycine scan was performed 7 days after the surgery. The radioisotope absorption of the enucleated kidney was well maintained except for the marginal area of the enucleated site. The renogram pattern was found to be equivocal with no loss of function compared with that before the operation: GFR before operation, right=5.6 mL/minute, left=8.8 mL/minute, total=14.4 mL/minute; GFR 7 days after operation, right=5.8 mL/minute, left=11.9 mL/minute, total=17.7 mL/minute.
Discussion
PN provides an effective therapy for patients who require preservation of renal function. From a technical perspective, there are two different strategies for LPN: One is resection of the tumor without ischemia, and the other is established by complete renal ischemia by clamping the renal vessels. With the non-ischemic technique, a variety of energy sources may be used as an adjunctive measure to minimize hemorrhage, including ultrasonic shears, 6 water-jet dissector, 7 diode laser, 8 floating-ball radiofrequency dissector, 9 microwaves, 10 and radiofrequency coagulation. 11 Nevertheless, there are several major drawbacks to these techniques. Because of ongoing burning and charring of the tissue and permanent bleeding, it becomes impossible to distinguish between normal parenchyma and the tumor tissue, and therefore a positive surgical margin cannot be assured. 12 Moreover, unexpected collateral thermal damage to the surrounding structures, such as the arteries, veins, and the collecting system, may cause several troublesome postoperative complications such as urinoma, pelvicaliceal stenosis, and renal arteriovenous fistula.10,13,14 Therefore, its indications should be highly limited to small exophytic renal tumors with adequate intervening renal parenchyma as far as the renal collecting system, in order to minimize serious complications. In Japan, microwave tissue coagulator is widely used for LPN, and we traditionally used this modality for LPN. The microwave tissue coagulator is applied peripherally in the healthy parenchyma surrounding the tumor with circumferential punctures producing coagulation of a conical-shaped portion of tissue. Subsequently, a wedge resection can be achieved in the bloodless field without renal pedicle clamping. However, there is some risk that this procedure will cause relatively large-volume parenchymal damage around the PN site. Therefore, we could not use this modality for a patient with an anatomically or functionally solitary kidney. On the other hand, in the complete renal ischemia techniques, the renal pedicle needs to be dissected, and the renal artery is clamped with a Satinsky or bulldog clamp to stop blood supply to the entire kidney. 15 This is a time-consuming and potentially dangerous procedure, with the risk of damage to the major blood vessels of the kidney. 16 The major concern in this context, however, is the duration of renal ischemia after hilar clamping. It is important that the ischemia time in LPN is at least 50% longer than in the open technique, even when performed by highly experienced hands. 17 Although renal injury from warm ischemia is transient and spontaneously reversible in patients with an anatomically or functionally solitary kidney, the detrimental impact of ischemia can potentially be even greater. 18 Therefore, LPN for a patient with a solitary kidney poses a unique surgical and clinical management challenge.
In our opinion, when LPN is performed on patients with solitary kidneys or impaired renal function, creating regional renal ischemia by using the Simon clamp would be more favorable than the conventional use of complete renal hilar clamping, for several reasons. First, this procedure omits the excessive skeletonization of the renal vessels and therefore reduces the risk of damage to the major vessels of the kidney. Moreover, it permits normal blood perfusion of the unclamped kidney during LPN, thus reducing the risk of ischemic damage to the entire kidney. This device also provides a uniform and constant pressure over the length of the jaws without crushing the renal parenchyma. Excision can be done in a bloodless field without any hurry or fear of renal ischemia; therefore, it allows surgical precision during tumor excision and may be associated with the ability to achieve maximal nephron preservation. A comparison of the preoperative and postoperative renogram patterns confirms the preservation of kidney functioning outcomes and supports the feasibility and effectiveness of this technique, even in the patient with a functionally solitary kidney.
We place the Simon clamp in the most posterocaudal assistant port to minimize the interference from the movement of the laparoscopic instrument, but the Simon clamp was not an obstacle during tumor resection. On the contrary, the Simon clamp grasps the entire kidney, and it is therefore mandatory to fully mobilize the kidney in the limited retroperitoneal space. During mass excision, the direction and angle of the kidney could be easily and precisely changed in a timely manner, and this facilitated precise tumor excision. However, we could not apply this modality for those with central or hilar tumors because of the impossibility of placing the clamp. This technique is more ideal for polar tumors where less ischemia of normal tissue also occurs.
This technique does not require advanced laparoscopic skill and maintains the advantages of minimally invasive surgery, while minimizing the risk of unexpected renal ischemic damage. We believe that this procedure can be easily performed by many urologists. In addition, this technique may be practical for the laparoscopic partial resection of other vascular solid organs.
Regional renal parenchymal clamping during RPN can be safely and effectively used to create a bloodless operative field. Our experience with this technique demonstrates the ability to perform maximal nephron-sparing surgery for patients with an anatomically or functionally solitary kidney, without involving warm ischemia.
Footnotes
Disclosure Statement
No competing financial interests exist.