
Abstract
Abstract
Introduction:
There is an ongoing debate on whether it is safe to push the boundaries and widen the indications of laparoscopic liver surgery after careful patient selection. We report 2 cases of pure laparoscopic en bloc left hemihepatectomy and caudate lobe resection for intrahepatic cholangiocarcinoma (ICC).
Methods:
The first patient (a 79-year old) had an ICC affecting segments 2, 3, and 4 of the liver with dilatation of segment 1 ducts at preoperative imaging. The second patient (an 81-year old) had an ICC affecting segments 2, 3 with local invasion of segment 1. Both patients underwent pure laparoscopic left hemihepatectomy and caudate lobe resection.
Results:
The first patient's operative time was 360 minutes and blood loss was 390 mL. Postoperative hospital stay was 8 days. The definitive histology was as follows: pT1 ICC (25 mm in maximal diameter), with 20 mm free resection margin. The second patient's operative time was 310 minutes and blood loss was 300 mL. Postoperative hospital stay was 4 days. The definitive histology was as follows: T1 ICC (49 mm in maximal diameter) with 10 mm free resection margin. The first patient was disease free 12 months after surgery. The second patient died 11 months after surgery of metastatic disease.
Conclusion:
Pure laparoscopic left hemihepatectomy and caudate lobectomy for ICC may be feasible and safe. This is, however, a very complex procedure requiring extensive experience in laparoscopic liver surgery and careful patient selection to optimize surgical outcome. To our knowledge, this is the first systematic description of a pure laparoscopic en bloc left hemihepatectomy and caudate lobe resection for ICC.
Introduction
Intrahepatic cholangiocarcinomas (ICC) account for 5%–10% of primary hepatic malignancies and 6% of all cholangiocarcinomas in Western countries.4–6 Diagnosis is often incidental, as ICC is usually asymptomatic.4,7 The differential diagnosis is mainly with colorectal carcinoma metastases. The Liver Cancer Study Group of Japan proposed a classification of ICC intro three types on the basis of the macroscopic findings: mass forming (the commonest type); periductal infiltrating; and intra-ductal growth type. The ICC may have mixed components, with intra-ductal growth type having a more favourable prognosis after resection.8,9 When feasible, surgery remains the most suitable treatment option. 5 The need for caudate resection may add significant challenges to an already complex major resection.
We present the cases of 2 patients who successfully underwent a pure laparoscopic left hemihepatectomy and en bloc caudate lobectomy for an ICC involving the left biliary duct and affecting the caudate lobe. The feasibility, safety, and oncological efficiency of this technically challenging procedure are discussed. To our knowledge, this is the first systematic description of a pure laparoscopic en bloc left hemihepatectomy and caudate lobe resection for ICC.
First case
A 79-year-old man was referred to our unit for review after an incidental identification of an ICC during routine follow-up for prostate cancer. He suffered from type 2 diabetes mellitus, ischemic heart disease, and hypertension. His past surgical history included anterior resection for upper rectal carcinoma 10 years earlier, and right hip replacement 4 years earlier.
The computed tomography (CT) scan performed for surveillance for his prostate cancer showed a left liver mass. He subsequently underwent magnetic resonance cholangio-pancreatography (MRCP) revealing an intra-hepatic lesion involving segments 2, 3 and 4, but away from the biliary confluence. Dilatation was noted in segment one ducts, thus suggesting possible caudate lobe involvement (Fig. 1). Abdominal and chest imaging showed no evidence of distant metastases. A decision for left hemihepatectomy and caudate lobectomy was taken after discussion at our multidisciplinary team meeting with surgeons, pathologists, oncologists, gastroenterologists, and radiologists.

First case: magnetic resonance cholangio-pancreatography showing dilated caudate lobe and left biliary system.
Second case
An 81-year-old man was referred to our unit after an incidental identification of an ICC during a follow-up investigation for bladder cancer. He had a transurethral resection of bladder tumor for a transitional cell carcinoma 4 years earlier and suffered from asthma and recurrent biliary colic.
A CT scan performed in 2007 for surveillance of his bladder cancer showed an atrophic left liver. This was conservatively managed due to the ambiguity of diagnosis, advanced patient age, and patient preference. A subsequent CT scan showed a slow growing mass, making this consistent with an ICC affecting the left hepatic ductal system (Fig. 2). An MRCP was performed showing dilatation of all of the left lateral segment ducts, and involvement of the left portal vein causing left lobe atrophy. Chest and abdominal imaging did not show any evidence of metastatic disease. A biopsy of the mass lesion was taken and confirmed the tumor as an ICC of papillary morphology. After discussion at our multidisciplinary team meeting, a laparoscopic left hemihepatectomy and caudate lobectomy appeared to be the most appropriate course of action.
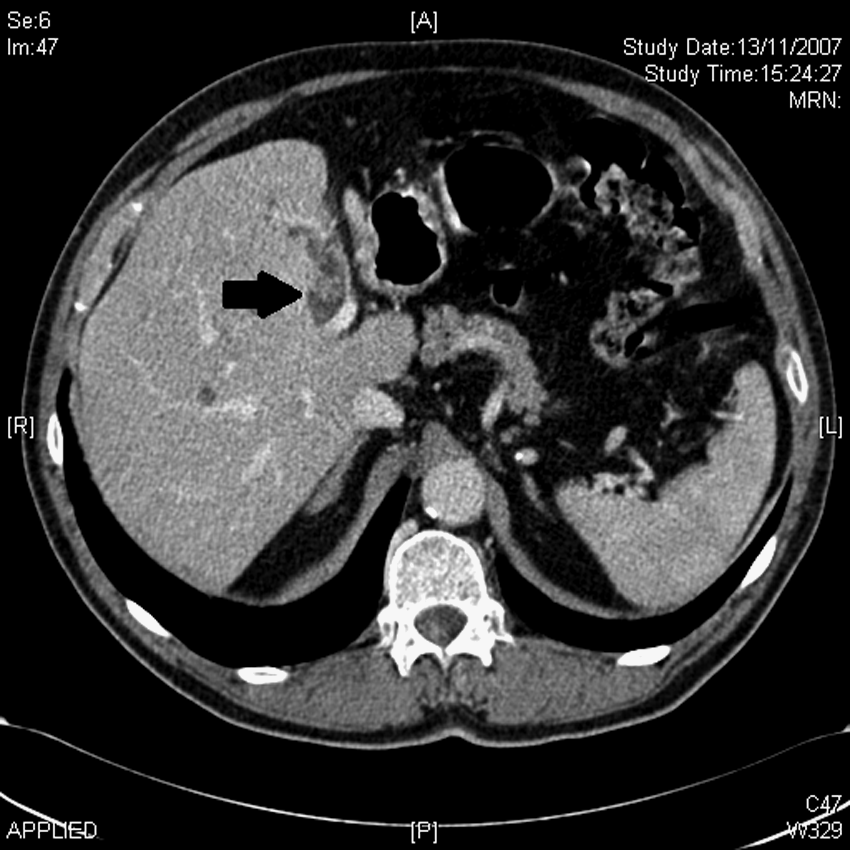
Second case: computer tomography showing ICC affecting the left hepatic ductal system (arrow) with left liver lobe atrophy.
Surgical Technique
The patient is placed in the supine position with the surgeon standing to the patient's left for the hilar dissection and then to the patient's right for the parenchymal dissection. Alternatively, the surgeon stands between the patient's legs for the whole procedure. Pneumoperitoneum is established by maintaining an intraperitoneal pressure of 12–14 mmHg and a differential pressure with the central venous pressure of 5–8 mmHg. Five ports are necessary in this procedure (Fig. 3).
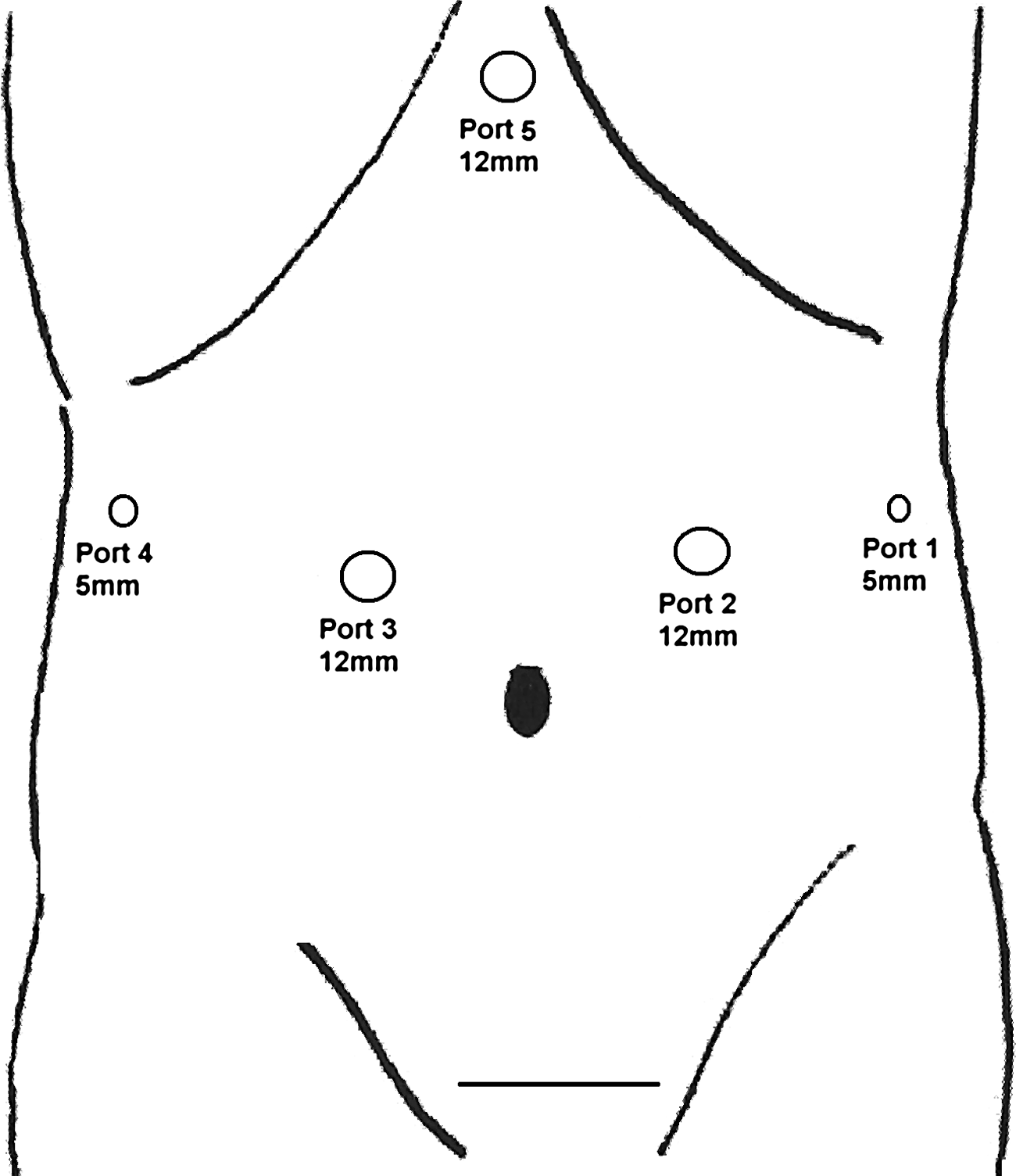
Five ports required for laparoscopic left hepatectomy.
Liver mobilization is performed by using Laparoscopic Operation by Torsional Ultrasound (LOTUS; S.R.A. Developments Ltd.), by first dividing the round and falciform ligaments back to the level of the hepatico-caval venous confluence. The triangular ligament is then divided, extending the line of dissection medially along the anterior border of the left coronary ligament, until the lateral border of the left hepatic vein is identified. The left lobe is then lifted, and the lesser omentum is opened to permit good vision of the caudate lobe.
The laparoscopic Pringle's maneuver is performed as described by our team elsewhere. 10
Inflow control is obtained extraparenchymally after exposing the portal structures by elevating the liver using the gallbladder and the round ligament as handles. The hepato-duodenal ligament dissection starts with a superficial transverse incision from left to right, 1–2 cm below the hilar plate (Arantius' ligament). The left hepatic artery is identified, slung, and dissected by using a diathermy hook, a nontraumatic grasper, and a specially designed laparoscopic 10 mm right angle Gemini dissecting forceps (Elmed). Once the arterial anatomy is clear, the left hepatic artery is ligated with three self-locking polymer Hem-o-lock clips (Weck Closure Systems) and divided. The division of the artery opens up the plane that allows direct vision of the left hepatic duct and portal vein. The left portal vein is dissected out, controlled with a sling, and divided between Hem-o-Lock clips or with an Endoscopic Articulating Linear Cutter such as ETS 45 mm (Ethicon Endo-Surgery). The left hepatic duct is then divided intrahepatically during the parenchymal transection.
The resection of the caudate lobe and the dissection of the left liver are carried out along side. After lifting the left lobe and pushing it to the right with the aid of a 10 mm articulating fan retractor, the inferior part of the caudate lobe is dissected away from the vena cava using LOTUS and metallic clips for vascular branches when encountered (Fig. 4). We then move to the left liver resection, which would enable a better exposure of the middle and posterior part of the caudate lobe. The parenchyma is initially dissected using LOTUS, starting on the upper liver surface from the front to the back, taking sequential layers of 2–3 mm depth down to the level of the middle hepatic vein. The line of the middle hepatic vein is identified on intraoperative ultrasound, and its relation to any tumor deposits is noted. The line of transection is then marked with diathermy scoring of the hepatic capsule to ensure dissection starting no more than 5 mm to the left of the line of the middle hepatic vein and providing adequate (minimum 10 mm margin in malignant disease) sonographic clearance of any segment 4 tumor deposits. When structures of >4 mm diameter are identified, they are secured with laparoscopic clips, placed away from the transection line to avoid subsequent inclusion into endovascular stapler lines. The dissection is continued in this way until large middle hepatic vein branches are encountered. At this stage, a two-handed technique is adopted by using the Cavitron Ultrasonic Surgical Aspirator (Valleylab) to skeletonise vascular structures in conjunction with LOTUS. This allows safe identification and control of larger vessels before dividing them. When the left hepatic vein confluence is revealed, the parenchyma is dissected to expose the superior and medial surfaces of the left hepatic vein over a 10 mm length of vein. The transection is then completed by using a single firing of an endovascular stapler to divide it and any remaining adjacent parenchyma, taking care to avoid traction injury to the middle hepatic vein and the cava.

The caudate lobe is dissected away from the vena cava by using metallic clips for vascular branches.
The specimen is removed in an impermeable bag (Endocatch, Ethicon Endo-Surgery) introduced through a 15 mm suprapubic port subsequently extended to a Pfannenstiel incision (∼6–7 cm).
Finally, the transection line is compressed with a clean gauze swab, and any bile leak is controlled with Prolene 4/0 stitches or with clips if a duct with pedicle is clearly identified. Hemostasis is obtained by using bipolar diathermy for small bleeding points and clips and Prolene sutures for any substantive bleeding. Hemostatic products such as fibrillar collagen and fibrin glue (Evicel, Johnson&Johnson Wound Management) are routinely used if oozing persists, particularly if near the middle hepatic vein. 11
The intraoperative results and postoperative course of our patients are summarized in Table 1.
Postoperative Outcome
First case
Four days postoperatively, the patient suffered chest pain. Electrocardiogram (ECG) showed multiple atrial and ventricular ectopic beats. This was treated with amiodarone and aggressive electrolyte therapy. The patient was discharged on postoperative day 8. Definitive histology of the specimen was consistent with a T1 ICC (25 mm maximal diameter) of intraductal growth type (20 mm free resection margin). Lymph nodes excised were negative for metastases. Twelve months after surgery, the patient was doing very well without signs of recurrence.
Second case
The patient had an episode of chest pain on postoperative day 1. Although this had been relieved with glyceryltrinitrate spray, no ECG changes or suspicious troponin level were detected. The patient was discharged on postoperative day 4.
Histological examination showed an invasive ICC (maximal diameter 49 mm) on a background of intraductal papillary mucinous neoplasm. Although the tumor was graded as a T1 adenocarcinoma of the bile duct, severe dysplastic changes were found throughout the left hepatic ductal system, extending up to the left hepatic duct margin (10 mm free resection margin).
Seven months after surgery, a CT of his chest, abdomen, and pelvis showed multiple low attenuation lesions consistent with cysts. No intrahepatic biliary dilatation was detected, although the common bile duct was slightly dilated. Destructive lesions of the left 10th rib and right iliac bone were observed, and both were associated with a low-density soft-tissue component. No mediastinal lymphadenopathy or lung nodules were demonstrated. The patient underwent an elective ultrasound scan guided biopsy of the left rib mass. No solid material was obtained, but 10 mL of fluid was aspirated and sent for cytology. Adenocarcinoma cells were identified among the blood-stained aspirate. The patient underwent palliative radiotherapy for rib and hip pain and died 4 months later (11 months after surgery).
Discussion
Our preliminary data showed that pure laparoscopic left hepatectomy and caudate lobe resection for ICC may be feasible, safe, and oncologically efficient when performed within a high-volume liver center with expertise in laparoscopic surgery. However, adequate patient selection is required. The patients described in our study had an early stage ICC, in both cases discovered incidentally during investigations or follow-up for urinary tract malignancies.
Laparoscopic pure left hepatectomy and caudate lobe resection for ICC has never been systematically described earlier. Cai et al. published the largest case series of 19 attempted laparoscopic left hepatectomies, of which 17 were successfully completed. Surgical indication was mainly for benign disease, including hepatolithiasis (n=17), and giant hemangioma (n=2). One patient operated for hepatolithiasis had incidental intraoperative finding of an ICC, which was laparoscopically resected with a 2-cm tumor-free margin. 12 Further reports of laparoscopic left hepatectomy mainly for benign disease have been reported, thus showing the feasibility and safety of this procedure for selected patients.13,14
We performed the first case of left hepatectomy and caudate lobe resection for ICC only after having gained experience with about 180 laparoscopic minor and major hepatectomies. Laparoscopic major hepatectomies may be extremely challenging, and major expertise in liver and laparoscopic technique is required. Surgeons should be ready to deal with major bleeding if it occurs as described by our group elsewhere, 11 and maintain a low threshold for conversions if the patient's safety is at risk.
In selected patients, the laparoscopic approach may favor an early safe discharge and prompt recovery. The latter is particularly suitable for elderly people who are commonly at a risk of prolonged postoperative recovery.`
Footnotes
Disclosure Statement
No competing financial interests exist.