
Abstract
Abstract
Objectives:
Essential hyperhidrosis (EH) is defined as excessive functioning of the sudomotor sweat system. Definitive treatment of choice is video-assisted thoracoscopic sympathetic interruption. Success rates are high, but compensatory hyperhidrosis (CH) remains a troublesome side effect. The aim of this study was to document patient satisfaction and side effects at least 6 months after thoracoscopic sympathicolysis.
Methods:
Between 2001 and 2005, 246 patients underwent bilateral ablation of the sympathetic chain at the thoracic level T2, T3, and/or T4. Questionnaires using open questions and scoring systems were sent at least 6 months after procedure and were returned by 138 patients (56%).
Results:
From the 138 patients (56 males/82 females), 39 suffered from cranial (±facial blushing), 34 from palmar, and 34 from axillary hyperhidrosis. Thirty-one patients were treated for a combination. No conversion to open surgery or deaths occurred. For the whole group, average quality of life was 4.5±2.5 before and 8.4±1.8 after surgery (P<.001). Ninety-one percent were very satisfied (score ≥7) and 80% showed an increased quality of life of ≥2. Compensatory sweating occurred in 76% of the patients, only 6% reported this as disabling. Comparing subgroups, a significant improvement in primary complaint score was found in 90%, 94%, and 91% for the T2, T3, and T4 patients, respectively. In the T4 group, the prevalence of CH was markedly lower (53%) and none of these patients were dissatisfied.
Conclusion:
Thoracoscopic ablation of the sympathetic chain is an effective treatment for EH; CH occurs in the majority of patients, but only rarely impairs postoperative quality of life.
Introduction
The first-line treatment of EH is often nonsurgical (e.g., topical antiperspirants, iontophoresis, and botulinum toxin injection), but the procedure of choice for definitive treatment is video-assisted thoracoscopic sympathetic interruption. The objective of this safe and minimally invasive method is to disconnect the sympathetic thoracic ganglia T2 (craniofacial EH with or without facial blushing), T3 (palmar EH), or T4 (axillary EH) by applying electrocoagulation, clipping, harmonic scalpel, or radiofrequency.3,4 It is an effective procedure with long-term anhidrosis achieved in 84–98% of the patients, hypohidrosis in 2.2–7%, and a failure rate range of 0.2–2%.5–7 Major postoperative complications such as injuries to great vessels, chylothorax, or brachial plexus lesions are extremely rare. 5 The most reported problems are postoperative pain or swelling, both of which usually resolve within 1 month after intervention. 2 Pneumothorax occurs frequently after surgery but the relatively small amounts of gas usually absorb without further treatment and only 0.4–2.3% require manual aspiration or chest tube drainage. 8
The most troublesome long-term adverse effect is compensatory hyperhidrosis (CH) which can affect the foot, trunk, face, buttocks, and popliteal fossa. Although CH prevalence as high as 86% has been reported,5,8–10 severe CH—perceived by the patient as disabling—only occurs in 1–8%.8,10 Also, this compensatory sweating has been attributed primarily to environmental temperature or physical activity, rather than to stress as is the case of EH. Besides the lack of exact criteria for defining CH, the heterogeneities of the surgical techniques used and of the levels disconnected make it difficult to appreciate the extent of CH reported in the literature. A review of the literature by Macia et al. 2 is not entirely conclusive but suggests that the probability of CH is independent of the technique used, and that less CH can be expected when destroying only one sympathetic ganglion or when performing surgery on the inferior ganglia (T3-T4).
In the present study, we aimed to document patient satisfaction, in terms of complaint scores including CH, but also quality of life, interviewed at least 6 months after having undergone thoracoscopic ablation of the sympathetic chain. We also examined these scores in subgroups of patients in whom only one ganglion had been ablated.
Patients and Methods
Between 2001 and 2005, 246 consecutive patients were treated for EH. Sequential bilateral procedures were performed at the T2, T3, or T4 level for craniofacial (±facial blushing), palmar, or axillary EH, respectively. All patients evaluated in this study were treated at the University Hospital of Brussels, operated by the same surgical team, using similar technical criteria. Briefly summarized, video-assisted thoracoscopy was performed under general anesthesia with the patient in a supine position with 90 degrees abduction of both upper limbs. Patients were intubated with a single-lumen tube, and underwent a sequential bilateral procedure with two incisions of 5 mm on each side. After establishing pneumothorax, the pleural space was inspected and the sympathetic chain identified. Ablation using monopolar electrocoagulation was the chosen technique in all the cases. 4 The procedure was performed as an outpatient intervention. Patients were discharged from the hospital several hours after the surgery after a clinical checkup and control of the chest X-ray.
At the end of the period under consideration—and at least 6 months after the procedure for the most recently treated patients—all patients above the age of 18 were asked to fill out a questionnaire. Permission from the local ethic committee had been obtained to prompt patients for filling out the questionnaire. Hundred and thirty eight of the 246 patients (56%) returned a correctly filled out questionnaire. Open questions were related to duration of symptoms, indication of the procedure, and prior treatments for EH (medication, iontophoresis, hypnosis, and behavioral training), as well as postoperative complications or side effects. The patient was also asked to score amongst others: impact on daily life, issues related to the procedure, to the hospital stay (1-day clinic), complications, and CH on other body parts after the procedure. All these issues were addressed in standard questions that required a response in terms of a score ranging 0 to 10 (0 being “not satisfied at all” to 10 being “entirely satisfied”). For any individual patient, the procedure was considered successful when the patient's overall quality of life score was 7 or more after the procedure; a dissatisfied patient was identified as reporting a quality of life score of 5 or less. Also, improvements in complaint scores were considered clinically meaningful when equaling (in absolute value) 2 or more. In particular, CH was assessed in two ways. First, CH was quantified by considering an increase in sweating score of ≥2 on any other body part than the body part corresponding to the primary indication. Then the patient was asked whether the reported compensatory sweating was also perceived as disabling.
We first assessed the outcome for the whole group (n=138), and then identified a group of 107 patients who required the ablation of only one ganglion, and repeated the analysis for three subgroups according to the level of sympathectomy (T2 only, T3 only, or T4 only).
Statistical analysis
Significant differences between pre- and postintervention scores were assessed using a Wilcoxon test. The proportion of patients in the three subgroups (T2, T3, and T4) was compared with the Chi-square test. Analysis of variance was performed to test for differences in values (e.g., of age) between the three groups. P<.05 was set as the level of significance.
Results
The results for the entire group are summarized as follows. The 138 patients (56 males/82 females) were 32±11 (standard deviation [SD]) years old, and had the intervention 18±13(SD) years after onset of hyperhidrosis. Of the 138 patients, 39 suffered primarily from cranial hyperhidrosis (with or without facial blushing), 34 primarily from palmar hyperhidrosis, and 34 primarily from axillary hyperhidrosis, and were treated by single T2, T3, or T4 ablation, respectively. The remaining 31 patients were treated by a combination of T2 and/or T3 and/or T4 ablation for a combination of the above indications. Of these 31 patients, 21 patients also mentioned other sweat locations or associated Raynaud's phenomenon. No conversion to open surgery was necessary and there was no operative mortality. No Horner's syndrome occurred. Eight patients required redo procedures; three of those were also unsuccessful on the second occasion (i.e., 2% failure rate).
Seventy-two out of 138 patients (52%) had already tried at least one method of conservative treatment in the years previous to the procedure. Local therapy with antiperspirants was attempted most often (40 patients), followed by iontophoresis (15 patients). Other techniques used by 2 patients or more included botulinum injection (8 patients), psychotherapy (8 patients), psychopharmaca (6 patients), acupuncture (5 patients), anticholinergics (4 patients), and hypnosis (3 patients). Twenty of the 138 patients had already tried more than one of the above methods.
For the whole group (n=138), general satisfaction scores related to information of the procedure, hospital stay, and waiting time were respectively 8.6(SD=1.5), 8.7(SD=1.4), and 7.9(SD=1.9); scores on whether they would recommend the procedure to others, or do it again themselves, were respectively 8.7(SD=2.8) and 8.9(SD=2.8). Average quality of life was 4.5±2.5(SD) before and 8.4±1.8(SD) after surgery (P<.001). Ninety-one percent of the patients were very satisfied (score ≥7), and 80% of the patients showed an increased quality of life of ≥2 points or more. Five patients (3.6%) could be labeled as dissatisfied (quality of life score <5). CH (any increase in sweating on other body parts even if not symptomatic) occurred in 76% of the patients, yet, only 6% of patients reported this as disabling. In 7% of the patients, the procedure resulted in palmar hypohidrosis. Other significant side effects affecting 2 patients or more were scars (5 patients), persistent dyspnea during exercise (5 patients), and feeling cold (2 patients).
The above-mentioned quality of life score obtained in the entire group, with an average increase of almost 4 points on a scale of 10, is compared with those obtained in the thoracic level T2, T3, and T4 subgroups in Figure 1, showing very similar and consistent increases in quality of life. Improvements (increases) in the quality of life scores were more or less mirrored by improvements (decreases) in complaint scores on the primary indication in each subgroup (Fig. 2). Also, when expressing a clinically meaningful improvement as a decrease in complaint score of ≥2, this was found to be the case in 90%, 94%, and 91% of the T2, T3, and T4 group patients, respectively (Table 1). Table 1 also details the compensatory effects, showing a markedly lower prevalence of CH in the T4 group (53%) with none of these patients reporting CH as disabling at all. It is noteworthy that this group of patients presenting to our clinic for axillary hyperhidrosis had waited for approximately 10 years before deciding to have the intervention; in the two other subgroups, this decision period was twice as long. Also, in the T4 group, no patients were dissatisfied with the intervention.
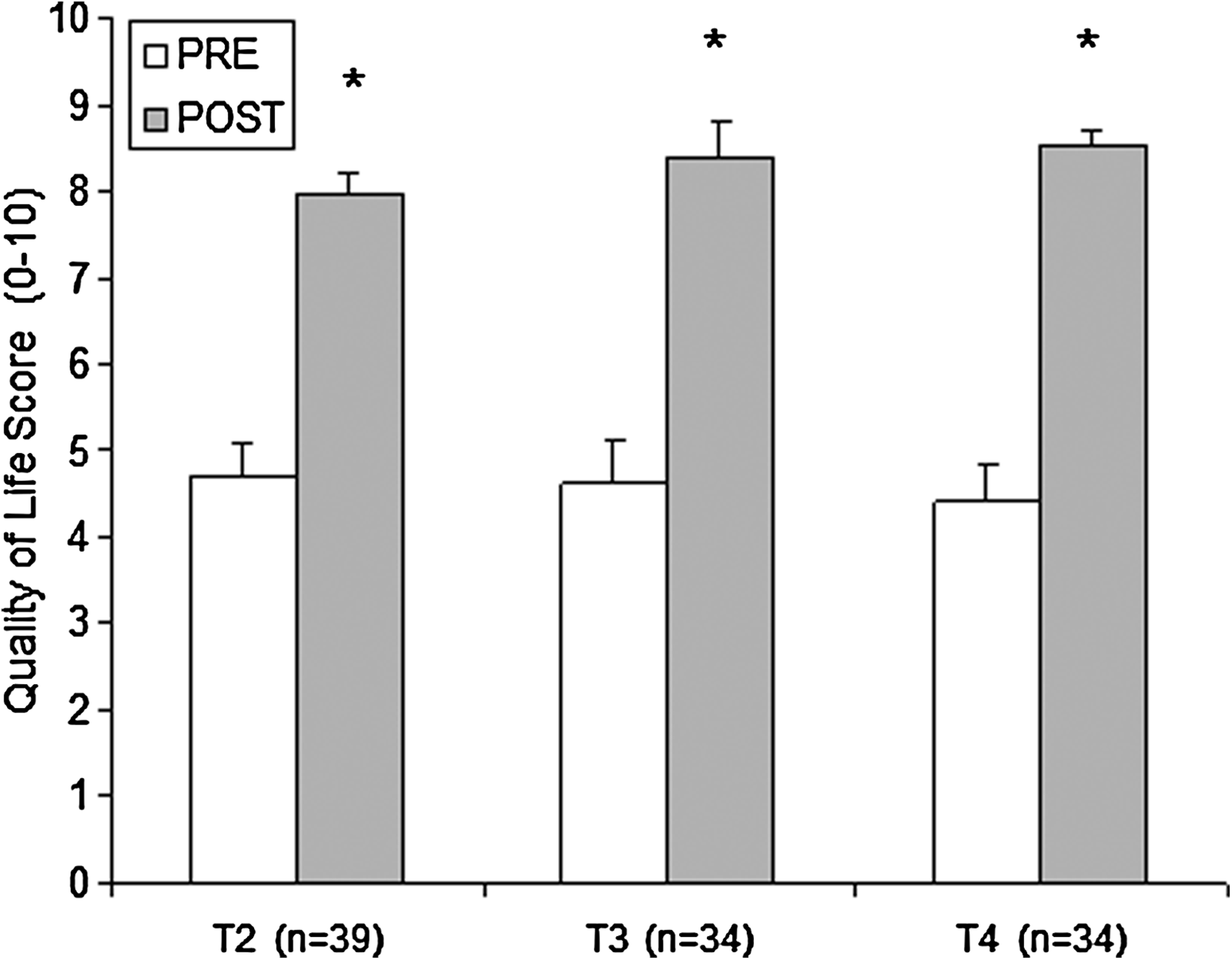
The figure shows the difference in quality of life score before and after the procedure. Unfilled bars represent the scores before the procedure, filled bars after the procedure. Asterisks indicate significant difference pre- versus postintervention (P<.001 for all).
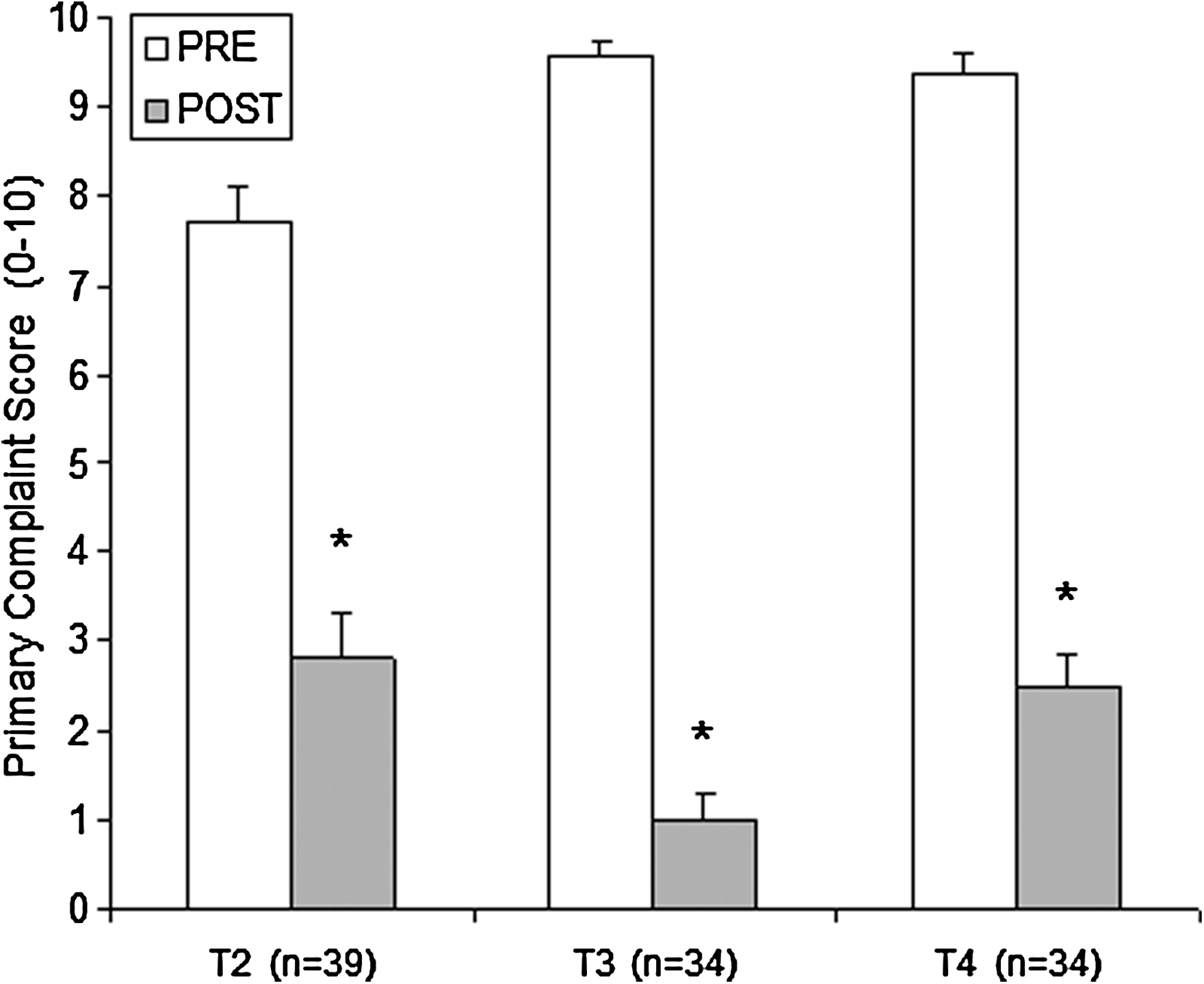
The figure shows the difference in primary complaint score before (unfilled bars) and after (filled bars) the procedure.
P values indicate an overall difference in value (analysis of variance) or in proportion (Chi-square test).
The superscripts indicate a significant difference in value or proportion versus other groups.
Discussion
The therapeutic options for the management of EH have traditionally been nonoperative. These include topical antiperspirants, anticholinergic drugs, iontophoresis, and botulinum injections. These methods are seldom sufficient and they only provide transient relief. Thoracoscopic interruption of the sympathetic chain is a safe and effective method for treating patients with EH, resulting in significant improvements in quality of life.3,4 The degree of postoperative patient satisfaction is directly related to the improvement of the primary symptoms and development of CH. Across all previous reports including various combinations of T2, T3, and T4 intervention, long-term anhidrosis is achieved in over 85% of the patients, and despite high rates of compensatory sweating (up to 86%), prevalence of disabling CH does not exceed 8%. Palmar hypohidrosis is never more than 7% and failure rate is 5% or less. Our results obtained for the entire patient group are very similar: 91% were very satisfied, prevalence of compensatory sweating was 76%, and disabling CH amounted to 6%; the procedure resulted in palmar hypohidrosis in 7% of our patients and failure rate was 2%.
Thus far, the most satisfactory results have been reported for palmar and axillary EH interventions, followed by craniofacial EH. For instance, Jeganathan et al. 7 report success rates of 98% and 96% of patients with palmar and axillary EH, respectively, and in only 84% in those patients with facial EH. Our study very clearly shows that such an outcome critically depends on how exactly patient satisfaction is assessed (Table 1). When we consider quality of life score, we obtain a very similar picture: over 90% of patients with palmar and axillary EH are very satisfied, compared with only 82% of patients with facial EH. However, when the improvement in primary symptom score is considered, very similar and high satisfaction rates (over 90%) are obtained in all three groups. The reason for this apparent discrepancy can be found when examining the CH scores (whether disabling or not). The higher prevalence of compensatory sweating in the T2 versus T3 and T4 groups is in fact the most likely reason why quality of life is scored somewhat less by the T2 group, despite a similarly high success rate in terms of the primary indication for the intervention. It has been suggested that lower success rates for facial hyperhidrosis/blushing could be due to a greater awareness of the risk for Horner's syndrome when performing high T2 ablation. Indeed, during T2 intervention, heat transmission or traction 11 can totally or partially damage the stellate ganglion (T1), which can lead to Horner's syndrome (with or without miosis). The awareness of risk factors associated with the T2 intervention could lead to an incomplete ablation of sympathic activity and hence a lesser improvement of the primary symptom scores for T2 than for T3 or T4. This appeared not to be the case in our center (Table 1).
The most frequently mentioned and feared complication is CH affecting the back, abdomen, and anterior thorax.5,8,9 Review of the literature reveals controversial findings on CH with reports of prevalence up to 86%,8,10 also specifying these as “minor” in 61%, “embarrassing” in 31.5%, and “disabling” in 7.5%.8,10 Possibly, the volatility of these terms to actually grade CH is the likely reason for the existing variability in reported prevalence of CH. In our center, we found a relatively low prevalence of persistent disabling CH (5.3% in the whole group; 10%, 3%, and 0% for T2, T3, and T4, respectively), despite a significant increase in sweating in other body parts (in 90%, 79%, and 53% of the patients in T2, T3, and T4 groups, respectively). The relatively lower CH in T3 and T4 groups obtained here are in fact comparable to those obtained by Liu et al., 12 reporting 77% and 56%, respectively. The lowest degree of CH and absence of any disabling CH in T4 group deserves particular attention, and could provide a clue as to the conditions that protect a patient from developing compensatory sweating. Several other authors have also already described lower percentages of CH if surgery is performed on the inferior ganglia.2,13,14
We recognize the limitation that our data originate from a relatively small sample of patients (56% return of the questionnaire) and were collected retrospectively. Further, the volatility of the terms to grade satisfaction and side effects as CH makes the results difficult to compare with other studies.
In summary, based on all the aforementioned results about quality of life and degree of satisfaction, thoracoscopic ablation of the sympathetic chain can be considered a safe and effective procedure for EH. Postoperative CH is frequent, but rarely cumbersome and has little or no effect on improvement in quality of life.
Footnotes
Disclosure Statement
No competing financial interests exist.