
Abstract
Abstract
Background:
Common bile duct stones are a frequent complication of gallstones. Endoscopic retrograde cholangiopancreatography and sphincterotomy are often performed to evaluate the etiology of obstructive jaundice and for concomitant therapeutic removal of common bile duct stones. We aimed to evaluate the recurrence rate of cholangitis or cholecystitis after endoscopic lithotripsy with gallstones in situ and to identify associated predictive factors.
Patients and Methods:
We retrospectively reviewed 183 patients who had received endoscopic lithotripsy between July 2007 and June 2010. We divided patients into two groups: One group who had received subsequent cholecystectomy (n=66) and one observational group (n=117). Patients with previous cholecystectomy or without gallstones were excluded. All included patients were followed up at our outpatient department. Our end point was the presence of symptoms of recurrent cholangitis or cholecystitis.
Results:
Subjects included 86 males and 97 females with a mean age of 62.5±16.3 years (range, 43–81 years). Cholangitis or cholecystitis recurred in 6 patients in the cholecystectomy group and 30 patients in the observational group. Findings revealed a lower recurrence rate and longer recurrence-free period in patients who received subsequent cholecystectomy. The recurrence rate of the observational group was significantly higher than that of the cholecystectomy group (25.6% versus 9.1%, P=.007). Univariate and multivariate Cox regression analyses revealed that common bile duct dilatation was an independent predictive factor for recurrence.
Conclusions:
Cholecystectomy is recommended after endoscopic lithotripsy. Common bile duct dilatation is associated with the rate of recurrent cholangitis or cholecystitis.
Introduction
Subsequent laparoscopic cholecystectomy (LC) is often recommended for patients who have gallbladder stones in situ after ERCP/ES. The rationale for cholecystectomy in patients with gallstones is to prevent biliary complications such as acute cholecystitis, biliary colic, recurrent biliary stones, cholangitis, and biliary pancreatitis. However, in our experience, many patients, especially elderly individuals, hesitate to receive the surgery because of perceived higher risk for aged patients or because concomitant chronic illness may make them poor surgical candidates. Some studies have evaluated routine LC in the extreme elderly 1 and the necessity and safety of cholecystectomy in high-risk candidates after CBD stone removal by ERCP. 5 Byrne et al. 5 reported that half of subjects had elective cholecystectomy and among that those choosing the wait-and-see approach, 20% developed complications. In the study by Costi et al., 1 the wait-and-see policy helped patients older than 80 years of age avoid LC, but biliary-related events developed in half of the patients, necessitating delayed surgery in some cases, with poorer outcomes. A Chinese study concluded that LC after endoscopic treatment of bile duct stones reduces recurrent biliary events and should be recommended. 6
Recurrence of cholangitis or cholecystitis after ERCP with removal of CBD stones, with and without cholecystectomy, has not been explored, and predictive factors for recurrence remain unclear. Given that our subjects had all undergone ERCP/endoscopic lithotripsy for removal of CBD stones, it seemed prudent to evaluate the effects of subsequent LC on recurrence. We hypothesized that if we could know the recurrence rate and predictive factors of recurrent cholangitis after patients receive ERCP/ES to remove CBD stones with gallstones in situ, then we could more effectively determine which patients may benefit from undergoing subsequent cholecystectomy. Understanding who might benefit would be of potential significance to clinicians faced with the decision of LC or no LC after clearance of CBD stones.
The aim of this retrospective study was to evaluate the recurrence rate of cholangitis after ERCP/ES removal of CBD stones with gallstones in situ and to identify predictive factors of recurrent cholangitis or cholecystitis after CBD stone removal.
Patients and Methods
The protocol for this retrospective study was approved by the Internal Review Board of Mackay Memorial Hospital, Taipei, Taiwan.
Patients
We retrospectively reviewed patients of Mackay Memorial Hospital who had undergone successful ERCP/ES and extraction of CBD stones between July 2007 and June 2010. All patients who had received ERCP for removal of CBD stones and whose ultrasound studies revealed in situ stones in the gallbladder were eligible for the study. We excluded patients who had received previous cholecystectomy or endoscopic lithotripsy for biliary pancreatitis and those who had no gallstones. In total, 325 patients who had received endoscopic sphincterotomy were initially screened. Of these, 101 patients who had received prior LC and 41 who had received ES due to biliary pancreatitis were excluded. The data of the remaining 183 patients were finally analyzed.
Methods
Patients' personal and clinical demographics were recorded, including age, gender, prior surgeries, blood sugar, liver function tests, renal function tests, serum lipid, blood culture results, and history of diabetes mellitus, hypertension, renal disease, and liver disease. All patients had received ES in our institution to remove CBD stones; we used a four-wire dormina basket or/and balloon retriever, and in all cases subsequent cholangiography had revealed no residual filling defect in the CBD. The dates of ERCP/ES, recurrent cholangitis or cholecystitis, and cholecystectomy were recorded. After the high probability of complications such as cholecystitis or cholangitis in those with CBD stones was explained to the patients, some older patients decided against having surgery because of personal issues such as advanced age, reactions to medications, possible complications, or the desire to return home until their health improved. Therefore, patients were divided into two groups based on whether or not they had accepted subsequent cholecystectomy after ES (ES+LC group) or whether surgery would be deferred and they would be observed further (ES-only group). All patients were followed up at our outpatient department, and our end point was the presence of recurrent symptoms of cholangitis or cholecystitis.
Statistical analysis
Statistical analyses were performed using SPSS version 18.0 statistics software (SPSS Inc., Chicago, IL). Continuous data were presented as mean±standard deviation values, and categorical data were presented as n (%) for a given group. Differences between groups were compared using the Mann–Whitney U test for continuous data due to abnormal distribution, whereas Pearson chi-squared test or Fisher's exact test was used for categorical data. Univariate and multivariate Cox regression model analyses were performed to identify the prognostic factors that might be associated with recurrence. Univariate Cox regression model analysis was applied to variables with a P value of <.2 from comparison between the subsequent cholecystectomy group and observational group. Multivariate Cox regression model analysis was then applied to variables with a P value of <.2 after the univariate Cox regression model analysis. The Kaplan–Meier curve with Log-rank test was performed to identify the cumulative recurrence rate between groups. A P value of <.05 was considered to be statistically significant.
Results
In total, 183 patients were included in this study. Figure 1 shows patients' disposition. Among the 183 patients, 116 patients were in a cholecystectomy group (ERCP+LC group), and the other 67 patients were in an observational group (ES-only group). In the cholecystectomy group, 6 patients had experienced recurrence. In the observational group, 30 patients experienced recurrence.

Flow chart of patients' disposition. ES, endoscopic sphincterotomy.
Table 1 presents the comparison of patient demographics and clinical characteristics between the cholecystectomy and observational groups. Overall, the average age was 62.5 years (SD=16.3). Among 183 patients, 86 patients were males (47%). Furthermore, the recurrence rate was significantly higher in the observational group compared with the cholecystectomy group (25.6% versus 9.1%, P=.007): In the observational group, 14 patients had recurrent cholangitis, and 16 had recurrent cholecystitis; in contrast, in the cholecystectomy group, 6 patients had recurrent cholangitis (Table 1).
Continuous data are represented as mean±SD values and categorical data as n (%) for a given group.
Differences between groups were compared using the Mann–Whitney U test for continuous data due to abnormal distribution. Pearson chi-squared test or Fisher's exact test was used to analyze categorical data.
P<.05 indicates statistically significant difference between groups.
ALT, alanine aminotransferase; ALP, alkaline phosphatase; AST, aspartate aminotransferase; WBC, white blood cells.
Table 2 shows the results of univariate and multivariate Cox regression model analyses of patients, which identify the prognostic factors that might be associated with recurrence. Variables with a P value of <.2 from comparison between the cholecystectomy and observational groups were selected for univariate Cox regression model analysis. Multivariate Cox regression was then applied to variables with a P value of <0.2 from the univariate Cox regression model analysis. The univariate Cox regression model analysis shows that patients receiving cholecystectomy or having positive results in CBD dilatation might be associated with recurrence. Groups, age, and CBD dilatation results were further analyzed by the multivariate Cox regression model analysis to explore their association with recurrence. Results show that the patients who were in the cholecystectomy group and had positive results in CBD dilatation might be at lower risk for recurrence after ERCP: Cholecystectomy group versus observational group, hazard ratio (95% confidence interval)=0.612 (0.390–0.958), P=.032; CBD dilatation, hazard ratio (95% confidence interval)=0.401 (0.206–0.781), P=.007 (Table 2).
Results of Cox regression mode analyses are represented as hazard ratio (HR) (95% confidence interval [CI]) and the respective P value.
Variables with a P value<.2 from the univariate Cox regression model analysis were then analyzed with the multivariate Cox regression model.
P<.05 indicates statistically significant difference between the two groups (laparoscopic cholecystectomy after ES group versus observational [wait-and-see] group).
Figure 2 presents results of the Kaplan–Meier curve of recurrence with Log-rank test between the cholecystectomy and observational groups. The mean times to recurrence were 18.7 months (95% confidence interval, 16.5–20.9 months) and 20.7 months (95% confidence interval, 18.3–23.1 months) for the observational group and the cholecystectomy group, respectively. In the cholecystectomy group, the respective cumulative recurrence rates at 3 months, 6 months, and 9 months after operation were 2%, 6.6%, and 9.8%. In the observational group, the respective cumulative recurrence rates at 3 months, 6 months, and 9 months after operation were 13.4%, 19%, and 20.5%. The Log-rank test revealed that the cumulative recurrence rate was significantly lower in the subsequent cholecystectomy group compared with the observational group (P=.033).
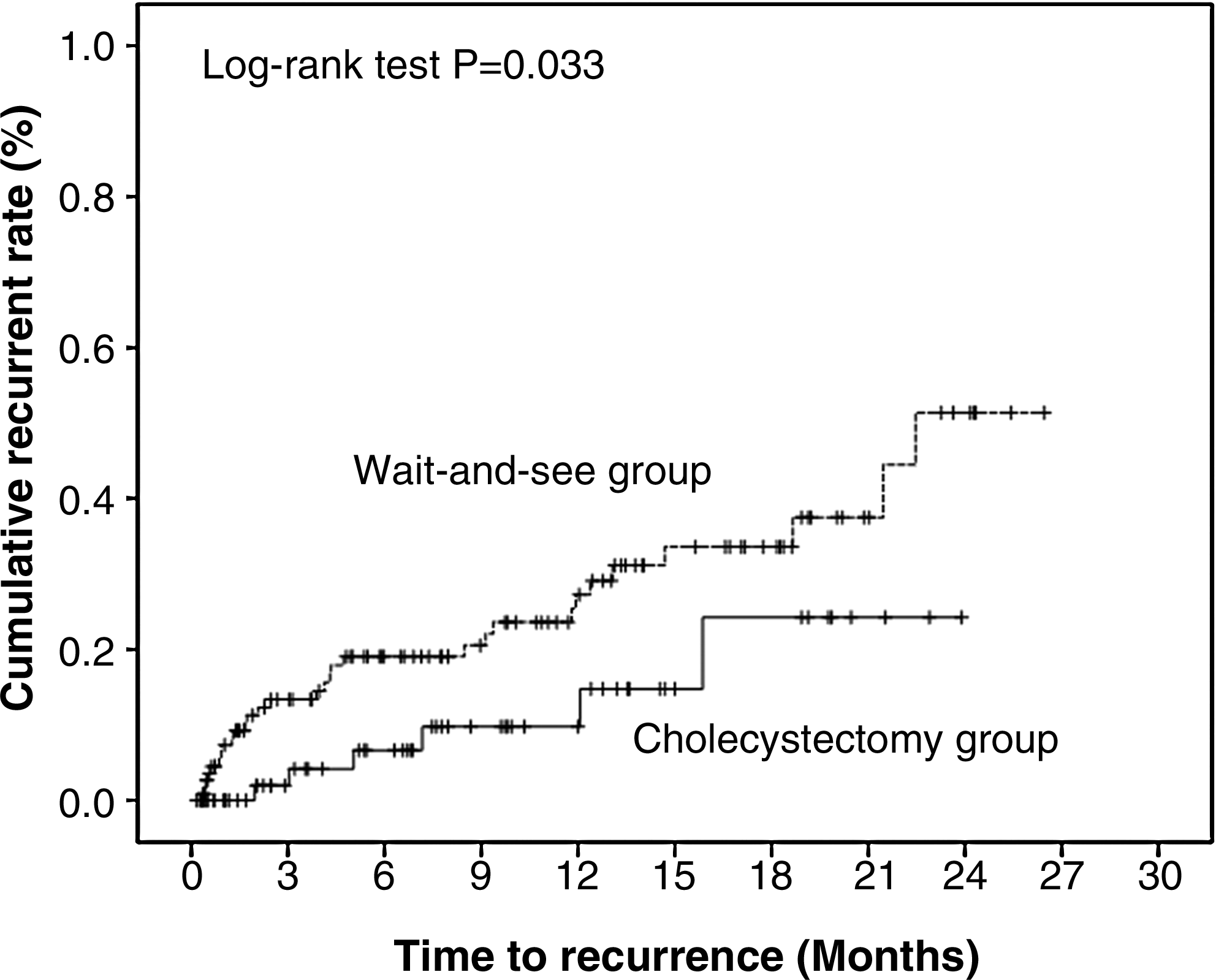
Kaplan–Meier curve of recurrence with Log-rank test by group. The solid line indicates the laparoscopic cholecystectomy after ES group, and the dotted line indicates the ES-only (wait-and-see) group. Recurrence is shown as +. Log-rank P=.033 indicates a significant difference in cumulative recurrence rate between groups.
Discussion
Our main findings revealed that patients who received subsequent cholecystectomy after CBD stone extraction had a lower recurrence rate and longer recurrence-free period compared with patients who had elected to be observed further. The recurrence rate of the observational group was significantly higher than that of the group receiving cholecystectomy (25.6% versus 9.1%, P=.007) During the mean follow-up period (256.4 days [ranging from 0 to 794 days] or 8.5 months [ranging from 0 to 26.5 months]), cholecystitis occurred in approximately 8% of patients in both groups. The incidence of recurrent cholangitis during follow-up was about 11%, and about 26% of the observational group patients developed at least one recurrent biliary event after sphincterotomy during follow-up, compared with 9% of patients who had undergone subsequent laparoscopic cholecystectomy. Boerma et al. 3 evaluated whether a wait-and-see policy was justified after successful sphincterotomy to remove CBD stones and concluded it could not be recommended routinely because 47% of expectantly managed patients developed recurrent symptoms and 37% of these patients actually needed cholecystectomy.
Recurrence rates in the present study are comparable to those of previous studies.3,4,7 However, other studies reported recurrent biliary events and higher morbidity, whereas in our study, complications were limited to cholangitis or cholecystitis. For example, Schreurs et al. 7 reported that 16% (27/164) of wait-and-see patients developed recurrence compared with 7.6% of patients receiving LC; patients returned with CBD stones, cholangitis, stenosis of Vater's papilla, cholecystitis, and symptomatic cholecystolithiasis. In another study, 47% of wait-and-see patients had recurrent biliary events after ES compared with only 1 of 49 patients (2%) in the group that received LC; morbidity was 32% versus 14%, and the hospital stay was 9 versus 7 days, respectively. 3 In a study of Chinese patients, 4 recurrence rates were 24% (21/89) for wait-and-see patients and 9.8% (8/82) for those undergoing cholecystectomy.
In our study, univariate and multivariate Cox regression analyses revealed that CBD dilatation was an independent predictive factor for recurrence. Therefore, we suggest that if patients have CBD dilatation, they are more in need of prophylactic cholecystectomy. Risk factors for development of biliary-related events after sphincterotomy with the gallbladder in situ have been sought to help in the selection of patients for prophylactic cholecystectomy. 8 Other possible risk factors have been reported, including diabetes, juxtapapillary diverticulum, and cholangitis at time of sphincterotomy. 9 An evaluation of risk factors for recurrent bile duct stones after endoscopic papillotomy concluded that gallbladder status, lithotripsy, and pneumobilia were significantly related to recurrence. 10 Fujimoto et al. 11 found pneumobilia to be the only significant risk factor for recurrence in their population. Given the risks and the rates of recurrence and considering the question of whether or not to recommend cholecystectomy as standard after successful removal of CBD stones, our study of a small population in a single institution points to routine LC and reserves the observational approach for older patients who may have concomitant illness or are otherwise not ideal surgical candidates. The safety and effectiveness of sphincterotomy have been documented by multiple studies and long-term follow-up,1–4,9,12,13 but whether routine cholecystectomy should follow is still being debated. Kageoka et al. 12 suggested that cholecystectomy after ES should be recommended for patients with calculous gallbladder but not for patients with acalculous gallbladder; they also found that pneumobilia was associated with recurrence. A recent randomized trial by Reinders et al. 14 investigated the timing of LC after ES and found that recurrent biliary events occurred in 36.2% of patients whose LC was delayed for 6–8 weeks; they concluded that LC within 32 hours—early LC—might prevent most biliary events and appeared to be safe after sphincterotomy. Archibald et al. 8 postulated which patients with relative contraindications would still be candidates for prophylactic cholecystectomy versus deferred cholecystectomy: Prophylactic cholecystecomy was advised for patients with gallstones in situ after ES, cholecystectomy if there was a history of pancreatitis, and deferral if more than 6 months had passed since ES was performed. Patients who deferred cholecystectomy were considerably older (mean age, 66.4 versus 49.8 years), which is similar to our thinking on the issue of age and wait-and-see policy. Generally, if deferring cholecystectomy does not risk survival or quality of life, the choice seems to depend on the incidence of recurrent symptoms. Kwon et al. 15 recommended restricting cholecystectomy to patients with symptoms from gallbladder stones and that indefinite postponement of cholecystectomy may be warranted in patients with gallstones in situ, for whom endoscopic treatment might be sufficient. Schreurs et al. 7 concluded that if CBD stones can be treated successfully with sphincterotomy and patients remain symptom-free, there is no need for routine cholecystectomy. Our results suggest otherwise given the lower recurrence rate and longer recurrence-free period of patients who received subsequent cholecystectomy after successful CBD stone extraction compared with those who adopted a wait-and-see policy.
This study has limitations, including the relatively small sample size and that data were only collected in one institution. A larger prospective study is needed to corroborate findings of the present study, especially with regard to age-related differences in recurrence rates and predictive factors for recurrence of cholangitis or cholecystitis after CBD stone removal with gallstones in situ.
In conclusion, based on our findings, we recommend routine laparoscopic cholecystectomy after endoscopic lithotripsy for the majority of patients. CBD dilatation is associated with an increased rate of recurrent cholangitis or cholecystitis.
Footnotes
Disclosure Statement
No competing financial interests exist.