
Abstract
Abstract
Objective:
Strategic laparoscopic surgery for improved cosmesis (SLIC) is a less invasive surgical approach than conventional laparoscopic surgery. The aim of this study was to examine the feasibility and safety of SLIC for general and bariatric surgical operations. Additionally, we compared the outcomes of laparoscopic sleeve gastrectomy with those performed by the SLIC technique.
Subjects and Methods:
In an academic medical center, from April 2008 to December 2010, 127 patients underwent SLIC procedures: 38 SLIC cholecystectomy, 56 SLIC gastric banding, 26 SLIC sleeve gastrectomy, 1 SLIC gastrojejunostomy, and 6 SLIC appendectomy. SLIC sleeve gastrectomy was initially performed through a single 4.0-cm supraumbilical incision with extraction of the gastric specimen through the same incision. The technique evolved to laparoscopic incisions that were all placed within the umbilicus and suprapubic region.
Results:
There were no 30-day or in-hospital mortalities or 30-day re-admissions or re-operations. For SLIC cholecystectomy, gastric banding, appendectomy, and gastrojejunostomy, conversion to conventional laparoscopy occurred in 5.3%, 5.4%, 0%, and 0%, respectively; there were no major or minor postoperative complications. For SLIC sleeve gastrectomy, there were no significant differences in mean operative time and length of hospital stay compared with laparoscopic sleeve gastrectomy; 1 (3.8%) of 26 SLIC patients required conversion to five-port laparoscopy. There were no major complications. Minor complications occurred in 7.7% in the SLIC sleeve group versus 8.3% in the laparoscopic sleeve group.
Conclusions:
SLIC in general and bariatric operations is technically feasible, safe, and associated with a low rate of conversion to conventional laparoscopy. Compared with laparoscopic sleeve gastrectomy, SLIC sleeve gastrectomy can be performed without a prolonged operative time with comparable perioperative outcomes.
Introduction
Subjects and Methods
One hundred twenty-seven adult patients underwent SLIC general and bariatric operations between April 2008 and December 2010. Our operative experience for SLIC started with cholecystectomy and appendectomy and was later applied to sleeve gastrectomy and gastric banding. Exclusion criteria for the SLIC approach to cholecystectomy included patients with large ventral hernia defect, history of prior upper abdominal midline operations, and body mass index (BMI) of >40 kg/m2. Exclusion criteria for SLIC appendectomy included perforated and retrocecal appendicitis. Exclusion criteria for the SLIC approach to bariatric surgery included patients with prior gastric or obesity surgery, large ventral hernia defect, history of prior upper abdominal midline operations, and BMI of >50 kg/m2. Data were collected on a computerized data form, including the following parameters: age, sex, preoperative BMI, operative time, length of hospital stay, intra- and postoperative complications, 30-day re-admission, 30-day re-operation, and 30-day and in-hospital mortality. For SLIC sleeve gastrectomy, the data were compared with those from a cohort of patients who underwent conventional laparoscopic sleeve gastrectomy prior to initiation of our SLIC program. A comparison was performed between the two groups with respect to demographic data, operative outcomes, morbidity, and mortality. This retrospective study was approved by the University of California Irvine Medical Center Institutional Review Board.
SLIC cholecystectomy
Patients were placed in a supine position. Both the operative surgeon and assistant stood on the patient's left side. Three laparoscopic incisions were made along the verge of the umbilicus (Fig. 1). Pneumoperitoneum was initiated using a Veress needle, and three trocars were placed (two 5-mm ports and one 12-mm port). A flexible-tip 5-mm camera (Olympus Surgical & Industrial America Inc., New York, NY) was placed for visualization. Additionally, a 2-mm rigid grasper was placed in the right upper quadrant and used to provide cephalad retraction of the gallbladder. A rigid grasping instrument was used for lateral retraction of the infundibulum of the gallbladder, and a flexible-tip dissecting instrument was used to identify the critical structures within the triangle of Calot. A cholangiogram was only performed selectively. In cases requiring cholangiography, conversion from SLIC to conventional laparoscopic cholecystectomy was performed. A critical view of safety was obtained prior to ligation and division of the cystic duct and artery. Once the cystic duct and artery were clearly delineated as the only two structures entering the gallbladder, they were clipped proximally and distally with a rigid multiclip applier. A rigid scissor was used to divide these two structures between the clips. The ultrasonic scalpel was used to remove the gallbladder from the liver bed. The gallbladder was placed into a bag and removed through the 12-mm trocar incision. The 12-mm fascial defect was closed with interrupted sutures.
SLIC appendectomy
Indications for appendectomy were appendicitis (n=3) and appendix adenoma (n=3). Three laparoscopic incisions were made within the skin verge of the umbilicus. Through these incisions, pneumoperitoneum was established, and three trocars (two 5-mm and one 12-mm) were placed. A flexible-tip 5-mm camera was placed for visualization. A standard laparoscopic grasper was used to retract the appendix, and a standard rigid dissector was used to dissect out the appendiceal vessels and appendix. An ultrasonic scalpel was used to mobilize the lateral attachment of the appendix and cecum. The mesentery of the appendix was divided using the ultrasonic scalpel. The appendix was then divided using a 45-mm linear stapler. The appendix was placed into a specimen bag and removed through the 12-mm trocar incision. Upon removal of the specimen, the 12-mm fascial defect was closed with an interrupted suture.
SLIC gastrojejunostomy
Three laparoscopic trocars were placed within the umbilicus (two low-profile 5-mm trocars and one 12-mm trocar). A flexible-tip 5-mm camera was inserted through a 5-mm port for visualization. Using two rigid graspers, the ligament of Treitz was identified, and a loop of proximal jejunum, 40 cm distal to the ligament of Treitz, was used for construction of the gastrojejunal anastomosis. Multiple (four) stay sutures were placed between the jejunum and the anterior aspect of the gastric wall. A gastrotomy and enterotomy were performed using an ultrasonic scalpel. The gastrojejunal anastomosis was then constructed using a 60-mm linear stapler with a 3.5-mm cartridge. The remaining common gastrotomy/enterotomy was closed with a running suture in two layers using the Endo Stitch™ (Covidien, Mansfield, MA) device. The anastomosis was tested with intraoperative endoscopy and showed no air leak. The abdominal 12-mm fascial defect was closed with an interrupted suture.
SLIC gastric banding
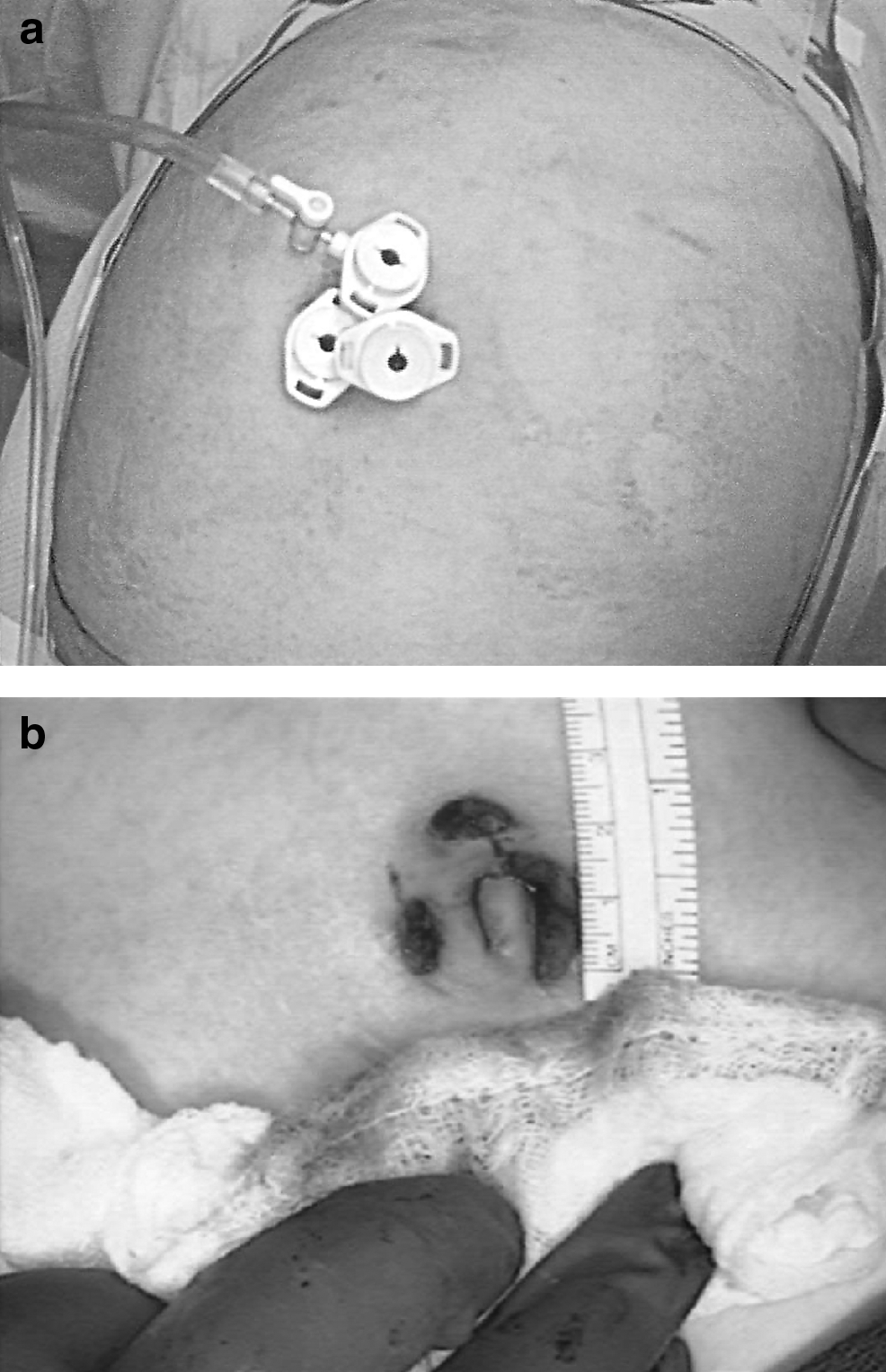
A single 3.5-cm incision was made in the midline between the xiphoid process and the umbilicus to accommodate implantation of the subcutaneous access port. Additionally, two 5-mm ports were placed at the umbilicus for visualization using the flexible-tip camera. Through the 3.5-cm incision, a 5-mm port was placed to accommodate the flexible liver retractor instrument, and a 15-mm trocar was also placed. The adjustable gastric band was inserted into the peritoneal cavity through the 15-mm trocar. The “pars flaccida” technique for placement of the gastric band was performed. The retroesophageal space was developed, and a flexible right-angle instrument was passed through this space to exit anteriorly through the angle of His. The suture attached to the adjustable gastric band was placed onto the right-angle instrument and then pulled through the retroesophageal space, wrapping the band around the proximal gastric cardia. The gastric band was then manually closed. Two or three gastrogastric sutures were placed anterior to the band, and a single medial, gastrogastric suture was placed below the band along the lesser curvature. All laparoscopic suturing was performed using the Endo Stitch device, and extracorporeal knot tying was performed with the Ti-knot® device (LSI Solutions, Victor, NY). The catheter from the band was exteriorized through the surgical incision and attached to the subcutaneous access port. The subcutaneous access port was positioned within the epigastric incision and secured to the rectus fascia using transabdominal suturing (Fig. 2).

Postoperative abdominal view of strategic laparoscopic surgery for improved cosmesis gastric banding with a single visible incision in the epigastric region for implantation of the subcutaneous port. All other laparoscopic incisions are hidden within the umbilicus.
Conventional laparoscopic versus SLIC sleeve gastrectomy
For SLIC sleeve gastrectomy, three laparoscopic trocars were placed within the umbilicus through three separate incisions, all contained within the umbilical verge, and a 5-mm trocar was placed in the right subcostal region (Fig. 3). Occasionally another 5-mm trocar was placed within the suprapubic region for additional retraction. Using a rigid grasper for retraction, the gastrocolic ligament was divided with bipolar cautery beginning 5 cm proximal to the pylorus. The greater curvature of the stomach was mobilized by dividing all short gastric vessels up to the angle of His. A liver retractor was not used in most cases. When needed, a conventional laparoscopic instrument was used to temporarily retract the liver. A 32-French bougie was placed transorally and positioned along the lesser curvature of the stomach. Multiple applications of the 60-mm linear stapler with staple-line reinforcement were used to construct the sleeve gastrectomy. When completed, the sleeve gastrectomy extended from 5 cm proximal to the pylorus to the angle of His. The 12-mm trocar site was enlarged, and the specimen was removed through this incision. Upon removal of the specimen, the fascial defect was closed with an interrupted suture.

Abdominal view after strategic laparoscopic surgery for improved cosmesis sleeve gastrectomy with one visible 5-mm incision in the right subcostal region. All other laparoscopic incisions are hidden within the umbilicus.
Conventional laparoscopic sleeve gastrectomy was performed with five abdominal trocars, including three 5-mm trocars, one 12-mm trocar, and a 15-mm trocar. These incisions are placed throughout the upper abdominal wall. Upon completion, the incision of the 15-mm trocar was extended to 2.5 cm to accommodate the removal of the gastric specimen.
Statistical analyses
All data were expressed as mean±standard deviation values. Analyses of differences between groups for demographic and perioperative data were performed using two-sample t tests or Fisher's exact tests for categorical data. Data for SLIC sleeve gastrectomy patients that required conversion to conventional laparoscopic technique were examined within the SLIC group. Statistical analysis was performed using a standardized biomedical software (Statview®, SAS Institute Inc., Cary, NC). A P value of <.05 was considered significant.
Results
From April 2008 to October 2010, 127 patients underwent SLIC procedures: 38 SLIC cholecystectomy, 56 SLIC gastric banding, 26 SLIC sleeve gastrectomy, 1 SLIC gastrojejunostomy, and 6 SLIC appendectomy. During the same time period, conventional laparoscopic surgery was also performed on 56 patients for cholecystectomy, 83 patients for gastric banding, and 28 patients for sleeve gastrectomy. Although there were many laparoscopic appendectomies performed within this same time period, they were performed by a different service, and the SLIC technique was not used. Overall, there was no 30-day or in-hospital mortality in the study cohort. The 30-day re-admission and re-operation rates were also 0%.
SLIC cholecystectomy
Two of 38 patients (5.3%) required conversion to four-port laparoscopy because of severe adhesions and difficulty in retraction of the gallbladder. One patient required placement of one additional 5-mm trocar for dissection of the cystic duct. The mean operative time was 65 minutes (range, 30–110 minutes). The mean length of stay was 0.5 days (range, 0–1 days). There were no intraoperative complications. There were no major or minor postoperative complications. Specifically, there were no postoperative biliary complications.
SLIC appendectomy and gastrojejunostomy
For SLIC gastrojejunostomy and appendectomy, none of the patients required conversion to conventional laparoscopy. The mean operative time for SLIC appendectomy was 26 minutes (range, 15–40 minutes). The operative time for SLIC gastrojejunostomy was 40 minutes. The mean length of stay was 1.5 days (range, 1–3 days). There were no postoperative complications.
SLIC gastric banding
Three of 56 patients (5.4%) had conversion to five-port laparoscopy for inadequate exposure and visualization. The mean operative time was 59 minutes (range, 35–140 minutes). The mean length of stay was 1.2 days (range, 1–2 days). There were no major or minor complications. Late complication included 1 patient (1.8%) with band slippage.
Conventional laparoscopic versus SLIC sleeve gastrectomy
Perioperative data of the two groups are shown in Table 1. Age and gender were similar between the two groups; however, the mean BMI was higher in the laparoscopic group (47 versus 42 kg/m2, P=.01). The mean operative time was similar between groups (78±26 minutes for laparoscopic versus 84±24 minutes for SLIC). In the laparoscopic sleeve gastrectomy group, all cases were performed successfully without conversion to open laparotomy. In the SLIC sleeve gastrectomy group, 1 of 26 patients (3.8%) required conversion to conventional five-trocar laparoscopic technique. The estimated blood loss was similar between groups (23±14 mL for laparoscopic versus 30±21 mL for SLIC). Intraoperative complications in the SLIC group included staple-line failure (n=1) and liver laceration (n=1). The length of hospital stay was similar between groups (1.4±0.6 days for laparoscopic versus 1.8±0.7 days for SLIC). None of the patients in either group required stay in the intensive care unit. There were no major complications. Minor complications occurred in 7.7% in the SLIC sleeve group (severe nausea and wound infection) and 8.3% in the laparoscopic sleeve group (severe gastroesophageal reflux disease and atrial fibrillation). Late complications included cholecystitis (n=1) in the SLIC sleeve group.
BMI, body mass index; NS, not significant; SLIC, strategic laparoscopic surgery for improved cosmesis.
Discussion
The quest to reduce the spectrum of surgical invasiveness continues with natural orifice surgery and clinical application of SLIC. The transition from open to laparoscopic surgery has forever changed the field of general surgery with the majority of general and bariatric operations now performed with the laparoscopic approach. Strategic laparoscopy for improved cosmesis may possibly be the next minimally invasive surgical approach on the path to natural orifice surgery. In this study, we found that SLIC general and bariatric operations can be performed safely and associated with a short learning curve and a low conversion rate to laparoscopy. In a cohort analysis of conventional laparoscopic versus SLIC sleeve gastrectomy, we found that SLIC sleeve gastrectomy can be performed safely utilizing surgical incisions mostly hidden within the umbilical verge, with perioperative outcomes comparable to those of conventional sleeve gastrectomy.
The transition from open to laparoscopic surgery has resulted in significant physiologic and clinical benefits. However, the transition from laparoscopic surgery to SLIC has shown much less forward progress, to include possibly lower postoperative pain and improved cosmesis. Therefore, it is imperative to develop a SLIC technique that would be reproducible and can be performed as safely as conventional laparoscopic surgery. There needs to be a balance between the clinical benefits of SLIC and safety of the procedure, with safety being the first priority. Our technique for SLIC procedures has evolved over the course of the present case series to achieve the above philosophy. For SLIC cholecystectomy, we initially only used three trocars placed within the umbilicus to perform the operation. Although feasible in certain cases, the technique only provides a single port for retraction of the gallbladder. Our current technique uses an additional 2-mm rigid percutaneous access instrument to retract the fundus of the gallbladder, giving the surgeon both cephalad and lateral retraction of the gallbladder similar to the operative angles of retraction of laparoscopic cholecystectomy. For SLIC appendectomy, the procedure can be performed with ease using three trocars placed within the umbilicus, and hence we have not altered our technique. For gastric banding, initially a 4.5-cm incision was placed between the xiphoid and the umbilicus through which four laparoscopic trocars were placed. Using this technique, we encountered significant “fighting” of instrumentation due to the close proximity of the instruments. Our current technique has evolved to include a smaller incision (3.5 cm) made between the xiphoid process and the umbilicus to accommodate two laparoscopic trocars and an additional two 5-mm trocars placed within the umbilicus for placement of a flexible camera and a retracting instrument. This simple alteration in technique significantly reduced our instrument interaction and has also reduced the size of the incision for implantation of the subcutaneous port. One of the most difficult tasks during SLIC is the performance of laparoscopic suturing and intracorporeal knot tying. In this series, we used an automated suturing device to perform laparoscopic suturing, and the knot tying was performed extracorporeally using an automated knot-tying device. Lastly, for SLIC sleeve gastrectomy, we initially performed the procedure through a single 4.5-cm incision placed between the xiphoid process and the umbilicus. The technique later evolved to three laparoscopic incisions placed within the umbilicus. More recently, we added an additional 5-mm trocar in the right subcostal region to facilitate retraction of the liver.
The equipment used for SLIC in our series includes conventional low-profile trocars, rigid instrumentation, and visualization platform. Many specialized ports have been developed for SLIC. These ports require a single skin incision with a similar size fascial incision. An issue about making a relatively larger fascial incision is the risk for late incisional hernia. Our technique involve placement of separate incisions at the umbilical verge to allow an improved degree of instrument interaction. Additionally, the fascia is made only large enough to accommodate the surgical specimen; hence there should not be an increase in the rate of incisional hernia. With regard to instrumentation, our technique uses mostly conventional rigid hand instrument. It is helpful, however, to have longer length (42 cm) for these instrumentations. In certain cases, such as SLIC cholecystectomy, there is an occasional need to have an articulating instrument to dissect out the cystic duct and artery. A specialize 2-mm percutaneous retracting instrument is also useful during SLIC cholecystectomy for retraction of the gallbladder. We routinely use the ultrasonic dissector for our conventional laparoscopic cholecystectomy and also use it for our SLIC cholecystectomy. In prospective randomized trials of patients undergoing laparoscopic cholecystectomy with dissection by ultrasonic energy versus monopolar energy, ultrasonic energy resulted in shorter operative time, lower gallbladder perforation risk, lower postoperative pain, and shorter mean length of hospital stay, 2 although higher cost remains the main disadvantage in the use of the current ultrasonic devices. With regard to the visualization platform, we use the conventional flexible-tip 5-mm endoscope as it provides a variable degree of image articulation. Because our technique uses mostly existing ports, instrument, and imaging endoscope, the cost for SLIC should be similar to or only slightly higher than that of the conventional laparoscopic operation.
There have been many reports of SLIC cholecystectomy.3–9 The SLIC technique varies among the different series with regard to fundal retraction of the gallbladder. In this study we used a rigid 2-mm grasping instrument to directly retract the gallbladder. An alternative technique is to perform transabdominal suture retraction of the gallbladder. 7 With SLIC cholecystectomy, the risk for bile leak and common duct injury remains a concern. There have been six published case series of SLIC cholecystectomy with reported bile leak complications ranging between 1% and 3.7%.3–9 Solomon et al. 6 reported a single case of duct of Luschka leak after 54 cases of SLIC cholecystectomy. Roberts et al. 5 similarly reported a case of a duct of Luschka leak after 56 SLIC cholecystectomy cases. Roy and De 8 reported 1 of 50 cases developing a biliary leak from an accessory duct in the gallbladder fossa. Edwards et al. 7 reported the highest biliary leak rate at 3.7%. They found three biliary complications after 80 SILS cholecystectomies: two from accessory ducts and one from a cystic duct stump leak. Kuon et al. 3 reported a single case of intraoperative right hepatic duct injury as a result of electrocautery. The duct injury was treated with endoscopic retrograde cholangiopancreatography and stent placement. Lastly, Hernandez et al. 4 reported a case of cystic duct stump leak after 100 cases of SLIC cholecystectomy. In contrast, Curcillo et al. 9 reported the largest experience of SLIC cholecystectomy with 297 patients with a 0% incidence of bile leak or injury. Our technique of SLIC cholecystectomy, which provides both cephalad and lateral retraction of the gallbladder, should minimize the risk of bile leak complications as the procedure is similar to that of laparoscopic cholecystectomy. In addition, surgeons should have a low threshold for conversion from SLIC to conventional four-port laparoscopy in cases with poor visualization and poor operative exposure.
There have been few reports of single-incision laparoscopic gastric banding, and the technique varies among reports (Table 2).10–13 Teixeira et al. 10 reported their initial experience of 22 cases of SILS gastric banding. They used a 3.5-cm umbilical incision to accommodate placement of a liver retractor and three abdominal ports. There are potential drawbacks to their technique. First, the incision is placed at the umbilicus, which is often a long distance away from the area of interest, the gastroesophageal junction and angle of His. Second, the umbilicus is an area with potential for bacterial colonization, hence possibly a higher risk for wound infection. The mean operative time in their series was 82 minutes with no perioperative complications; 1 patient (4.5%) required conversion to conventional laparoscopy. 10 Saber and El-Ghazaly 11 similarly reported SLIC gastric banding in 8 patients performed through a 2.5-cm periumbilical incision; the mean operative time was 105 minutes with no reported postoperative complications. The largest series to date reported SLIC gastric banding in 60 patients performed through a 4.5-cm periumbilical incision and a separate subxiphoid incision for retraction of the liver. 12 The mean operative time was 55 minutes. Conversion to conventional laparoscopy occurred in 6.7% of cases. Wound infection occurred in 5 patients (8.3%), and 2 of 5 patients had dehiscence of the wound with possible involvement of the port. 12 The results from this series caution against placement of the implantable port within a periumbilical incision. An increase in the rate of port-site infection as observed in their series would negatively impact any potential benefit of SLIC. Our technique for SLIC gastric banding specifically places the single incision away from the umbilicus to avoid any potential for wound complications. There has been only one comparative study evaluating laparoscopic versus SLIC gastric banding. Nguyen et al. 13 reported on 23 laparoscopic gastric bandings versus 23 SLIC gastric bandings. The conversion rate in the SLIC group was 13%. There were no significant differences in operative time or length of stay between the two groups. There were also no postoperative complications in either group.
LOS, length of stay; OR, operating room.
The use of SLIC has also been applied to complex operations such as construction of a gastrointestinal anastomosis. Nguyen et al. 14 reported a single case of performing a gastrojejunal anastomosis through transumbilical trocars. SLIC gastric bypass has also been reported. Huang et al. 15 reported 32 patients who underwent SLIC gastric bypass through a periumbilical incision. The mean operative time was 101 minutes with a mean length of stay of 1.2 days. There were no major complications. Minor complications included wound seroma in 1 patient. 15 Although SLIC gastric bypass is feasible, more clinical studies are needed to document the safety of this particularly complex procedure performed through a single incision.
There have been few reports of SLIC sleeve gastrectomy (Table 3).16–18 Gentileschi et al. 16 reported outcomes of 8 SLIC sleeve gastrectomies; the mean operative time was 128 minutes with a mean hospital stay of 2.4 days. Galvani et al. 17 reported SLIC sleeve gastrectomy in 7 patients; the mean operative time was 103 minutes, and there were no postoperative complications. Saber et al. 18 reported a comparative study of laparoscopic (n=12) versus SLIC (n=14) sleeve gastrectomy and found that SLIC sleeve gastrectomy was associated with less postoperative pain and a shorter length of hospital stay. In our study, we report the largest series of SLIC sleeve gastrectomy to date and found that outcomes of SLIC sleeve gastrectomy are comparable to those of conventional sleeve gastrectomy with respect to operative time, length of hospital stay, postoperative morbidity, and 1-year weight loss.
There are several limitations to this study. First, this report was not a randomized comparison, and therefore we were unable to assess the potential clinical benefits of SLIC sleeve gastrectomy, such as reduction in postoperative pain and shorter convalescence. Second, patients who underwent SLIC sleeve gastrectomy were a select group of patients with a relatively lower BMI. The safety and feasibility of SLIC sleeve gastrectomy technique in patients with BMI >50 kg/m2 are not known. Lastly, other relative contraindications for SLIC include the presence of large ventral hernia and previous abdominal surgery, which often require conventional laparoscopy for lysis of adhesions. In addition, the SLIC approach was not selected for revisional operation such as conversion of gastric banding to sleeve gastrectomy or when a combination of operation is required such as performance of gastric banding with cholecystectomy or gastric banding with hiatal hernia repair. Despite these limitations, this study is the largest study to date to compare SLIC sleeve gastrectomy with conventional laparoscopic sleeve gastrectomy and shows that SLIC sleeve gastrectomy can be performed safely with similar perioperative outcomes and is associated with a relatively short learning curve.
In conclusion, SLIC general and bariatric operations are technically feasible, safe, and associated with a low rate of conversion to conventional laparoscopy. Compared with laparoscopic sleeve gastrectomy, SLIC sleeve gastrectomy can be performed safely without prolonging the operative time and with comparable perioperative outcomes. The SLIC procedures were performed with mostly existing ports, laparoscopic instrumentation, and visualization platforms, which make the cost of this procedure comparable to that of the laparoscopic procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.