
Abstract
Abstract
Background:
Laparoscopic sleeve gastrectomy (LSG) represents a valid option for morbidly obese patients, either as a primary or as a staged procedure. Staple-line reinforcement (SLR) is strongly advocated to decrease the chance of bleeding. The aim of this article is to report our experience with a new technique of SLR using a thrombin–gelatin matrix in a series of morbidly obese patients subjected to LSG.
Subjects and Methods:
Patients subjected to LSG using a thrombin–gelatin matrix for SLR from April 2010 to April 2011 were included in the study. Each patient's record was registered and prospectively collected for the analysis.
Results:
Seventy-four patients were subjected to LSG using a thrombin matrix for SLR. There were 56 female and 18 male subjects with a mean age of 44.8 years (range, 16–64 years). Mean preoperative body mass index was 46.2 kg/m2 (range, 40–72 kg/m2). Mean operative time was 74.4 minutes (range, 58–96 minutes). Mean time for application of the thrombin matrix was 4.8 minutes (range, 3.2–6.6 minutes).
Conclusion:
LSG with a thrombin matrix for SLR is a safe operation and a valid alternative to other well-established techniques.
Introduction
Main drawback of LSG is the severity of postoperative complications, mainly bleeding 3 and gastric leak 4 ; less severe complications are development of gastroesophageal reflux disease, 5 stricture 6 or dilation 7 of the gastric tube, and insufficient weight loss. 8 The incidence of significant hemorrhage from the staple line is reported to be in the range of 1.6%–10%. 9 Staple-line leaks represent the most dangerous and life-threatening complication after LSG, with a mean incidence of 2.7% from 24 studies with 1,749 patients. 10 Leaks after sleeve gastrectomy commonly occur at the proximal aspect of the staple line, immediately below the gastroesophageal junction, because of the creation of a high internal pressure.
Staple-line reinforcement (SLR) is actually strongly advocated but not well standardized. There are different options of SLR: Oversewing the staple line or buttressing it with specific bioabsorbable material, such as glycolide trimethylene carbonate copolymer (Gore Seamguard® [W.L. Gore & Associates, Inc., Flagstaff, AZ]), 11 bovine pericardium strips (Peri-Strips Dry® and Peri-Strips Dry with Veritas® [Synovis Surgical Innovations, St. Paul, MN]), 12 or porcine small intestinal submucosa (Surgisis Biodesign® [Cook Medical, Inc., Bloomington, IN]). 13 Although a reduction of staple-line complications has been postulated using SLR, the published articles have failed to show a clear benefit using each technique.
No literature study reports the application of hemostatic agents or sealants over the staple line after LSG, aiming to better control postoperative bleeding. The purpose of this article is to report our preliminary experience with a new technique of SLR, using a thrombin–gelatin matrix, in a series of morbidly obese patients subjected to LSG.
Subjects and Methods
From April 2010 to April 2011, morbidly obese patients undergoing LSG and SLR with a thrombin–gelatin matrix (Floseal®, Baxter International, Deerfield, IL) in our Department of Surgical Sciences at the University of Rome “Tor Vergata,” Rome, Italy, were included in the study.
They were studied preoperatively by means of a multidisciplinary work-up with a nutritionist, psychiatrist, and medical internist. An upper gastrointestinal endoscopy was performed to rule out incidental pathologies. Cardiorespiratory functional evaluation was carried out if required. Every patient was extensively informed about the surgical procedure, with all potential advantages, possible complications and side effects, and expected results according with the recent literature.
An intravenous dose of cephalosporin (2 g) was administered as antibiotic prophylaxis immediately before surgery; thromboprophylaxis included elastic stockings and low-molecular-weight heparin pre- and postoperatively.
Indications for LSG were the following conditions: body mass index (BMI) over 60 kg/m2 in high-risk patients; BMI between 50 and 60 kg/m2 in patients without diabetes; BMI between 40 and 50 kg/m2 in patients refusing a complex procedure like Roux-en-Y gastric bypass; patients with severe gastric inflammatory disease and Helicobacter pylori infection; patients with previous abdominal surgery involving the intestines; and young patients not suitable for gastric banding. Specific contraindications, apart from the general contraindications to bariatric surgery, were severe and documented gastroesophageal reflux disease and previous gastric surgery.
Surgical technique
The patient was placed in a supine position on the operating table with arms extended in abduction and legs opened, in reverse Trendelenburg position with a 30° tilt. The surgeon stood between the legs, with the assistant on the left side of the patient and the cameraperson to the patient's right. Abdominal insufflation was set at 15 mm Hg. Trocars were placed as follows: A 10-mm trocar (T1) 20 cm below the xyphoid process for the 30° optical system; a 5-mm trocar (T2) on the left anterior axillary line; a 12-mm trocar (T3) on the left midclavicular line just between the first and the second trocars; a 12-mm trocar (T4) on the right midclavicular line; and a 5-mm trocar (T5) below the xyphoid process. Using a dissecting coagulator (Ultracision®, Ethicon Endo-Surgery, Cincinnati, OH), the greater curvature of the stomach was mobilized at a point 3 cm proximal to the pylorus. The lesser sac was entered, and with the surgery staying close to the wall of the stomach, the greater curvature ligaments (gastrosplenic and gastrocolic) were divided all the way up to the angle of His.
We paid particular attention to the identification and mobilization of the angle of His with exposure of the left crus of the diaphragm to delineate the gastroesophageal junction and to facilitate complete resection of the gastric fundus. Retrogastric adhesions were removed to allow for complete mobilization of the stomach, to eliminate any redundant posterior wall of the sleeve, and to exclude the fundus from the gastric sleeve.
After a complete mobilization of the stomach was reached, a 40-French orogastric tube was inserted transorally into the pylorus and placed against the lesser curvature. This helped to calibrate the size of the gastric sleeve, prevent any constriction at the gastroesophageal junction, and provide a uniform shape to the entire stomach.
Gastric transection by a cutting stapler (Echelon Flex™ Endopath®, Ethicon Endo-Surgery) was begun at a point 3 cm proximal to the pylorus, leaving the antrum and preserving gastric emptying. The stapler was fired consecutively along the length of the orogastric tube until the angle of His was reached; we used the green load for the thicker gastric antrum and the blue load for the remaining corpus and fundus. Care was taken not to narrow the stomach at the angularis. Moreover, at this point we inspected the organ anteriorly and posteriorly, to ensure no redundant gastric tissue and to guarantee an adequate sleeve volume.
After the gastric transection was completed, the orogastric tube was removed, and the staple line was inspected for bleeding and tested for leak. With the patient flat and the pylorus gently clamped, the integrity of the staple line was assayed by insufflating air under saline and infusing 30–60 cm3 of methylene blue into the remaining stomach.
Then the entire staple line was covered by Floseal, and the matrix was carefully squeezed using the specific laparoscopic applicator (Figs. 1 and 2). In case of bleeding a little gauze was introduced into the abdomen and used to plug the suture line. At the end, the staple line was washed with saline, and the residual material was aspirated.
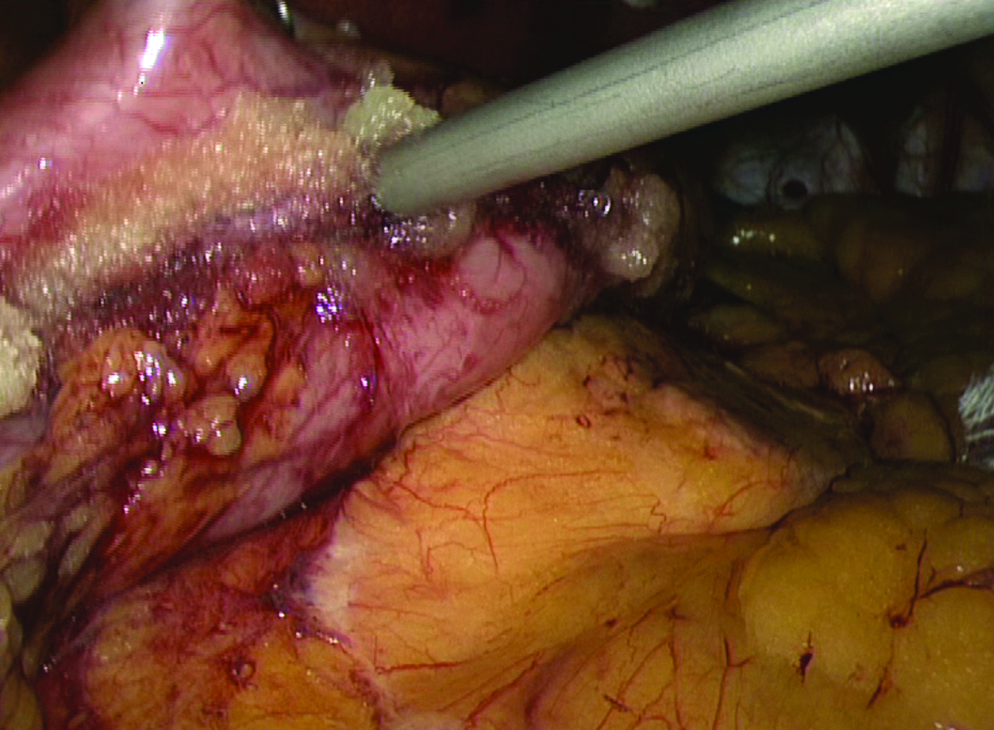
Reinforcement of the entire staple line by laparoscopic application of Floseal.

The staple line of LSG covered homogeneously by the thrombin matrix at the end of surgery.
The resected stomach was extracted through the periumbilical incision before completing the procedure. A suction drain was left in place; the procedure ended with removal of the ports under direct vision and closure of the fascial defects with a figure-of-eight 2/0 nonabsorbable suture to prevent port site hernia.
On the first postoperative day an X-ray upper gastrointestinal series with constrast medium for gastrointestinal radiography (Gastrografin®, Bracco Diagnostics, Princeton, NJ) was carried out in all patients; if it did not show any abnormal finding, a clear fluid diet was started. Patients were mobilized within the same day of surgery and discharged as soon as they could easily walk and drink, after a normal blood test check and no clinical complication. They were given a liquid diet for 2 weeks and started the regular follow-up in our outpatient clinic after 1 week from the operation. Then they entered a multidisciplinary staged evaluation for the subsequent months and years.
Patients' records were examined, and data were prospectively collected as follows: demographics; BMI pre- and post-surgery; percentage EWL (%EWL); methylene blue test and Gastrografin swallow test results; operative time; time required to apply Floseal; and hospital stay.
Results
During the study period, in total, 74 patients were subjected to LSG for morbid obesity and application of the thrombin–gelatin matrix for SLR. There were 56 female and 18 male subjects, with a mean age of 44.8 years (range, 16–64 years). There were no conversions to the open technique. Mean preoperative BMI was 46.2 kg/m2 (range, 40–72 kg/m2). Mean operative time was 74.4 minutes (range, 58–96 minutes). Mean time for application of the thrombin matrix was 4.8 minutes (range, 3.2–6.6 minutes).
The methylene blue test and the X-ray upper gastrointestinal series were negative in all patients. The thrombin–gelatin matrix was successfully applied in every subject above the entire staple line; there were no complications related to the SLR. No additional stitches were needed in cases of small intraoperative bleeding after Floseal application. There was no early or late mortality after surgery.
We observed two major postoperative complications (2.7%): One gastric stump leak (1.3%) and one major bleeding from the trocar site (1.3%), both successfully treated by laparoscopic re-exploration.
The staple-line leak occurred in a 16-year-old girl with a preoperative BMI of 68 kg/m2, subjected to LSG in April 2010. After an uneventful procedure and a regular postoperative course the patient was discharged on postoperative Day 5. She was re-admitted on postoperative Day 9 with abdominal pain and fever. Computed tomography scan with a Gastrografin swallow revealed a small leak from the gastric stump immediately below the gastroesophageal junction. She was treated with relaparoscopy, drainage, and total parenteral nutrition. A new X-ray upper gastrointestinal series 2 weeks later showed complete healing of the gastric fistula, and oral feeding was started. She is doing fine at 1-year follow-up.
The second complication was a major bleeding from a trocar site. The patient was a 42-year-old male with a BMI of 58 kg/m2 who experienced tachycardia and mild abdominal pain during postoperative Day 1. The blood sample revealed a drop in the hemoglobin level of 4.6 points, requiring transfusion of 1 unit. Hence he underwent a laparoscopic re-exploration, revealing a hemorrhage from the left epigastric artery, while the staple line was fine. Hemostasis was accomplished by an open suture. The subsequent postoperative period was uneventful.
Discussion
Bariatric surgery is the only evidence-based approach to sustainable weight loss, improving comorbidity and survival in morbidly obese patients.
LSG is a formidable operation in terms of weight loss in the short- and mid-term (5 years) periods. As a two-stage procedure, it was initially performed using a 60-French bougie with a 33% excess weight loss at 11 months. 14 Since then surgeons began using LSG as a primary procedure using smaller-sized bougies, with greater %EWL (62%). 15 In a recent systematic review, weight loss ranged from 33% to 85% of excess weight in patients subjected to LSG. 3 The durability of LSG at 5 years has been clearly demonstrated. 16
The main concerns about LSG remain unclear and need further investigation, like the risk of important postoperative complications including staple-line leak (1%–3%) and hemorrhage (3.5%). To date, there is no high-grade evidence in the literature about the need for SLR during LSG, although it is extensively debated and highly recommended by most of the authors.17–19
The main potential advantage of SLR might be the improvement of the staple-line strength, reducing the incidence of complications at this point. Whatever technique is used, the operation time is obviously prolonged with consequences on overall surgical time. As for staple line leaks, the evidence on fewer complications with SLR is even lower and weaker. 20 Chen et al. 17 in a recent review concluded that there is no reason to believe that reductions in leak rates occur because reinforcement is used, highlighting how the leak may still appear despite SLR. On the other hand, SLR seems to be effective in decreasing the incidence of bleeding after LSG.13,21 In other words, at present SLR is strongly advocated for hemostasis because of the advantages on staple-line strength, with only a supposed reduction of leaks.
Many different materials and techniques for SLR are available for each surgeon's armamentarium, although standardization is still lacking. This is because of the variability of techniques without a clear advantage of one method over the others. Many authors in the past have discussed and analyzed each single technique, but no consensus has been reached; moreover, SLR-related complications were reported, such as intraluminal migration using bovine pericardial strips, tissue ischemia, or gastric sleeve stenosis after oversewing the staple line.22,23
The use of hemostatic agents and sealants has been widely reported in bariatric surgery in various procedures. 24 In two different articles, we reported the results of a large multicenter randomized study concerning the use of a fibrin glue during laparoscopic gastric bypass, showing a reduction of the incidence of complications in the fibrin glue group.25,26 Following the trial, we continued to investigate the potential benefit of sealants in bariatric surgery, and with the growing experience with LSG we decided to evaluate the application of hemostatic agents during this procedure.
We did not find any specific report about the use of hemostatic agents (such as Floseal, for example) during LSG, either for hemostasis of the surgical field or for SLR. The idea of using Floseal came out from the experience with this matrix in general surgery and from the incidence of 3% of cases of bleeding after LSG in our previous experience with this procedure. Floseal hemostatic matrix is applied to the tissue surface at the staple line. Floseal granules expand approximately 20% within 10 minutes and physically restrict the flow of blood. Blood percolates through the spaces and is exposed to thrombin. A clot forms around the mechanically stable matrix provided by the granules. The structural integrity of the gelatin–fibrin matrix enables it to remain in place at the tissue surface. The granules not incorporated in the clot can and should be removed with gentle irrigation without disrupting the hemostatic seal. Floseal is reabsorbed by the body within 6–8 weeks, consistent with the time frame of normal wound healing. 27
In this preliminary evaluation of Floseal for SLR, we had no technical difficulty or intraoperative complication related to the thrombin matrix. After the gastric transection was accomplished, the SLR was easily obtained by using the laparoscopic applicator, which allowed positioning the Floseal even at the top of the staple line, close to the esophagogastric junction. During the procedure, no risks of conversion to open surgery were encountered.
Compared with the oversewing suture, which usually requires several minutes to be accomplished, SLR with Floseal is faster; in this way it is possible to avoid longer operative time for patients who often have several comorbidities.
In the presence of some bleeding from the staple line, we observed a quick hemostasis after the Floseal was squeezed, without the need of adjunctive stitches. Nevertheless, although the thrombin–gelatin matrix is effective in the presence of oozing or raw bleeding surfaces, it does not replace an adequate and focused hemostasis of actively bleeding vessels.
Furthermore, using a fluid material it is possible to avoid specific complications, such as ischemia or stenosis of the sleeve rather than permanence of a foreign body and intraluminal migration, which has been observed with other SLR techniques.
One of the potential controversies of utilization of this matrix could be the cost of the Floseal. The aim of this study was not a specific financial evaluation of SLR; anyway, for each patient we used a single 5-mL application, with a charge of about 260 euros. This increase of the expenditure has to be compared with that of the other SLR methods. Specifically, the oversewing suture is associated with an important lengthening of the operative time and therefore with an increase of operating room cost, whereas the buttressing materials are themselves expensive surgical tools. Future systematic analysis is needed to provide accurate data on the total cost of SLR techniques.
In conclusion, early results from this study show that the application of Floseal for SLR is easy and safe, without a large impact on the operative time. This hemostatic agent has the potential to prevent postoperative hemorrhage of the staple line after LSG, although more data and comparison with other methods are needed in order to obtain definitive results. At present, however, SLR with Floseal should be considered a valid alternative to other well-established techniques in an attempt to decrease complications after LSG.
Footnotes
Disclosure Statement
No competing financial interests exist.