
Abstract
Abstract
Background:
Laparoscopic cholecystectomy, particularly in the same hospital stay, has been widely recommended to treat gallstone-pancreatitis over the last decade. Although pancreatitis produces severe oxidative injury, laparoscopy exerts an additional effect over that is produced by pancreatitis. The preconditioning phenomenon previously reported as protective in open surgery is a beneficial maneuver also in laparoscopic surgery. So in the present study we have tried to find out the effect of laparoscopic preconditioning over the pancreatitis in cerulein-induced pancreatitis rats.
Methods:
Acute pancreatitis was induced in 24 rats weighing between 280 and 350 g by three subcutaneous injection of 80 μg/kg of body weight cerulein. A 1-cm midline laparotomy was performed for all rats, and then they were randomly assigned to one of the following three groups (n=8 for each): Group I (control), Group II (laparoscopy), and Group III (laparoscopic preconditioning [L-Pre]). After that, a catheter was placed into the peritoneum for the creation of the pneumoperitoneum (Pp) in all the animals except the control group. The rats of Groups II and III were subjected to 60 minutes of Pp with 15 mm Hg intraabdominal pressure followed by 30 minutes of deflation. The L-Pre procedure was applied to Group III immediately before the laparoscopic procedure. Blood samples were taken for biochemical assays. Pancreas tissue samples were taken for light microscope analysis.
Results:
The light microscopy of the pancreas tissues revealed that cerulein injection caused edema and sparse inflammatory cell infiltration mimicking the edematous pancreatitis. However, the application of laparoscopy over the pancreatitis produced significant inflammatory cell infiltration, acinus vacuolization, and necrosis (in one case) in addition to edema. But, the laparoscopic preconditioning maneuver applied before the laparoscopy significantly decreased in particular acinary vacuolization and cell infiltration. Therefore the total sum of the histopathological score of the L-Pre group was significantly less than that of the laparoscopy group. The biochemical analysis of the groups revealed that laparoscopy caused significant elevation of malondialdehyde levels and decrease of reduced glutathione values. However, the addition of preceding preconditioning produced significant amelioration of these parameters.
Conclusion:
Laparoscopic preconditioning may be a useful method to decrease the oxidative injury in cases undergoing cholecystectomy for biliary pancreatitis. But, it should be emphasized that this was a restricted experimental study, and further clinical studies are needed to adopt these results into clinical settings.
Introduction
Cerulein-induced acute pancreatitis is the most widely explored experimental model in this topic. Cerulein is a rapidly inducible agent and has a highly reproducible course. The changes relevant with cerulein-induced pancreatitis can easily be detected because the histological picture of cerulein-induced pancreatitis resembles the early phase of acute edematous pancreatitis in humans. 3 Cerulein causes acinar intracellular changes leading eventually to production of oxygen-derived radicals. If the amount of radicals produced exceeds the capacity of the intrinsic scavenger system, oxidative injury occurs, and cellular membrane damage begins. This damage then causes the leakage of excess free radicals, pancreatic enzymes, and cellular debris into the interstitium. This vicious cycle is propagated by the production of more oxygen radicals and injury to other structures such as capillaries. 4 Inflammatory cell infiltration acts at least partially in this mechanism because Guice et al. 5 reported that neutrophil and complement depletions prevent early edema formation in cerulein-induced pancreatitis. Several exogenous scavengers have been tried to reduce the oxidative injury observed after cerulein induction in the literature.6–9 Oxidative stress observed after cerulein-induced pancreatitis can be documented by showing the accumulation of lipid peroxidation products and depletion of natural scavenger system enzymes biochemically. The histopathologic features seen after cerulein injection can be demonstrated by observing the edema, inflammatory cell infiltration, acinar cell vacuolization, hemorrhage, and necrosis in hemotoxylin and eosin–stained pancreatic tissues by light microscopy.
Laparoscopic surgery is widely used in gallstone pancreatitis as well as other areas of surgery. However, it produces unique oxidative injury mainly caused by the ischemia–reperfusion mechanism. Therefore, in the case of biliary pancreatitis, laparoscopy produces an additional increase of oxidative injury over that caused by pancreatitis itself after laparoscopic cholecystectomy. So, some kinds of preventive measures should be applied before laparoscopy in order to reduce the post-laparoscopic oxidative injury overwhelming the pancreatitis. Therefore we have conducted the present study to evaluate whether laparoscopic preconditioning (L-Pre) could be applied before laparoscopy to reduce the oxidative injury in rats with cerulein-induced pancreatitis.
Materials and Methods
The current study was conducted with the approval of the University Ethical Committee dated November 29, 2010 with protocol identification number B302AKU0920000/148. The experiment protocol was designed in accordance with the guidelines for the National Institutes of Health. 10 Twenty-four rats weighing between 280 and 350 g were included into the study. Animals received standard rat chow and tap water ad libitum. Following an overnight fasting acute pancreatitis was induced in the animals by three subcutaneous injection of 80 μg/kg body weight cerulein (Sigma-Aldrich, Munich, Germany). After a 1-hour observation period from the last cerulein injection the rats were anesthetized with an intramuscular injection of ketamine HCl (5 mg/kg, Ketalar®; Eczacibasi-Warner Lambert, Istanbul, Turkey). An additional dose or doses of ketamine (1 mg/kg, intramuscularly) were given for the rats that required excess anesthesia throughout the experiment protocol. A 1-cm midline laparotomy was performed for all rats, and then they were randomly assigned to one of the following three groups (n=8 for each): Group I (control), Group II (laparoscopy), and Group III (L-Pre). After that a catheter was placed into the peritoneum for the creation of the pneumoperitoneum (Pp) in all the animals except the control group by using a technique described by our group previously.22,24 The rats of Groups II and III were subjected to 60 minutes of Pp with 15 mm Hg intraabdominal pressure followed by 30 minutes of deflation. The L-Pre procedure was applied to Group III immediately before the laparoscopic procedure. For the purpose of this study L-Pre was defined as 5 minutes of Pp with 15 mm Hg intraabdominal pressure followed immediately by 5 minutes of deflation. Group III remained under anesthesia for a total of 100 minutes, whereas the total anesthesia period in the other groups was 90 minutes. The study was concluded with seven rats in Group II and eight rats in the other groups.
At the end of the experimental procedure, laparotomy incisions were opened and extended. Blood samples were taken from the aorta and withdrawn into heparinized tubes for biochemical assays. The pancreas was reached, and a 2-×2-cm tissue piece was obtained. The rats were then sacrificed with an intracardiac potassium injection. The pancreas tissue samples were immersed in 10% formaldehyde for light microscope analysis. Each tissue and blood sample was assigned a code number and referred to the biochemists (A.V., B.K., and A.A.) and pathologist (F.A.). Blood samples were withdrawn into the heparinized tubes, and plasma was separated by centrifugation at 800 g and 4°C over a 10-minute period. Plasma malondialdehyde (MDA) and reduced glutathione (GSH) levels were determined by the methods described by Okhawa et al. 11 and Beutler, 12 respectively. Tissue samples were prepared in fixed 10% formalin solution. They were embedded in paraffin, cut into sections 3 μm thick, and stained with hematoxylin and eosin. Each section of pancreatic tissue was scored from 0 to 3 in terms of edema, inflammatory cell invasion, acinary vacuolization, hemorrhage, and necrosis as follows:
For edema: 0, none; 1, interlobular edema; 2, interlobular and mild intralobular edema; 3, severe intralobular edema.
For inflammatory cell infiltration: 0, none; 1, sparse perivascular and periductal infiltration; 2, mild perivascular and periductal infiltration; 3, severe perivascular and periductal infiltration.
For acinary vacuolization, 0, none; 1, present in less than 25% of cells; 2, present in 25%–50% of cells; 3, present in more than 50% of cells.
For hemorrhage: 0, none; 1, 1–2 hemorrhagic foci in every preparation; 2, 3–5 hemorrhagic foci in every preparation; 3, more than 5 hemorrhagic foci in every preparation.
For necrosis: 0, none; 1, necrosis in less than 15% of pancreatic cells; 2, necrosis in 15%–35% of pancreatic cells; 3, necrosis in more than 35% of pancreatic cells.
These parameters were combined into a semiquantitative scale as described by Ceranowicz et al. 13 The total sum of histopathological scores was obtained for all groups by combining the individual parameters. The results are expressed as mean±SEM values. Data analysis were performed by using the Kruskal–Wallis nonparametric test. Differences between the paired groups were tested by the Mann–Whitney U test. Results were accepted as statistically significant at P<.05.
Results
The light microscopy of the pancreas tissues revealed that cerulein injection caused edema and sparse inflammatory cell infiltration mimicking the edematous pancreatitis (Fig. 1). However, the application of laparoscopy over the pancreatitis produced significant inflammatory cell infiltration, acinus vacuolization, and necrosis (in one case) in addition to edema (Fig. 2). But, the L-Pre maneuver applied before the laparoscopy significantly decreased in particular acinary vacuolization and cell infiltration (Fig. 3). Therefore the total sum of the histopathological score of the L-Pre group was significantly less than that of the laparoscopy group. These results are given in Table 1. The biochemical analysis of the groups revealed that laparoscopy caused significant elevation of MDA levels and decrease of GSH values. However, the addition of preceding L-Pre produced significant amelioration of these parameters. The MDA and GSH values of the groups are shown in Figure 4.
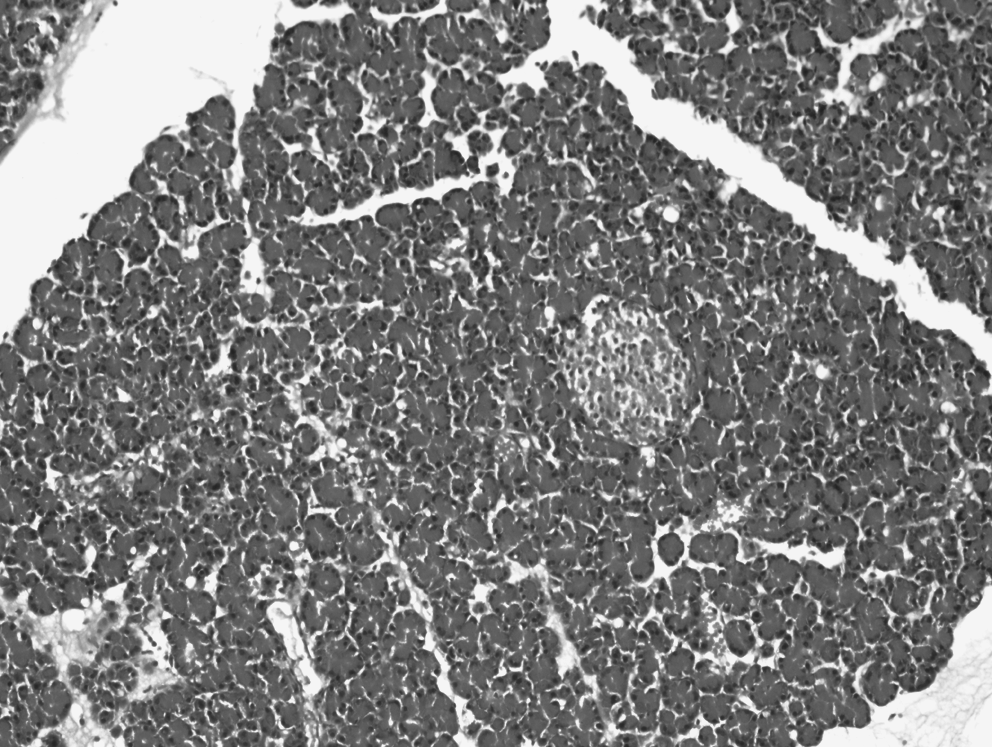
Pancreas tissue in the control group. H & E ×100.
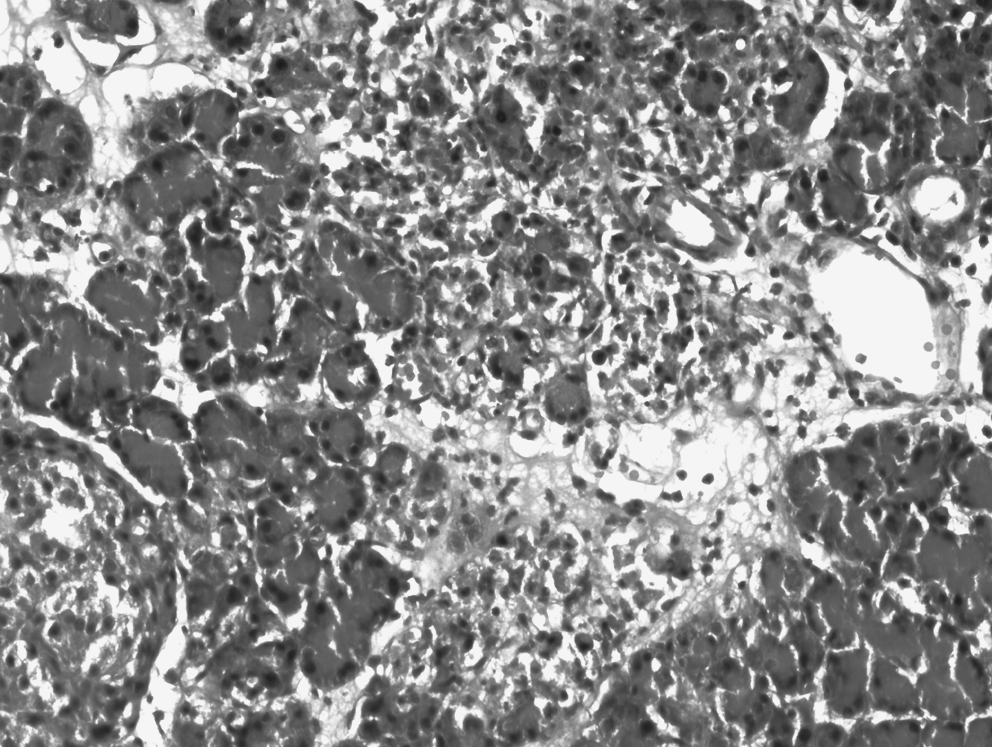
Pancreas tissue in the laparoscopy group: Moderate inflammatory cell infiltration and pancreatic necrosis in less than 15% of pancreatic cells. H & E ×200.

Pancreas tissue in the laparoscopic preconditioning group: Interlobular edema and acinar cytoplasmic vacuolization in less than 25% of pancreatic cells. H & E ×200.
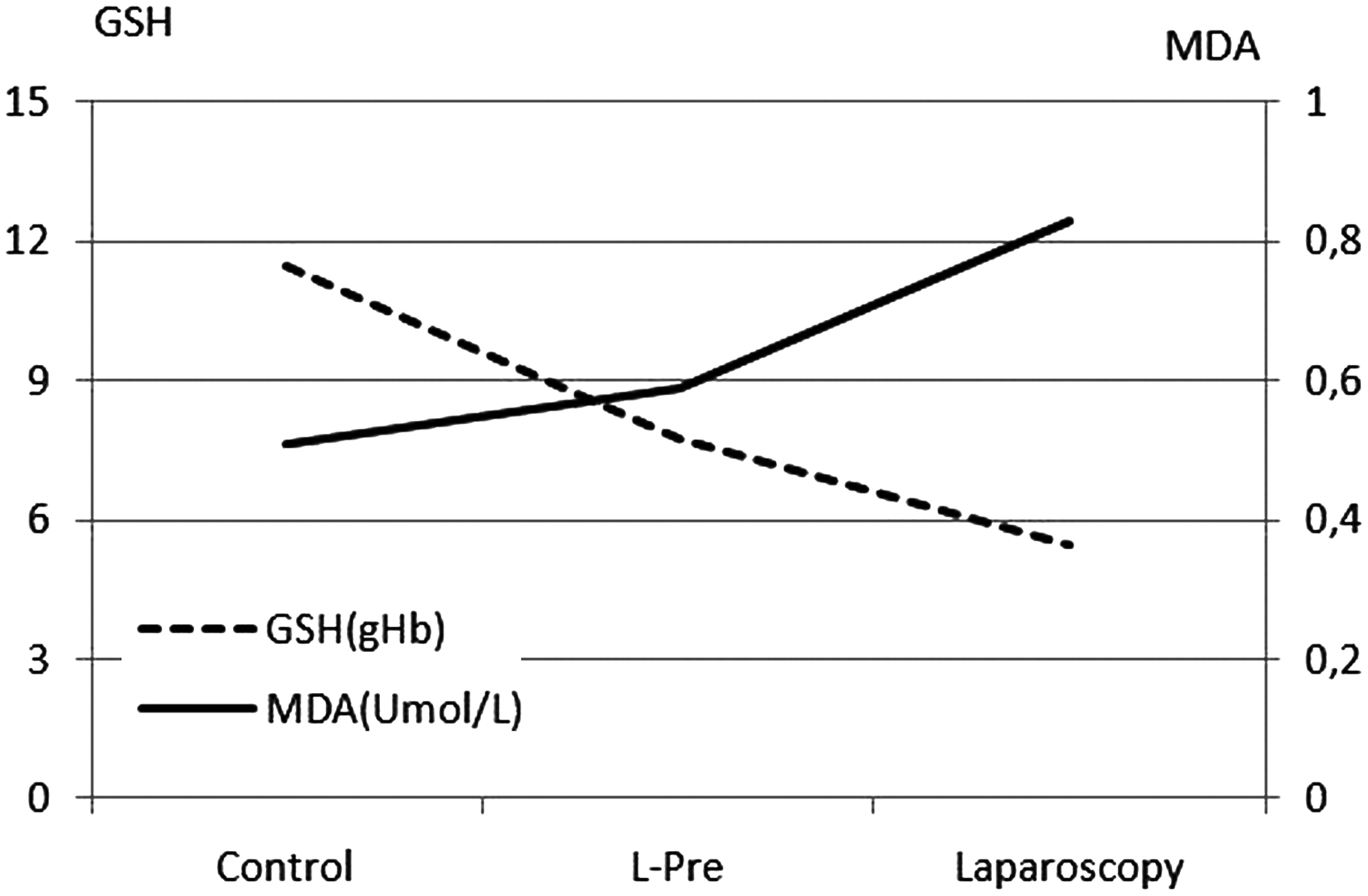
Laparoscopic preconditioning ameliorated significantly the malondialdehyde (MDA) and reduced glutathione (GSH) values. gHb, grams of hemoglobin.
Laparoscopic preconditioning (L-Pre) decreased the inflammatory cell infiltration and acinar vacuolization as well as the total sum.
Discussion
The present study was undertaken to understand the role of L-Pre in the prevention of laparoscopy-induced oxidative injury in pancreatitis rats. It is known that in experimental pancreatitis models, cerulein causes lysosomal degradation of intracellular organelles and marked interstitial edema. 14 Pancreatitis is an autodigestive disease, and acinar cell destruction eventually produce large amounts of reactive oxygen species. 15 Although the intermediate mechanisms are different, laparoscopy also produce oxidative injury. The relevant mechanisms with laparoscopy are mainly attributed to its ischemic effect because it is actually an ischemia–reperfusion injury. When we consider these the two insults together, laparoscopy in pancreatitis rats produces an overlapping attenuated oxidative injury. Several reports in the literature indicated that certain antioxidant agents such as melatonin, N-acetylcysteine, ascorbic acid, superoxide dismutase, catalase, and deferoxamine have a beneficial effect to reduce oxidative injury following cerulein-induced acute pancreatitis.16–21
In our study cerulein caused mild edema and leukocyte infiltration in pancreatic tissues. The application of the laparoscopy produced extensive inflammatory cell infiltration and acinar vacuolization in addition to the findings observed in the control group. There was also mild pancreatic necrosis in 1 case in the laparoscopy group. So it was observed that laparoscopy not only intensified the histopathologic findings that cerulein caused, but also has led to the emergence of new findings. The L-Pre maneuver applied before laparoscopy decreased the intensity of inflammatory cell infiltration and acinar vacuolization. Neither necrosis nor hemorrhage was observed in this group.
When we consider the biochemical results combined with the histopathological findings, it was found that the addition of laparoscopy on pancreatitis increased the MDA levels significantly. However, the addition of preconditioning decreased the MDA level elevation significantly, although values stayed higher than that of the control group. Similar to these findings, GSH values were also significantly lower in the laparoscopy group, indicating scavenger consumption. But, the preconditioning maneuver significantly elevated the GSH content compared with the laparoscopy group. However, it was still lower than that of the control group.
We have previously reported the effects of laparoscopy on oxidative injury. Actually, the true weight of laparoscopy-related oxidative stress resides in the fact that it is not only an indicator of oxidative damage, but also a causal factor in progressive functional and structural deterioration. 22 Laparoscopy causes its oxidative effect at its two phases: namely, Pp and deflation. Pp produces ischemia during insufflation, whereas reperfusion injury occurs during the desufflation phase. Moreover, the generation of reactive oxygen radicals after the restoration of blood flow during the deflation phase is one of the most important mechanisms of laparoscopy-related organ dysfunction. We have previously reported that laparoscopy produces oxidative injury to the peritoneum, liver, and small intestine.22–24
Because the eventual result of laparoscopy-related organ dysfunction is assumed to be caused by its ischemic effect, we have previously tried the pre-laparoscopic administration of erythropoietin (an anti-ischemic agent) and found that it decreased the lactate dehydrogenase, tumor necrosis factor-α, and MDA values. 25 The severity of the oxidative injury of laparoscopy is dependent of the kind of gas used, the period of laparoscopy, and the set level of the intraabdominal pressure.26–28 L-Pre is a mechanical protective maneuver that consists of brief period(s) of Pp and deflation sequence(s). We have previously shown that preconditioning preceding the sustained laparoscopy prepares the tissue against the following longer period of laparoscopy, thus decreasing the post-laparoscopic oxidative injury.22,24 It can also decrease the effects of different mediators involved in microcirculatory organ dysfunction, including tumor necrosis factor-α and interleukin-6.29–31
Although there is no ideal and standard preconditioning procedure, different cycles or periods of preconditioning maneuvers can be applied to reduce the laparoscopy-related oxidative injury. Arioz et al. 32 have recommended that 5 minutes of preconditioning may be applied as well as 10 minutes in terms of ameliorating the MDA and GSH values. On the other hand, Sahin et al. 33 have recommended a step-rising CO2 insufflation model instead of the preconditioning that we have described. Our clinic routinely performs the laparoscopic cholecystectomy during the same hospital stay after the attack of gallstone pancreatitis has subsided. Such an approach has been accepted to decrease the recurrent pancreatitis episodes (approaching an occurrence of 61% after discharge), acute cholecystitis, and obstructive jaundice.
Considering the previously mentioned literature information, pancreatitis and laparoscopy produce a more pronounced oxidative injury, although the mechanisms supposed are different. So in the present study we have applied our previously defined preconditioning model to experimental pancreatitis. We found that L-Pre decreased the histopathologic injury observed after laparoscopy alone. This amelioration was related especially to decreased inflammatory cell infiltration and acinar vacuolization. It also decreased significantly the MDA value, which is a reliable marker for end-stage oxidative injury. GSH has a pivotal role in cellular defense mechanisms and plays a major role in decreasing the tissue injury induced by free oxygen radicals following ischemia–reperfusion injury. 34 We found that L-Pre also decreased the GSH consumption.
The results of the present study suggest that L-Pre may be a useful method to decrease the oxidative injury in cases undergoing cholecystectomy for biliary pancreatitis. But, it should be emphasized that this is a restricted experimental study and that further clinical studies are needed to adopt these results into the clinical setting.
Footnotes
Disclosure Statement
No competing financial interests exist.