
Abstract
Abstract
Introduction:
In the last few years laparoscopic surgery has become the gold standard for the treatment of several urological diseases such as renal cancer and ureteropelvic junction obstruction (UPJO). A transmesenteric approach for left laparoscopic pyeloplasty has been recently described in order to avoid bowel manipulation and the potentially related complications. The aim of the present study is to describe the surgical technique and the advantages of the transmesenteric approach for laparoscopic pyeloplasty, pyelolithotomy, and simple nephrectomy in our experience.
Subjects and Methods:
From December 2007 to May 2010, 12 laparoscopic procedures for left renal diseases were performed using a transmesenteric approach. The indications were left UPJO in 9 cases, left pelvic-ureteral stones in 2 cases, and left end-stage kidney disease in one case.
Results:
No conversions or intraoperative complications were observed. No blood transfusions were required. Resumption of oral intake and canalization occurred in all cases within 48 hours of the procedure. All patients had an uneventful postoperative course.
Conclusions:
The laparoscopic transmesenteric approach represents an interesting and advantageous technical improvement of minimally invasive surgery for the treatment of left renal diseases.
Introduction
The laparoscopic approach to the kidney can be either retroperitoneal or transperitoneal.2,3 When a transperitoneal approach is preferred, the classical technique implies the mobilization of the ascending or descending colon. In order to avoid this surgical step and the potential risks of bowel injuries and postoperative prolonged ileum, a transmesenteric approach has been recently described for left laparoscopic pyeloplasty (LPP).4–6
The aim of this study is to describe the surgical technique and advantages of the transmesenteric approach to the left kidney for LPP, laparoscopic pyelolithotomy (LPL), and laparoscopic simple nephrectomy (LSN) in our experience.
Subjects and Methods
From December 2007 to May 2010, 12 laparoscopic procedures for left renal diseases were performed at our center using a transmesenteric approach. The indications were left UPJO in 9 cases, left pelvic-ureteral stones in 2 cases, and left end-stage kidney disease in one case.
Preoperative characteristics of the patients (6 males and 6 females) are shown in Table 1. Two patients were obese (body mass index >30 kg/m2). American Society of Anesthesiologists score was 2 for all patients.
After induction of general anesthesia, a 16 Fr. Foley urethral catheter is applied, and the patient is placed in a lateral 60° decubitus. In 11 cases, open laparoscopy was performed using a Hasson trocar placed at the level of the umbilicus or on the pararectal line. The choice was based on the patient's body habitus. Pneumoperitoneum was induced using a Veress needle only in one case.
In 11 cases four trocars were used (one 5 mm below the xiphoid process, one 12 mm along the hemiclavear line, and one 5 mm in the iliac fossa along the anterior axillary line). In one case the procedure was performed using only three trocars (a Hasson trocar and two 5-mm trocars).
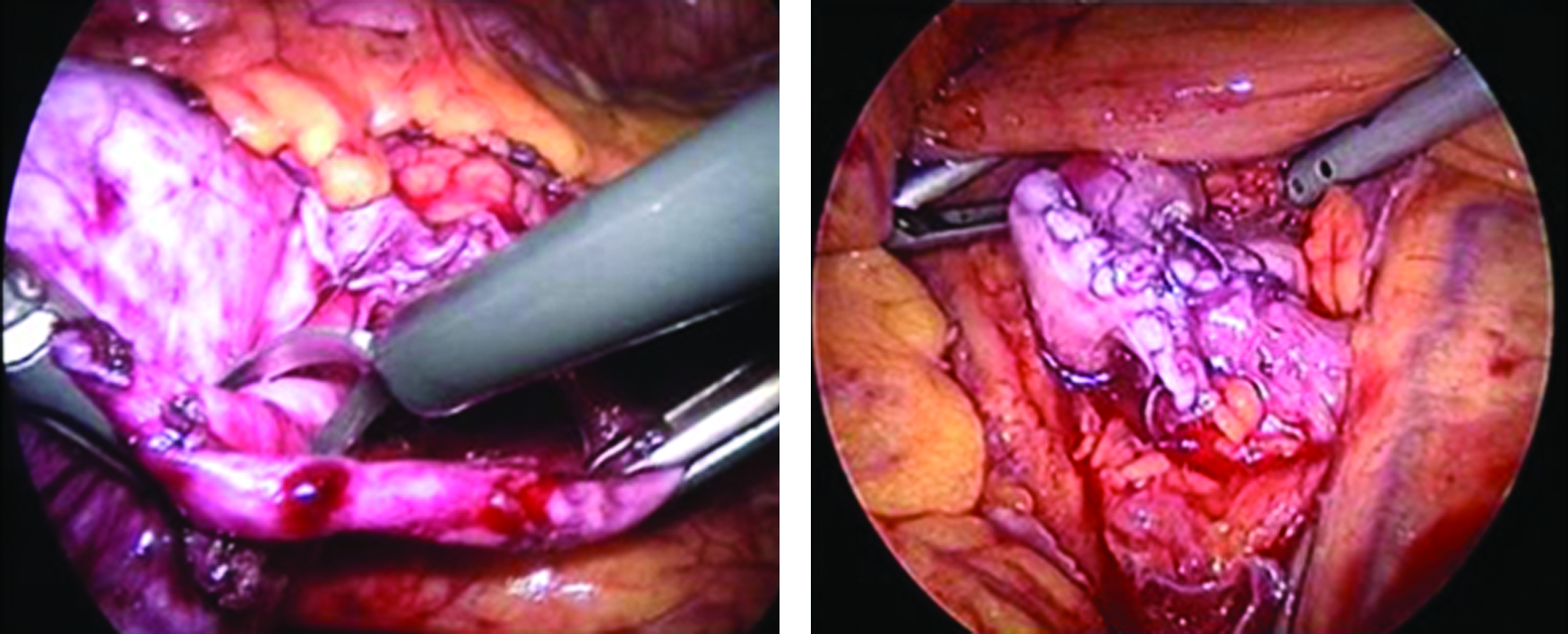
The first step of the transmesenteric technique was the exposure of the mesenterocolic space, which can be located between the descending colon and the inferior mesenteric vein and the gonadal vein (Fig. 1). The small bowel was then gently pushed medially. The renal pelvis and ureteropelvic junction can be generally easily identified underneath the peritoneum. A 3–4-cm longitudinal incision was performed through the mesentery of the descending colon in order to create a window through which the renal vessels and pelvis can be bluntly isolated (Fig. 2).
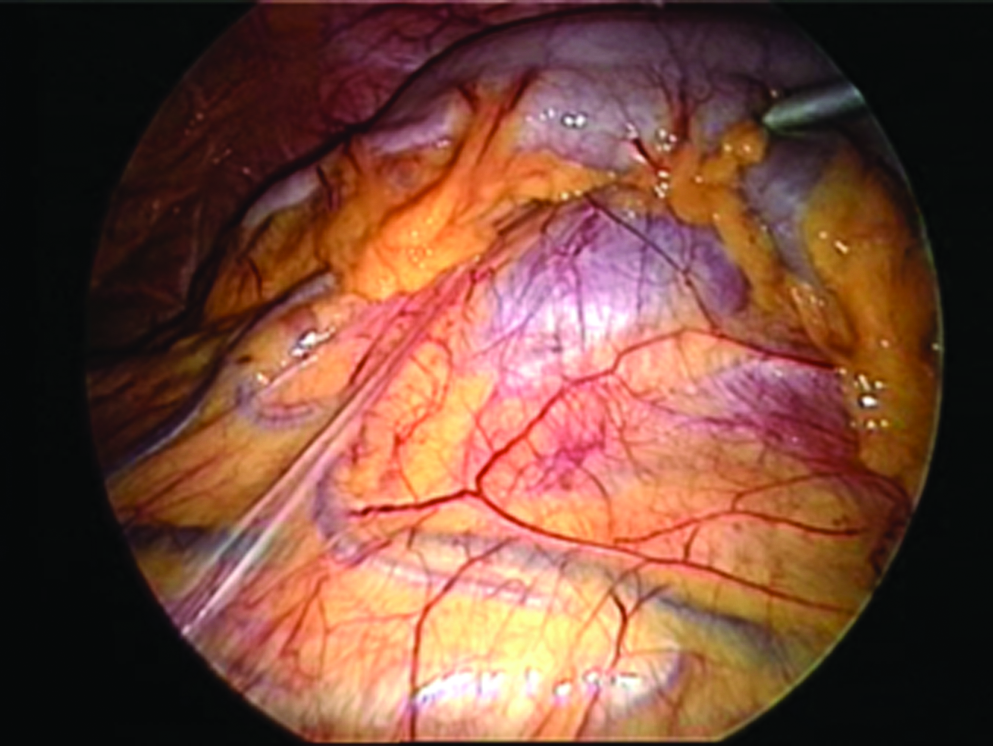
Exposure of the mesenterocolic space.

Laparoscopic dismembered pyeloplasty was performed according to the Anderson–Hynes technique in all cases of UPJO (Fig. 3). When a pyelolithotomy was performed, the renal pelvis was incised with cold scissors. Stones in the renal pelvis were retrieved with a laparoscopic grasper. A flexible cystoscope was then inserted through a 12-mm trocar to explore the renal calyces. Caliceal stones were extracted using a basket. All stones were placed in a laparoscopic bag that was extracted through one of the trocars at the end of the procedure.
In all cases of LPP and LPL a double J ureteral stent was introduced in an antegrade fashion through a 5-mm trocar with the assistance of a ureteral open-end catheter before completing the pelvic suture. The correct position of the distal end of the stent was checked with flexible cystoscopy.
LSN was performed following the classical laparoscopic steps. In this case a stitch was placed to anchor the lateral edge of the peritoneal window to the abdominal wall in order to obtain better exposure.
At the end of the procedure the mesenteric window was always closed using single reabsorbable stitches. Finally, a drainage was left into the peritoneal cavity.
Results
No conversion or intraoperative complication occurred. Blood transfusions were not needed. Intraoperative and perioperative features of the 12 procedures are shown in Table 2.
Resumption of oral intake and canalization occurred within 48 hours of the procedure in all cases. No significant postoperative complication was recorded. Blood work before discharge showed a mean hemoglobin level of 12.5 g/dL and mean white blood count of 8.25×103/μL. Creatinine was in the normal range for all patients.
The ureteral stent was always removed 20 days after the surgical procedure.
Two months after surgery all patients were investigated with clinical examination, urinalysis, urine culture, and sensitivity. All patients were asymptomatic. Abdominal ultrasound and renal scintigraphy were performed for patients who underwent LPP. In all cases the abdominal ultrasound showed reduction of hydronephrosis, and renal scintigraphy demonstrated an improved urinary excretion pattern. Patients with urinary stones were all stone-free at the plain x-ray of the abdomen performed after LPL.
Discussion
The first laparoscopic nephrectomy was performed by Clayman et al. 7 in 1991, and the first laparoscopic pyeloplasty by Schuessler et al. 1 in 1993. These techniques were quickly adopted in urological practice in centers with laparoscopic expertise. Several studies have confirmed the efficacy, safety, and excellent results of these procedures, which allow a shorter hospital stay and a earlier return to normal activities compared with open sugery. Therefore, LPP and LSN are today the gold standard for treatment of UPJO and kidney removal for benign disease. Minimally invasive procedures (extracorporeal shock wave lithotripsy, endoscopic treatment) are today preferred for the treatment of renal stones. However, LPL is sometimes needed for complex renal stones. 8
These procedures can be performed with either a retroperitoneal or a transperitoneal approach. Like several other authors, we generally prefer a transperitoneal access because it allows better vision to identify anomalous vessels or manage renal abnormalities and a wider working space that allows easier suturing of the renal pelvis and easier tying of intracorporeal knots. On the right side, mobilization of the ascending colon is not always necessary to expose the renal pelvis, whereas this is generally always required on the left side. To avoid this surgical step a transmesenteric access to the left kidney was proposed. Cisek et al. 9 first described this approach in pediatric practice, and recently a few series of transmesenteric LPP have been reported with good results.4–6 In the last few years we also applied the transmesenteric approach in our practice for treatment of UPJO and recently extended the indications to selected cases of complex stones and end-stage kidney disease. Using this technique, the mobilization of the splenic flexure of the colon and the section of the splenocolic ligament are avoided with less risk of bowel and splenic injuries. Furthermore, minimal bowel manipulation is needed, potentially leading to faster recovery of bowel peristalsis. 4
Our results confirm the potential advantages of the approach. In fact, no complications related to injuries of abdominal organs were observed, and blood transfusions were never required. All patients showed a fast canalization and resumption of oral intake. The operative times were comparable with those of traditional laparoscopic procedures in our experience. However, a proper comparison of the length of the procedure with the two approaches is not possible because the surgeries were performed by different surgeons in different periods of their learning curve. In all cases with UPJO postoperative results showed an improved urinary excretion pattern.
In the case of renal stones, the laparoscopic approach allows the use of endoscopic instruments (such as flexible cystoscopes) to remove fragments located in calyces that would be hard to reach with laparoscopic instruments. In our experience this combination of minimally invasive treatments always allowed a complete extraction of complex stones.
Finally, to our knowledge no cases of LSN with transmesenteric approach have been previously described. Our patient had an uneventful postoperative course with no intraoperative or postoperative complications.
In conclusion, the transmesenteric approach for the treatment of left kidney diseases appears to be safe, to favor an early discharge and recovery of patients, and to obtain results comparable with the traditional technique that implies the mobilization of the descending colon. This approach represents an interesting and advantageous technical improvement of minimally invasive surgery for renal diseases.
Footnotes
Disclosure Statement
No competing financial interests exist.