
Abstract
Abstract
Background:
The role of intraoperative cholangiography (IOC) during laparoscopic cholecystectomy (LC) remains controversial. This study evaluates the outcomes of a management policy of LC without IOC.
Subjects and Methods:
Patients with symptomatic cholecystolithiasis were classified regarding their potential risk for choledocholithiasis, and those at low risk received no further investigations, whereas medium- and high-risk patients underwent preoperative magnetic resonance cholangiopancreatography (MRCP) and/or endoscopic retrograde cholangiopancreatography (ERCP) with duct clearance. Those who required duct exploration were excluded. LC proceeded without IOC. Data were collected prospectively.
Results:
Between 2002 and 2011, 717 consecutive patients underwent LC; 168 (23.4%) were classified as medium or high risk, and 57 of those had preoperative duct clearance at ERCP. The conversion rate from LC to open surgery was 4.7%. The morbidity rate was 3.9%, and there were no mortalities. Nineteen patients in the low-risk group were re-admitted, of whom three patients (0.4% of 717 patients) had choledocholithiasis on ERCP. Minor bile duct injury occurred in 3 patients, and a fourth developed ischemic bile duct stricture 7 months following open conversion.
Conclusions:
The selective use of preoperative MRCP and ERCP to detect and treat choledocholithiasis facilitates the safe application of a policy of LC without IOC. Careful operative technique is necessary to avoid duct injury.
Introduction
Subjects and Methods
Patients
Consecutive patients who underwent LC for symptomatic gallstones between 2002 and 2011 were identified. Data were prospectively collected including demographics, clinical presentation, the results of abdominal ultrasound (US), liver function tests (LFTs), classification of the risk of bile duct stones, further preoperative investigations including MRCP and ERCP, conversion rate to open surgery, operative morbidity including bile duct injury, and details of re-admissions following LC.
Classification of risk of choledocholithiasis
Patients were classified with regard to the risk for choledocholithiasis as follows. Patients with uncomplicated or locally complicated gallstone disease in the absence of any abnormalities of the common bile duct (CBD) on abdominal US and with normal LFTs were classified as low risk and did not receive further investigations. The definition of locally complicated gallstone disease included the clinical presentation of acute cholecystitis or a mucoceole. Patients with uncomplicated or locally complicated gallstone disease with a dilated CBD of ≥8 mm on abdominal US, abnormal LFTs, or both were classified as medium risk. Patients with the presentation of clinical jaundice (bilirubin ≥35 μmol/L), cholangitis, or pancreatitis were classified as high risk and were further subdivided into the following clinical categories: (a) jaundice and/or cholangitis, (b) pancreatitis, and (c) pancreatitis and jaundice.
Prior to the introduction of MRCP in 2005, patients classified as medium or high risk underwent ERCP. From 2005, patients in the medium- or high-risk categories initially underwent an MRCP and received an ERCP if an abnormality was detected within the CBD. Patients with jaundice and evidence of cholecystolithiasis on abdominal US preceded directly to ERCP. During ERCP, endoscopic sphincterotomy was always performed if stones were detected. Patients who failed to achieve clearance of the bile duct on ERCP were referred to a tertiary center for LC and CBD exploration (CBDE) and were excluded from this series of LC.
LC
All LCs were performed by or under supervision of one consultant general surgeon (A.K.A.). Conventional four ports were used (two 10-mm ports and two 5-mm). IOC was not performed in any of the patients in this series.
Follow-up
The duration of postoperative follow-up was limited to 6 months by targets set up by the National Health Service, especially in asymptomatic patients. However, general practitioners would refer patients back to the same consultant surgeon if there were any postoperative concerns in the long term.
Statistical analysis
The sensitivity and specificity (95% confidence intervals [CI]) of a policy of selective ERCP in the preoperative detection of choledocholithiasis were calculated using MedCalc version 11.5.1 for Windows software (MedCalc Software, Mariakerke, Belgium). The policy was considered incorrect if a retained bile duct stone was detected postoperatively, and correct if the patient either did not re-present with symptoms of choledocholithiasis or was not found to have retained stones on postoperative investigations.
Results
Patients
Seven hundred seventeen patients were identified, 582 female and 135 male, with a mean (range) age of 49 (16–86) and 56 (14–83) years, respectively. Five hundred forty-nine (76.6%) were classified as low risk, 43 (6.0%) as medium risk, and 125 (17.4%) as high risk (Table 1).
Data are numbers of patients (%).
Local complications refer to those of gallstone disease such as acute cholecystitis or a mucoceole.
LFT, liver function test; US, ultrasound.
Medium risk
Sixteen of the patients identified as medium risk prior to 2005 received ERCP, which detected stones in the CBD in 6 patients. From 2005, 20 patients were investigated using MRCP, which detected an abnormality in 6 patients who then underwent ERCP that identified CBD stones in 4 patients, Mirizzi's syndrome in 1 patient, and 1 patient who did not have stones. A further 7 medium-risk patients had a normal repeat abdominal US and LFTs and did not undergo MRCP or ERCP (Fig. 1).

Results of preoperative investigations for choledocholithiasis. ERCP, endoscopic retrograde cholangiopancreatography; MRCP, magnetic resonance cholangiopancreatography.
High risk
Sixty-eight patients presented with clinical jaundice, cholangitis, or both. Of these, 36 received endoscopic sphincterotomy following the identification of stone(s) in the CBD. Forty-six presented with pancreatitis in the absence of jaundice, and of these, ERCP detected stones in 8 patients. The clinical presentation of pancreatitis and jaundice was seen in 11 patients, 3 of whom were found to have CBD stones and received endoscopic sphincterotomy and stone extraction (Fig. 2).
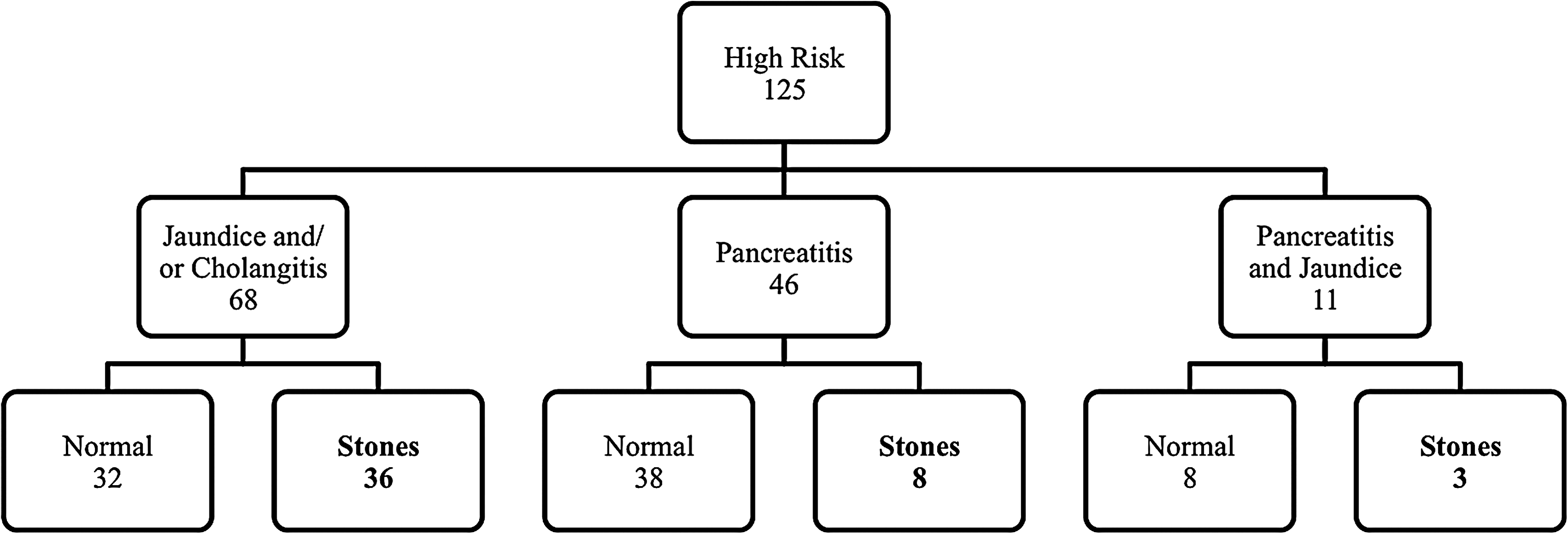
High-risk group: Subclassification and results of preoperative investigations for choledocholithiasis.
Conversion to open surgery
Laparoscopic cholecystectomy was converted to open surgery in 34 patients (4.7%) for the following reasons: anatomical scarring (n=19), gallbladder fistula to adjacent viscus (n=5), bleeding (n=3), perforation of the gallbladder with chronic abscess (n=3), tangential injury to the CBD (n=2), Mirizzi's syndrome (n=1), and gangrenous gallbladder with perforation (n=1). All converted cholecystectomies were uneventful but for 1 patient, who re-presented with delayed ischemic biliary stricture (see below).
Bile duct injuries
Tangential injury of the bile duct (Strasberg's classification, type D) 4 occurred in 3 patients (0.42%), 2 of which were due to a very short or absent cystic duct. An open T-tube was placed in both, following open conversion, and a subhepatic drain was placed laparoscopically in the third. One patient (0.14%), who was converted from laparoscopic to open cholecystectomy because of a contracted gallbladder, suffered bleeding from the porta hepatis during the open dissection that was controlled; he re-presented 7 months later with ischemic CBD stricture (Bismuth's classification, type 4) 5 and underwent reconstructive surgery successfully. In this particular patient, open IOC would not have been technically possible because of a contracted gallbladder and a very short cystic duct.
Postoperative complications
Complications were encountered in 24 patients (3.3%), and these included port site bleeding (n=10), cardiorespiratory complications (n=4), bile leak (n=6), umbilical port-wound infection (n=6), small bowel injury (n=1), paralytic ileus (n=1), and serous fluid leak (n=1). Bile leaks resolved within 3 days in 5 patients but persisted for 3 weeks in 1 patient who presented 7 months later with obstructive jaundice secondary to an ischemic stricture (see above). There were no operative (30-day or in-hospital) mortalities.
Follow-up and re-admissions
Taking into account the follow-up policy and the National Health Service targets described in Subjects and Methods, 321 patients (44.8%) attended the 6-month follow-up. Of those, only 4% complained of temporary looseness of bowel motions and dyspepsia.
Sixteen patients were re-admitted within 8 weeks postoperatively with abdominal symptoms (Fig. 3). These included abdominal pain (n=12), jaundice (n=3; all had filling defects in the bile duct on MRCP, but stones were found in 2 patients on ERCP and were extracted), and pancreatitis (n=1; MRCP revealed no stones). Of the 12 patients who presented with abdominal pain, this settled in 10 patients, whereas 2 patients had abnormalities of the CBD detected on abdominal US and MRCP and received ERCP (no stone was found in 1 patient; the other received an endoscopic sphincterotomy with stone extraction).
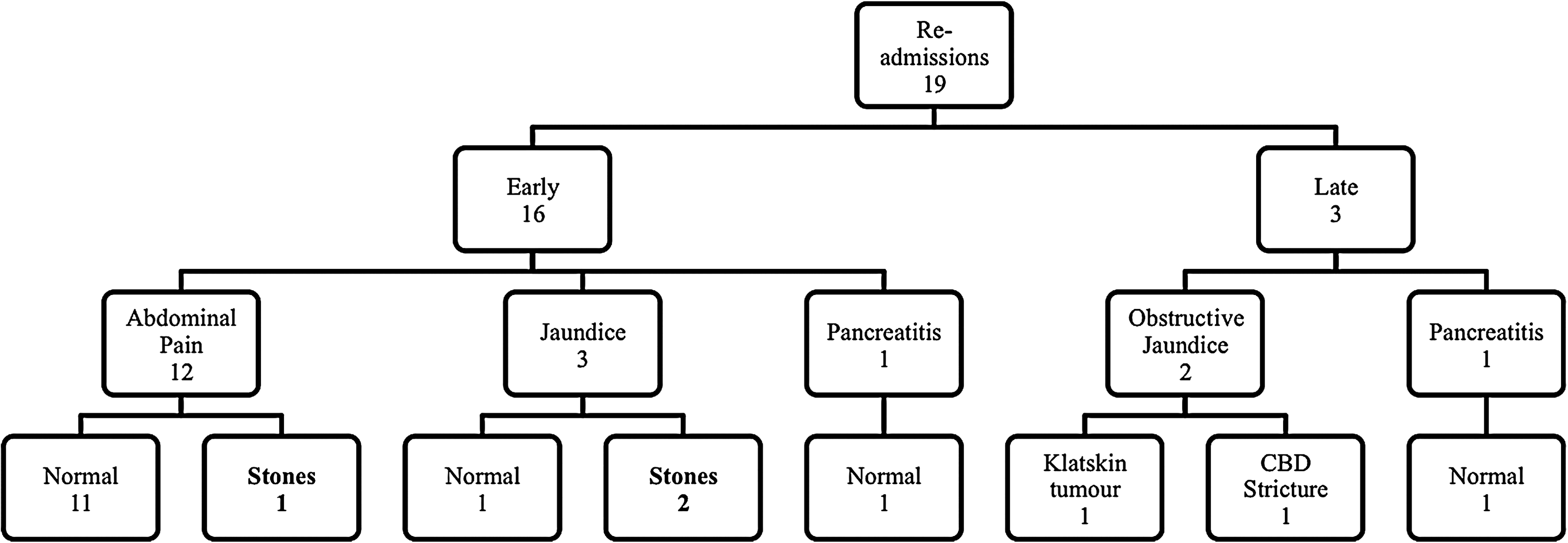
Re-admissions following laparoscopic cholecystectomy: Presentations and results of investigations. CBD, common bile duct.
Three patients were re-admitted between 8 weeks and 7 months following cholecystectomy (Fig. 3). Two patients presented with obstructive jaundice 6 and 7 months following LC: a Klatskin tumor was identified in the former and a CBD stricture in the latter. Both patients were referred to a hepatobiliary specialist unit. One patient was re-admitted with pancreatitis and received MRCP, which did not detect any abnormality within the CBD.
All patients who were re-admitted following LC had originated from the low-risk category and had not previously received MRCP or ERCP. Retained stones were detected in only 3 patients. The incidence, therefore, of retained stones among the 717 patients using the selective algorithm of preoperative MRCP and/or ERCP described above was 0.42%.
Sensitivity and specificity of selective preoperative MRCP and/or ERCP
The selective approach of preoperative MRCP and ERCP identified bile duct stones in 57 patients (incidence, 7.9%); retained stones following LC were found in 3 patients (incidence, 0.42%). Therefore, this approach demonstrated a sensitivity of 95.0% (95% CI, 86.1%–99.0%) and a specificity of 100% (95% CI, 99.4%–100.0%) in the detection of bile duct stones.
Discussion
The use of IOC during LC remains a topic of debate. The argued main benefits of this imaging modality are the identification of stones within the CBD and the delineation of the biliary anatomy, which assists in the avoidance or identification of bile duct injury. IOC is performed routinely, selectively, or not at all depending on the surgeon's practice. We have found LC without IOC performed by an experienced surgeon to be a safe operative intervention for patients with symptomatic cholelithiasis. There has been no incidence of major bile duct injury during LC, and the selective use of MRCP and ERCP has been successful in the preoperative identification and management of stones within the CBD in 99.6% of patients.
Routine IOC has had demonstrable benefits in the identification of bile duct stones with a reported sensitivity of 97.4% compared with that of 50.0% for selective IOC when retained stones detected during follow-up were considered. 1 Those who support the selective use of IOC argue that this is unnecessary in patients with normal LFTs, CBD diameter, and no history of jaundice or pancreatitis as the incidence of choledocholithiasis is extremely low. 6 In a study that applied a selective preoperative ERCP (persistently elevated LFTs) or IOC (transiently elevated LFTs and/or CBD dilatation on US), the incidence of retained bile duct stones was 0.43%. 6 We have used preoperative MRCP and/or ERCP in patients with abnormal LFTs, dilated bile ducts, or a history of jaundice, cholangitis, or pancreatitis. Our selective approach was found to be sensitive in identifying stones within the CBD in 95.0% of patients and demonstrated an incidence of retained stones of 0.42%.
The short duration of follow-up, and the 44.8% compliance rate with it, limited the validity of these calculations. The recent National Health Service targets regarding postoperative follow-up of patients halted the extension of clinical appointments beyond 6 months, particularly in asymptomatic patients. Although this may raise concerns as to the long-term results of this management protocol, it is believed that symptomatic patients would eventually present to the same site and that general practitioners would refer to the same consultant surgeon. Our patients' records would be requested if they were to present to another hospital. It is improbable that emigrants would have had a significant impact upon the results.
The detection of bile duct stones intraoperatively raises the possibility of several management options. These include laparoscopic or open CBDE, intraoperative and postoperative ERCP, and an expectant policy with follow-up MRCP in patients with small stones of 3 mm or less in diameter. 7 Laparoscopic CBDE is advantageous because of shortened hospital stay, single-stage management, and a low overall cost.8,9 However, few surgeons are able to perform this operation, and it is therefore an option unavailable to the majority of treatment centres. Conversion to open surgery for the purpose of CBDE removes the advantages of the minimally invasive approach. 7 Intraoperative ERCP creates an organizational challenge, whereas postoperative ERCP has a failure rate of 4%–10%, and therefore a second operation to explore the duct may be required. 8 Furthermore, one study revealed that one-third of patients with an abnormal IOC had a normal postoperative ERCP and suggested the use of less invasive postoperative investigations such as LFTs followed by endoscopic US or MRCP. 10
The shortcomings of intraoperative identification of bile duct stones are demonstrated by the limitations of the management options available at this stage. Therefore, the use of preoperative investigations to identify and appropriately manage those with duct stones prior to surgery is advocated. MRCP is a reliable noninvasive tool to detect bile duct calculi, but a negative test does not guarantee their absence at the time of surgery. Pierce et al. 8 compared the findings of preoperative ERCP to IOC and found 13.7% of patients had a false-negative ERCP and retained or newly passed bile duct stones. This study advocates the use of routine IOC in patients who have had stones detected within the CBD on preoperative ERCP, 8 whereas others support the use of routine IOC for those who did not receive preoperative ERCP. 11 No patients in our study who received preoperative ERCP were re-admitted because of choledocholithiasis, supporting the validity of this intervention.
The discrepancies in the different strategies used in the management of detected choledocholithiasis extend into the economic sector. One economic analysis identified single-stage LC with laparoscopic CBDE to be economically advantageous in comparison with pre- and postoperative ERCP in the treatment of choledocholithiasis. 12 Conversely, Brown et al. 13 found postoperative ERCP more cost-effective than laparoscopic CBDE.
Studies have demonstrated that routine IOC reduces the rate of bile duct injuries, assists in their early detection and immediate repair,2,14 and is therefore a more cost-effective policy than LC alone followed by expectant management in the majority of patients. 13 There have been reported cases of avoided bile duct transection by using IOC, as this can reveal the misinterpretation of the CBD as the cystic duct. 14 Therefore, injuries sustained in patients who received routine IOC were usually of a lesser severity. 2 Although routine IOC required an additional 3–6 minutes per operative case, economic advantages have been proposed because of savings in the cost of managing bile duct injuries and possible litigation.2,14 Other studies have suggested that meticulous dissection and correct anatomical interpretation can avoid bile duct injuries without the need for IOC and argue that IOC increases the cost and duration of surgery.3,6,7,15 Moreover, a recent study of 31,838 patients reported no significant difference in the incidence and detection of bile duct injury between those who did and did not receive IOC. 16 Although 3 of our patients suffered tangential bile duct injuries, we have encountered no major injury 17 that could have been avoided by IOC.
The argument that selective IOC avoids bile duct injuries is open to criticism. A recent review of the literature reported a greater incidence of bile duct injuries when selective IOC was used compared with routine IOC. 2 This is largely due to intraoperative misinterpretation of anatomical variations in patients not receiving IOC, a point that argues for routine IOC. However, the use of routine IOC does not necessarily abolish the risk of bile duct injury, as this complication might have already occurred by the time an IOC is performed. Moreover, IOC does not reveal ischemic injury to the bile duct that presents at a later date with a stricture.2,10 In addition, persistent attempts to perform IOC have been reported to inflict bile duct injury. 2
Intraoperative alternatives exist to the use of cholangiography. Laparoscopic US has proven successful in identifying bile duct stones as well as illustrating the biliary anatomy; however, interpretation of this imaging modality is more complex and requires prolonged training compared with IOC. MRCP may replace cholangiography as an intraoperative imaging modality in the future. 18
The routine omission of IOC during LC is a safe operative treatment for patients with gallstone disease provided a careful preoperative selection of patients at risk of bile duct stones for further investigations and therapeutic ERCP is adopted. The experience of the surgeon is important in the careful dissection and identification of the biliary anatomy in order to avoid injury to the main bile ducts.
Footnotes
Disclosure Statement
No competing financial interests exist.