
Abstract
Abstract
Background:
Morbidity and mortality remain relatively high for transthoracic esophagectomy with open thoracotomy. The literature is limited in describing the total combined laparoscopic and thoracoscopic Ivor Lewis esophagectomy. The aim of this study is to evaluate the outcomes of combined thoracoscopic and laparoscopic Ivor Lewis esophagectomy for the treatment of esophageal carcinoma.
Subjects and Methods:
This is a retrospective review of 15 patients diagnosed with esophageal carcinoma who underwent thoracoscopic and laparoscopic Ivor Lewis esophagectomy from August 2009 to August 2011. Eleven patients (73.3%) were diagnosed with adenocarcinoma, and 4 patients were diagnosed with squamous cell carcinoma. In total, 8 patients (53.3%) received induction chemoradiation. The mean follow-up time was 10.5±1.9 months. Postoperative morbidity and mortality were reported.
Results:
The median age was 71 years old. Fifteen patients underwent total thoracoscopic laparoscopic and Ivor Lewis esophagectomy. The operative mortality rate was 0%. The mean operative time and estimated blood loss were 468±54 minutes and 182±67 mL, respectively. The median intensive care unit days and ventilator days were 1.0 and 0.0, respectively. The median length of stay was 10 days. In total, 3 patients developed complications: One contained anastomotic leak managed with an esophageal stent, one chylous effusion managed nonoperatively, and one case of postoperative atrial fibrillation. The median number of lymph nodes dissected was 11. All of the patients had an R0 resection.
Conclusion:
Total thoracoscopic and laparoscopic Ivor Lewis esophagectomy is technically feasible, and we were able to achieve relatively good initial outcomes without major morbidity and mortality.
Introduction
Currently, there are numerous variations of laparoscopic and laparoscopic–thoracoscopic esophagectomy techniques reported in the literature. 5 Some of these techniques incorporate mini-thoracotomy and hand ports in order to conduct the operation. Limited numbers of reports have described the total thoracoscopic and laparoscopic Ivor lewis esophagectomy.6–10 In this report, I describe the outcomes of a small series of patients with esophageal carcinoma who underwent total thoracoscopic and laparoscopic Ivor Lewis esophagectomy at a single institution.
Subjects and Methods
Study design
This study is a retrospective review of 15 patients who underwent total laparoscopic and thoracoscopic esophagectomy for esophageal carcinoma on the General Thoracic Surgery Service at the Stanford Hospitals and Clinics between August 2009 and August 2011. The charts and electronic medical records of all patients identified were reviewed, and data were collected in de-identified fashion. The study was approved by the Stanford Institutional Review Board, and the requirement for informed consent was waived. All of the patients were clinically staged before the initiation of treatment with endoscopy, computed tomography scans, and clinical history and exam. Endoscopic ultrasound and positron emission tomography scans were performed in all 15 patients prior to esophagectomy.
Surgical technique
The patient is positioned on the operating room table in the supine position. A double-lumen tube, central line, arterial line, and epidural are placed by the anesthesiologist. An esophagogastroduodenoscopy is performed initially to confirm the location of the esophageal tumor. In total, five laparoscopic ports are placed for laparoscopic mobilization of the gastric conduit (Fig. 1). A 10-mm port is placed to the left of the midline approximately 4 cm above the umbilicus using the Hasson cut-down technique. Carbon dioxide insufflation is then initiated for pneumoperitoneum to a pressure of 15 mm Hg. A 10-mm 30° thoracoscope is then placed through the 10-mm port for visualization. A 12-mm port is placed to the right of the midline at the same level as the 10-mm laparoscopic port. A 5-mm port is placed at the left costal margin, the right costal margin, and the right flank area. A 5-mm laparoscopic liver retractor is used to retract the left lateral segment of the liver cephalad. The greater curvature of the stomach is mobilized by dividing the gastrocolic ligament using the LigaSure™ device (Covidien, Mansfield, MA) while avoiding injury to the right gastroepiploic artery. The short gastric vessels are then divided along the greater curvature of the stomach with the LigaSure device. The lesser omentum is then incised with the Harmonic scalpel (Ethicon Endo-Surgery, Cincinnati, OH), and the esophagus is encircled with a Penrose drain at the hiatus. A Kocherization of the duodenum is not performed routinely because the esophagogastric anastomosis can performed without tension in the upper thorax. In addition, a pyloric drainage procedure is not performed routinely. None of the patients in this series experienced delayed gastric emptying in the postoperative period. All of the patients are placed on proton pump inhibitor therapy and metoclopramide in the immediate postoperative period. The proton pump inhibitor therapy is continued after the patients are discharged home because the majority of postesophagectomy patients experience gastroesophageal reflux symptoms. A 5–6-cm gastric conduit is then formed with multiple applications of the Endo GIA™ endoscopic stapler (Covidien) along the lesser curvature (Fig. 2). The gastric conduit is then sutured to the cardia with two #0 silk sutures using the EndoStitch™ device (Covidien). A 10-French jejunostomy tube is placed over a Seldenger wire into the proximal jejunum and secured with a 2-0 silk purse string using the EndoStitch device. The jejunostomy insertion site is secured to the abdominal wall with two interrupted 2-0 silk sutures, while taking great care to avoid torsion of the small bowel.

Laparoscopic port placement for mobilization of the gastric conduit. © 2011 by medicalartstudio.com and reproduced with permission.
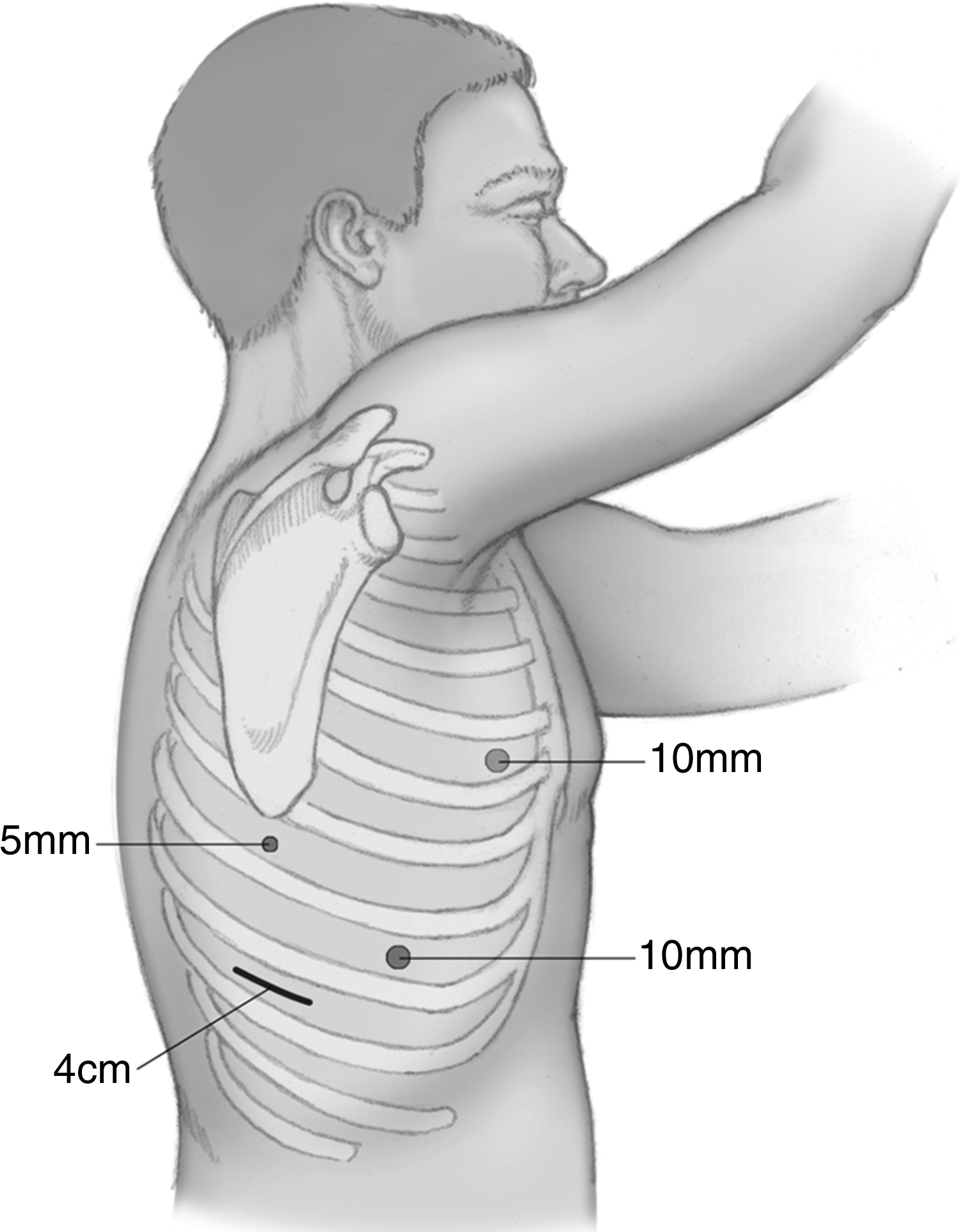
Right thoracoscopy port placement. © 2011 by medicalartstudio.com and reproduced with permission.
The thoracoscopic portion of the procedure is performed with the patient in the left lateral decubitus position with three thoracoscopy ports and a small access incision without rib-spreading (Fig. 3). A 10-mm port is placed in the 8th intercostal space posterior axillary line for the 10-mm thoracoscope. A 10-mm port is placed in the 5th intercostal space anterior line for retraction of the lung. A 3–4-cm access incision is made in the 9th intercostal space for removal of the specimen and placement of the end-to-end anastomosis circular stapler. A small Alexis wound protector (Applied Medical, Santa Margarita, CA) is placed in the access incision to prevent wound contamination when the specimen is removed. A 5-mm port is placed below the tip of the scapula. The inferior pulmonary ligament is divided with the Harmonic scalpel, and the mediastinal pleura over the esophagus is incised from the hiatus to the azygous vein. The azygous vein is dissected and divided with the Endo GIA endoscopic stapler. The esophagus and the lymphatic tissue are dissected circumferentially from the hiatus to about 2–3 cm above the azygous vein. The conduit and specimen are then pulled gently into the chest, with great care taken not to twist the gastric conduit. The proximal esophagus is divided above the azygous vein with the Endo GIA stapler. The specimen is then removed from the protected access incision, and the proximal and distal margins are evaluated with frozen sectioning. A 25-mm anvil (OrVil™, Covidien) is passed transorally, which is connected to a 90-cm polyvinyl chloride delivery tube, through a small opening in the esophageal stump staple line. The anastomosis is completed by joining the anvil with the 25-mm end-to-end anastomosis stapler (Covidien) inserted through a gastrotomy at the tip of the gastric conduit (Fig. 4). A nasogastric tube is then passed under direct vision into the gastric conduit. The gastrotomy is then resected with two or three applications of the Endo GIA stapler. The anastomosis is either covered with redundant omentum or mediastinal pleura. A 28-French chest tube and a 24-French Blake drain are placed for drainage of the chest. A barium swallow study was obtained on postoperative Day 6 to evaluate the esophagogastric anastomosis.

Laparoscopic creation of the gastric conduit. © 2011 by medicalartstudio.com and reproduced with permission.

Thoracoscopic formation of the esophagogastric anastomosis with the end-over-end anastomosis stapler. © 2011 by medicalartstudio.com and reproduced with permission.
Statistical analysis
Categorical variables were analyzed with the chi squared test, and continuous variables were analyzed with an unpaired Student's t test. The arithmetic means were reported with the standard deviation. The statistical analyses were performed using MedCalc statistical software (MedCalc Software, Mariakerke, Belgium). Differences were considered significant when the probability was less than .05.
Results
In total, 15 patients underwent total thoracoscopic and laparoscopic Ivor Lewis esophagectomy. A patient who was converted to an open Ivor Lewis esophagectomy during laparoscopy because of extensive tumor involvement of the cardia and fundus was not included in this series. A second patient who underwent a hybrid Ivor Lewis esophagectomy with laparotomy and thoracoscopy due to multiple prior abdominal surgeries was not included as well. Nine patients were male, and 6 patients were female. The median age was 71 years, and the mean age was 67.4±8.6 years. In total, 3 patients had significant chronic obstructive pulmonary disease and were active cigarette smokers. In addition, 3 patients had a history of coronary stent placement for management of coronary artery disease (Table 1). Adenocarcinoma (73.3%) was the most common histological diagnosis, and squamous cell carcinoma comprised 26.7% of the cases. Eight patients (53.3%) received induction chemoradiation prior to esophagectomy, whrtrsd 1 patient (6.7%) received induction chemotherapy alone. In total, 10 patients (66.7%) had T3 tumors on endoscopic ultrasound. The clinical staging base in endoscopic ultrasound is listed in Table 2. Nodal involvement was based on positron emission tomography, computed tomography, and endoscopic ultrasound findings of suspicious periesophageal lymphadenopathy. Fine needle aspiration was not attempted in most cases because the needle would have to be passed through large bulky tumors to reach the lymph nodes.
CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; ECOG, Eastern Cooperative Oncology Group.
The mean total operative time was 468±54 minutes, and the median total operative time was 468 minutes. The mean estimated blood loss was 182±67 mL. One patient received a transfusion intraoperatively for preoperative anemia related to induction chemotherapy. The mean number of lymph nodes dissected was 11.4±1.1 nodes. All of the patients had an R0 resection with negative proximal, distal, and radial margins on final pathology. A summary of the operative data is listed in Table 3. The overall operative mortality rate was 0%, and the overall postoperative morbidity rate was 20%. The median intensive care unit stay was 1 day, and the median ventilator days were 0. The median length of stay was 10 days. One patient developed atrial fibrillation, which was treated effectively with diltiazem prior to discharge home. One patient developed a chylous effusion that was treated nonoperatively with total parenteral nutrition and nothing by mouth for 10 days with complete resolution. This patient received 60 Gy of radiation prior to the esophagectomy procedure, which resulted in significant fibrosis around the esophagus. A patient with squamous cell carcinoma of the esophagus who had received neoadjuvant chemoradiation developed a contained anastomotic leak after having a negative barium swallow study on postoperative Day 6. An 18-×70-mm covered esophageal stent was placed, and the patient was discharged home on clear liquids. The complications are summarized in Table 4. The mean follow-up time is 10.5 months. During the study period, 2 patients (13.3%) required single balloon dilation for anastomotic stricture. All 15 patients are currently alive. Two patients developed distant recurrent disease that was treated with chemotherapy.
ICU, intensive care unit; MI, myocardial infarction.
Discussion
Since the first description of the two-stage Ivor Lewis esophagectomy in 1946, 1 the procedure has become the procedure of choice in several centers for the resection of esophageal carcinoma. The technique allows surgeons to perform an adequate mediastinal lymphadenectomy, provides excellent exposure to the intrathoracic esophagus, and allows for extensive resection of the gastric cardia for tumors extending into the proximal tumor. The main disadvantage of traditional Ivor Lewis esophagectomy is the necessity for open thoracotomy. In a randomized clinical trial comparing transthoracic and transhiatal esophagectomy, Hulscher et al. 2 demonstrated that patients undergoing esophagectomy with open thoracotomy had a significantly higher rate of pulmonary complications, which resulted in more ventilator days, intensive care unit days, and hospital days. In an attempt to minimize the perioperative morbidity associated with esophagectomy, a few centers have developed minimally invasive esophagectomy techniques for surgical resection of esophageal carcinoma. Luketich et al. 4 reported their extensive experience with the total laparoscopic and thoracoscopic three-field esophagectomy with cervical anastomosis; in this series, 222 patients with high-grade dysplasia or esophageal carcinoma underwent minimally invasive esophagectomy with relatively low operative mortality (1.4%). The median intensive care unit days were 1 day, and the median length of stay was 7 days. These results for operative mortality rate and length of stay were superior to the findings of two large contemporary series involving open transthoracic and transhiatal esophagectomy.11,12
This report describes a series of total thoracoscopic and laparoscopic Ivor Lewis esophagectomy without of the use of hand ports or mini-thoracotomy. There are currently four reports in the literature describing total minimally invasive Ivor Lewis esophagectomy (Table 5). Bizekis et al. 6 reported the results of 15 patients undergoing total laparoscopic and thoracoscopic Ivor Lewis esophagectomy without mini-thoracotomy; this cohort of patients had no postoperative pulmonary complications such as pneumonia or pulmonary embolism, and the median length of stay was 7 days. The first report describing total minimally invasive Ivor Lewis esophagectomy was by Watson et al., 7 who described 2 patients undergoing a technique consisting of hand-assisted laparoscopy and thoracoscopy; both patients had an uneventful postoperative course and were discharged home on postoperative Day 10. Nguyen et al. 9 reported a series of 46 minimally invasive esophagectomies that included a total of 3 totally minimally invasive Ivor lewis esophagectomies with 4.3% mortality rate and a median length of stay of 8 days. Kunisaki et al. 10 reported a series of 15 patients undergoing totally minimally invasive Ivor Lewis esophagectomy; in this series, the mean length of stay was 30 days, and the anastomotic leak rate was 13.3%, but there were no operative mortalities (0%).
Mini-thoracotomy used.
3 of the 46 patients underwent a total laparoscopic and thoracoscopic Ivor Lewis esophagectomy.
EBL, estimated blood loss; LOS, length of stay; OR, operating room.
In the present series of 15 patients undergoing total thoracoscopic and laparoscopic Ivor Lewis esophagectomy, the operative mortality was 0%. In this elderly population (median age, 71 years), the postoperative outcomes were relatively good with our minimally invasive Ivor Lewis approach. There were no postoperative pulmonary complications, such as pneumonia, pulmonary embolism, or respiratory failure. As a result, the median intensive care unit days and ventilator days were minimized. There were three complications, which included atrial fibrillation, a chylous effusion, and a contained anastomotic leak. The chylous effusion occurred in a patient who had received 60 Gy of preoperative radiation prior to surgical resection. The thoracoscopic mobilization of the esophagus was difficult because of fibrosis; therefore, the thoracic duct was likely injured resulting in a chylous effusion. The chylous effusion resolved in 10 days without operative intervention, and the patient was discharged home on a regular diet. The patient who developed a contained anastomotic leak was managed with an 18-×70-mm covered esophageal stent. A subsequent barium study 2 days later was negative for extravasation of contrast, and the patient was discharged home on full liquids and enteral tube feeds. This patient received preoperative chemoradiation, and she had a component of malnutrition preoperatively. The anastomosis was performed above the level of the carina, which was within the radiation field. The operation was not complicated by technical issues, tension on the anastomosis, or compromised blood supply. Thus, the presumed etiology of the anastomotic leak was the confounding preoperative risks factors listed previously.
The median length of stay for this series is 10 days, which is similar to the results of the other minimally invasive Ivor Lewis series (Table 5). The mean operative time for this series is 468 minutes, which is slightly higher than the reports by Watson et al. 7 and Nguyen et al. 9 and lower than the report by Kunisaki et al. 10 Our mean operative time was likely influenced by both the learning curve, the effects of preoperative chemoradiation, and dissection of predominately T3 bulky tumors. The mean estimated blood loss was 182 mL, and none of the cases required emergent conversion to an open incision for hemorrhage. All of the patients in our report underwent an R0 resection with negative proximal, distal, and radial margins on final pathology, and the median and mean numbers of lymph nodes dissected were 11.0 and 11.4, respectively.
In this report, I have demonstrated that totally laparoscopic and thoracoscopic Ivor Lewis esophagectomy can be performed with minimal morbidity and mortality. Overall postoperative respiratory complications such as pneumonia, acute respiratory distress syndrome, and pulmonary embolus were not encountered in the postoperative period after minimally invasive Ivor Lewis esophagectomy. The results in this report were comparable to those of other published reports describing the results of minimally invasive Ivor Lewis esophagectomy. The overall low frequency of pulmonary complications that are seen after the minimally invasive approach is likely a direct result of avoiding open thoracotomy, which has been implicated in increased rates of pulmonary complications. 2 Given the small size of this series and a relatively short follow-up period, we cannot comment on the 5-year survival rate or local–regional recurrence rates achieved with minimally invasive Ivor Lewis esophagectomy. As our experience increases with this technique, we will be able to better define the long-term benefit of total laparoscopic and thoracoscopic Ivor Lewis esophagectomy over the traditional open technique.
Footnotes
Disclosure Statement
No competing financial interests exist.