
Abstract
Abstract
Benign mucinous cystadenoma of the ovary is extremely rare in children and adolescents. Because of the benign, slow-growing nature, they can be extremely large at the point of presentation. These large abdominal tumors present a challenging opportunity for the application of minimally invasive techniques. The authors present a case of an extraordinarily large childhood mucinous cystadenoma removed laparoscopically.
Introduction
Case Report
History
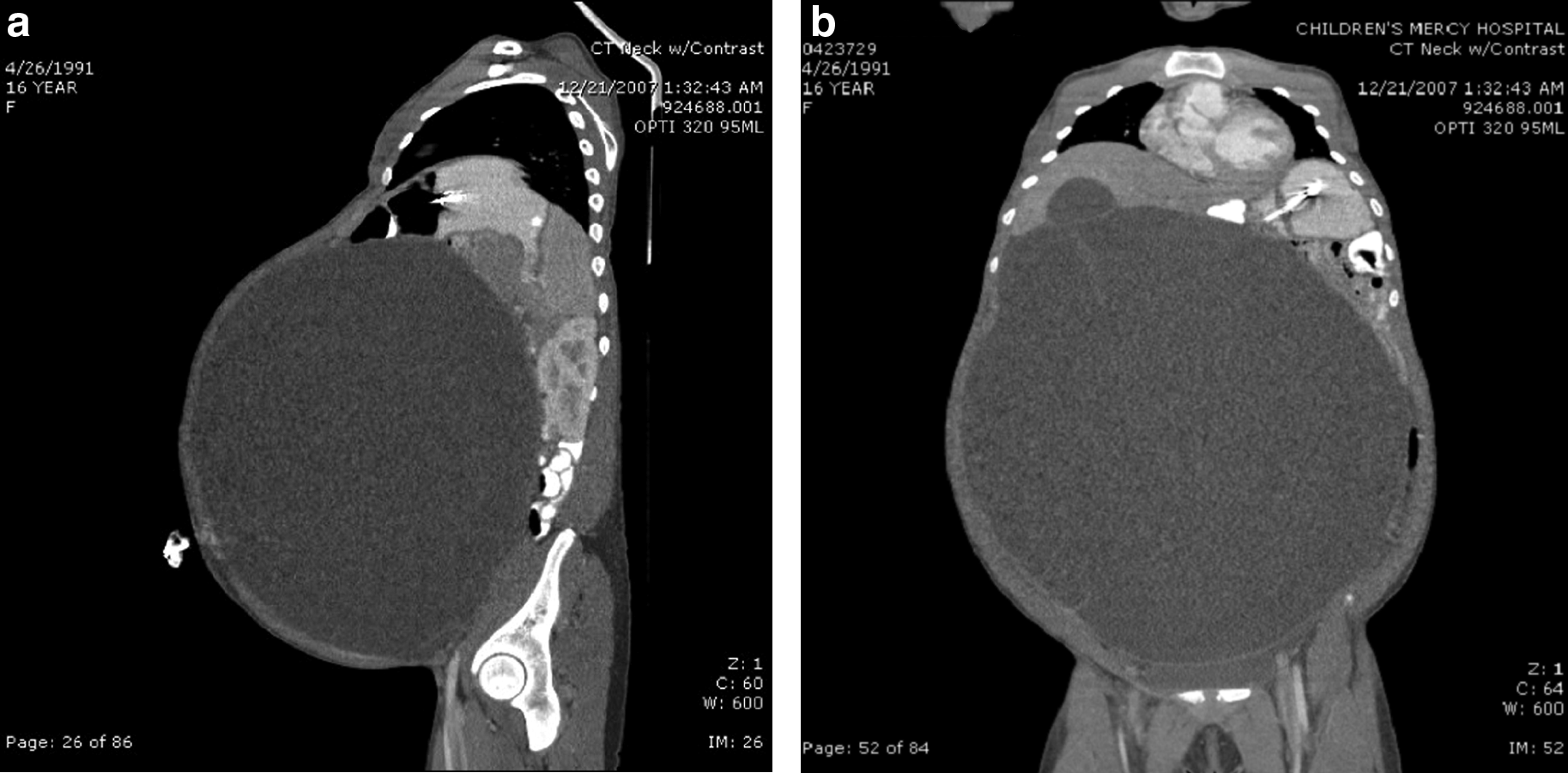
A 16-year-old previously healthy girl presented to our adolescent clinic with a 2-year history of increasing abdominal distension without pain but associated with weight loss, constipation, and occasional breathing difficulties. Her past medical history was otherwise unremarkable. Physical examination revealed a markedly distended, nontender abdomen with girth measuring 61 cm. She was admitted for further evaluation and management. A computed tomography scan of the abdomen and pelvis revealed a massive cystic abdominal mass occupying the entire abdomen and pelvis. The lesion, measuring 37 cm×31 cm×37 cm, compressed all the intraabdominal organs posteriorly and displaced both hemidiaphragms superiorly, resulting in dramatic pulmonary compression (Fig. 1). The mass had some internal septations, but no solid component, and was suspected to be of ovarian origin. There was no lymphadenopathy or evidence of metastasis. Laboratory testing revealed a mildly elevated CA 125 protein at 38 U/mL (reference range, 0–34 U/mL), whereas other markers were normal, including alpha-fetoprotein of 1.0 ng/mL, serum human chorionic gonadotrophin of <1 mIU/mL, carcinoembryonic antigen of 0.3 ng/mL, and lactate dehydrogenase of 436 U/L.
Operation
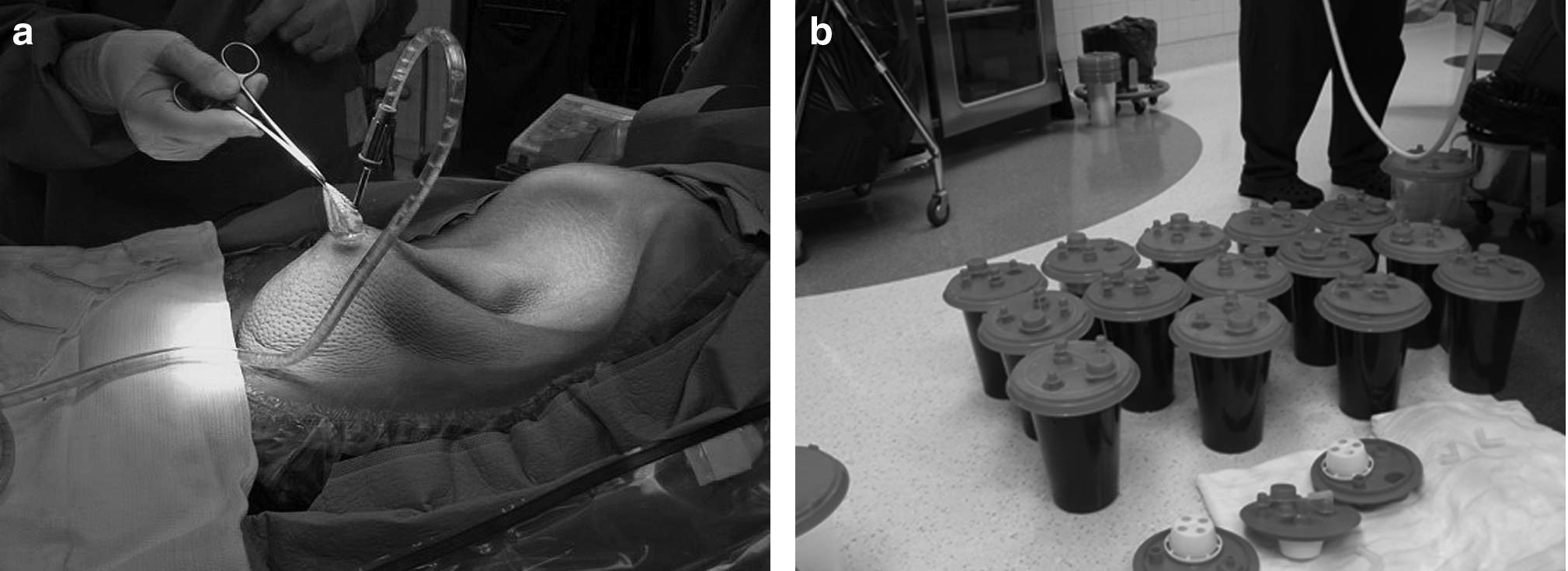
The patient was placed in a supine position (Fig. 2). A small umbilical incision was made and readily provided access to the cystic mass, which was densely adherent to the anterior abdominal wall in this area. There was no free space between the tumor wall and the peritoneum without dissection, and therefore no direct communication with the free peritoneal cavity, so we were comfortable suctioning the lesion through the umbilicus at this point. The cystic portion of the mass, visualized directly through the umbilical incision, was opened sharply, and the edges of the cyst wall were grasped with clamps. A pool-suction tip was connected to wall suction and placed directly into the cyst cavity, and over 16 L of fluid was drained to decompress the majority of the cyst (Fig. 3). The opening in the cyst was then closed with a suture, and we began a difficult blunt dissection to separate the cyst from the anterior abdominal wall. Using blunt finger dissection between the mass and the anterior abdominal wall, we were able to create enough space to introduce two 5-mm instruments through separate small incisions lateral to the umbilicus. The mass was densely adherent to the anterior and lateral abdominal wall and a portion of the liver, requiring extensive blunt and sharp dissection to mobilize the mass. The majority of this dissection was performed with blunt laparoscopic graspers to spread within the tissue plane between the cyst and the surrounding structures. Endo Shears™ (Covidien, Norwalk, CT) were used to divide some densely adherent tissue, with limited use of attached monopolar electrocautery to control small bleeding vessels. We did not use an ultrasonic or bipolar electrosurgical device to carry out this cutting and coagulating because of concerns that such a device might perforate the cyst wall. Upon visualizing the pelvis, the mass found to be originating from the right ovary. The left ovary appeared normal, and inspection of the omentum and peritoneal surfaces found no nodules and no enlarged lymph nodes. Peritoneal washings were not performed, as this would have returned a vast predominance of red blood cells. Once the mass was decompressed and mobilized, the lesion was brought out through the umbilicus, which required extending the incision slightly to eviscerate the entire cyst wall (Fig. 4). The vascular pedicle was then divided with a linear-cutting GIA™ stapler (Covidien), with care to preserve the Fallopian tube.

A massive abdominal mass is readily apparent on physical exam.

After laparoscopic mobilization, the decompressed cyst was removed through the umbilicus, and the vascular pedicle was divided with a stapler.
Postoperatively she was noted to have a hemoglobin level of 5.5 g/dL, for which she received one transfusion of packed red blood cells. This low hemoglobin was presumed to be from oozing from the abdominal wall from the large surface area of dissection. After stability was ensured and she advanced to a regular diet, she was discharged to home on postoperative day 3. On subsequent follow-up, her abdominal wall musculature regained normal tone remarkably well.
Pathologic gross examination revealed a 27-×25-×5-cm cystic mass with a wall thickness of 0.3–0.7 cm. Within the mass were complex, multiloculated, thin-walled cysts. Histologic examination found the cyst lining composed of a single layer of mucin-containing columnar or cuboidal epithelium, without cytologic atypia or nuclear stratification. The columnar epithelium was described as intestinal type, containing rare goblet cells, ciliated columnar cells, and focal hyperplastic changes with formation of papillary projections. The external surface was covered by flattened mesothelial cells. No normal ovarian tissue was identified. Immunohistochemistry found no glial fibrillary acidic protein–positive neuroglial tissue or desmin-positive muscle tissue to suggest mature teratoma. The final pathologic diagnosis was mucinous cystadenoma, intestinal type.
Discussion
The majority of childhood ovarian tumors arise from germ cells, whereas less than 20% are derived from the surface epithelium of the ovary. 2 A review of 1700 published cases of ovarian neoplasms in girls under 20 years of age reported epithelial tumors in only 19%, of which 16% were malignant. 1 The most common epithelial neoplasm in children is benign cystadenoma, of which 75% are serous and 25% are mucinous cystadenomas.1,2 Mucinous cystadenoma occurs as a large cystic mass, often multiloculated, lined by tall columnar epithelium and containing fluid rich in mucus. 3 It primarily occurs in women between age 20 and 40 years, rarely occurs in teenagers, and is exceptionally rare in premenstrual girls. 4 Malignant transformation occurs in only 5%–10%. This tumor can grow to an enormous size, sometimes occupying the entire abdominal cavity, but is usually not adherent to adjacent organs.5,6 Extremely large mucinous cystadenomas have been reported to present with renal insufficiency due to ureteral obstruction and even abdominal compartment syndrome.8,9 Conservative surgical management, consisting of unilateral salpingo-oophorectomy, is adequate treatment for benign and borderline malignant mucinous cystadenomas. 7
The use of laparoscopy to resect large ovarian lesions has been widely reported; however, the literature contains few reports describing a laparoscopic approach to massive cystic abdominal lesions.10,11 Advantages of laparoscopy in this situation are immense because an open operation would require an incision from pubic bone to xiphoid in order to complete the dissection and evisceration of the mass. Given the massive size of this tumor, such a large incision would not have obviated the need to aspirate and decompress the cyst in a controlled fashion, in order to avoid an uncontrolled free intraperitoneal rupture during mobilization. Transumbilical aspiration of the large cystic components allowed the benign tumor to decompress in a controlled manner with minimal contamination and subsequently deliver out through a small incision. Laparoscopy was then used to dissect the tumor free from the abdominal wall and liver, to which it had become chronically adherent. Some authors have advocated using two adhesives and a sterile plastic bag to aspirate large ovarian cysts through the bag and prevent peritoneal contamination with cystic fluid when a malignant tumor is suspected. 12 In this case, the peritoneum around the umbilicus was densely adherent to the mass, with no free peritoneal space, so it was deemed safe to suction the fluid without this adjunct, as it would add little to the anatomic situation. Furthermore, this history demonstrated a very low likelihood of malignancy. Benign mucinous cystadenoma was the strongly suspected diagnosis, due to the chronic, indolent course, the extremely large size at presentation with entirely cystic components, no metastases or lymphadenopathy, and normal serum markers. It is important that, if an ovarian mass has any features suggesting malignancy, peritoneal contamination must be meticulously avoided, which may require an open approach. Appropriate staging procedures for malignancy include aspiration of ascites and/or peritoneal washings, inspection of peritoneal surfaces, the omentum, the contralateral ovary, and retroperitoneal lymph nodes, and biopsy of any suspicious lesions. Additionally, the surgeon should be prepared to complete a full cytoreduction and staging operation, as well as involve a gynecologic oncologist in a case of this nature.
Benign ovarian mucinous cystadenomas are rare and often present as extremely large cystic tumors, as exemplified in this case, but the massive size does not preclude the use of minimally invasive techniques for resection. Such an approach can be performed and avoid an extensive laparotomy incision.
Footnotes
Disclosure Statement
No competing financial interests exist.