
Abstract
Abstract
Background:
The study was conducted to assess the patient acceptability of non-sedated upper gastrointestinal (GI) endoscopy and to study cardiorespiratory changes during the procedure.
Subjects and Methods:
This study was conducted in the outpatient endoscopy room of Department of Surgery of a teaching tertiary-care hospital in North India. The patients underwent diagnostic GI endoscopy under topical pharyngeal anesthesia using 5% lidocaine. No sedation was used. Pulse rate (PR), respiratory rate (RR), oxygen saturation (SpO2), and mean blood pressure (BP) were recorded immediately prior to endoscopy, during endoscopy, and 5, 15, and 30 minutes after endoscopy. Using a 10-point Likert scale, all the patients were asked to record their expected discomfort for the endoscopy as a pre-test score and their actual level of discomfort during endoscopy as a post-test score. Patients were also asked about whether they would opt for non-sedated upper GI endoscopy again in the future if required.
Results:
Sixty patients underwent diagnostic upper GI endoscopy during the study period. Post hoc tests using Bonferroni's correction revealed that mean PR, RR, and mean BP changed significantly during endoscopy. However, these parameters normalized at 30 minutes following endoscopy. Mean SpO2 did not differ significantly at the different time points. Pre- and post-endoscopy mean visual analog scale scores to assess the expected level of discomfort during endoscopy were not statistically different. Forty-four patients (73.3%) indicated their willingness to undergo repeat non-sedated endoscopy in the future if required. Binary logistic regression analysis identified young age, male gender, and long duration of procedure as significant factors for unwillingness to undergo repeat non-sedated endoscopy.
Conclusion:
Non-sedated endoscopy is a feasible, safe, and fast office procedure and seems well tolerated by most patients.
Introduction
The advantages of non-sedated upper GI endoscopy are multifold. Intensive monitoring of patients is not required, and so costly equipment, the recovery room, and skilled manpower are not needed. There are no sedation-related complications. Moreover, the patient remains conscious and can follow the examination from the monitor. Patients can also cooperate in changing position during non-sedated endoscopy. The patient may come for non-sedated endoscopy unescorted and can also resume his or her work the very same day. These advantages of non-sedated upper GI endoscopy make it a practical option in resource-scarce developing countries, provided patients tolerate and accept non-sedated upper GI endoscopy reasonably. This is also of utmost importance so that non-sedated endoscopy should not prove to be a barrier for patient compliance in a repeat procedure if required.
The present prospective observational study was conducted to assess acceptability of non-sedated upper GI endoscopy and to assess cardiorespiratory changes in patients undergoing non-sedated upper GI endoscopy.
Subjects and Methods
Study design and setting
This was a prospective observational study performed in the outpatient endoscopy room of the Department of Surgery of a tertiary-care hospital in North India where more than 1000 upper GI endoscopy procedures are done annually. The study interval was May 1, 2011–August 31, 2011.
Study population
Sixty patients underwent diagnostic upper GI endoscopy during the study period in a single surgery unit. Exclusion criteria were as follows: (1) age less than 18 years; (2) hemodynamically unstable patients; (3) patients having active coronary ischemia, respiratory distress, and baseline oxygen saturation (SpO2) of less than 95% and requiring oxygen therapy before the procedure; (4) previous experience of upper GI endoscopy; (5) known allergy to lidocaine; (6) patient not giving consent to participate in the study; and (7) uncooperative patients.
Methodology
The procedure, associated discomfort, and advantages and disadvantages of non-sedated upper GI endoscopy were explained in detail to all patients fulfilling the inclusion criteria. An informed consent was taken from the patients for participating in the study. Approval was obtained from the Institutional Ethics Committee to conduct the study.
Upper GI endoscopy was performed using an esophagogastroduodenoscope (model EG-250WR5, Fujinon Singapore PTE Ltd.). Topical anesthesia was induced in the pharynx by spraying a solution of 5% lidocaine until the gag reflex was abolished. No sedation was used. A nurse and an attendant were present during the procedure to assist in biopsies and oral suction, if required. The endoscope was inserted through the oral cavity and the upper esophageal sphincter under direct vision. The esophagus, stomach, and duodenum down to the second part were examined as usual. Biopsies were performed when indicated.
Data collection procedures
The sociodemographic profiles of all patients were recorded. Indications for the upper GI endoscopy and endoscopy findings were noted.
Indicators of cardiorespiratory changes
Pulse rate (PR), respiratory rate (RR), SpO2, and mean blood pressure (BP) were recorded immediately prior to endoscopy, during endoscopy, and 5, 15, and 30 minutes after endoscopy.
Indicator of patient's acceptance of the procedure
Using a 10-point Likert scale, all the patients were asked to record their expected discomfort for the test as a pre-test score. After completion of the test, all the patients were again asked to record their actual level of discomfort experienced during non-sedated endoscopy as a post-test score. The discomfort was assessed by scores between 0 and 10, with 10 being the most severe degree of discomfort and 0 being no discomfort. Patients were asked about whether they would opt for non-sedated upper GI endoscopy again in the future if required.
Statistical analysis
Statistical analysis was done using SPSS version 10 software. The data are summarized as mean±standard deviation values. Repeated-measure analysis of variance (ANOVA) was used to compare PR, RR, mean BP, and SpO2 at different points in time. Pre- and post-endoscopy visual analog scale (VAS) scores for level of discomfort are presented as mean±standard deviation values (95% confidence interval), and the mean difference was tested for statistical significance using the paired t test. Binary logistic regression analysis was done to identify factors to predict willingness to undergo repeat endoscopy in the future. A P value of <.05 is taken as significant.
Results
There were 60 patients who underwent diagnostic upper GI endoscopy during the study period. Mean age of the patients was 42.50±15.39 years. There were 32 male and 28 female patients in the study group (male:female ratio 8:7). Table 1 describes the various indications for which upper GI endoscopy was undertaken in the study group. The examination was completed to the second part of duodenum in all 60 patients. The average examination time was 6.23±2.71 minutes. Table 2 describes the various endoscopic findings seen in the study group. No abnormality was observed in 26.6% (n=16) patients.
Repeated-measures ANOVA with a Greenhouse–Geisser correction determined that mean PR differed statistically significantly between different time points (F=35.028, P=.00). Post hoc tests using Bonferroni's correction revealed that mean PR increased during endoscopy (109.66±22.44 beats per minute, 95% confidence interval [CI] 103.87–115.46) compared with before endoscopy (92.23±19.62 beats per minute, 95% CI 87.16–97.30), which was statistically significant (mean difference=17.43 beats per minute, 95% CI 10.26–24.60, P=.00). However, mean PR at 30 minutes post-endoscopy decreased to 92.93±18.10 beats per minute (95% CI 88.25–97.61), which was statistically not different from the pre-endoscopy mean PR (mean difference −0.70±14.55, 95% CI −3.05 – 4.45, P=.71).
A repeated-measures ANOVA with a Greenhouse–Geisser correction determined that mean BP differed statistically significantly between different time points (F=13.36, P=.000). Post hoc tests using Bonferroni's correction revealed that mean BP increased during endoscopy (97.53±15.66 mm Hg, 95% CI 93.49–101.58) compared with pre-endoscopy (90.81±14.05 mm Hg, 95% CI 87.18–94.44), which was statistically significant (mean difference 6.72, 95% CI 2.30–11.13, P=.00). However, mean BP rate at 30 minutes post-endoscopy decreased to 90.28±12.17 mm Hg (95% CI 87.13–93.42), which was statistically not different from the pre-endoscopy mean BP (mean difference −0.53±8.75, 95% CI −2.79 to 1.72, P=.63).
Repeated-measures ANOVA with a Greenhouse–Geisser correction determined that mean RR differed statistically significantly between different time points (F=73.58, P=.00). Post hoc tests using Bonferroni's correction revealed that mean RR decreased during endoscopy (14.42±3.76 breaths per minute, 95% CI 13.44–15.38) compared with before endoscopy (17.60±3.63 breaths per minute, 95% CI 16.66–18.54), which was statistically significant (mean difference 3.18, 95% CI 2.06–4.30, P=.00). However, mean RR at 30 minutes post-endoscopy increased to 17.13±3.77 breaths per minute (95% CI 16.15–18.10), which was statistically not different from the pre-endoscopy mean PR (mean difference −0.46, 95% CI −1.11 to 0.18, P=.15).
Repeated-measures ANOVA with a Greenhouse–Geisser correction determined that mean SpO2 did not differ significantly at different time points (F=2.38, P=.09). In view of the insignificant change in SpO2 at different time points, further post hoc tests using Bonferroni's correction were not undertaken.
Figure 1 shows various changes PR, RR, mean BP, and SpO2 during endoscopy.
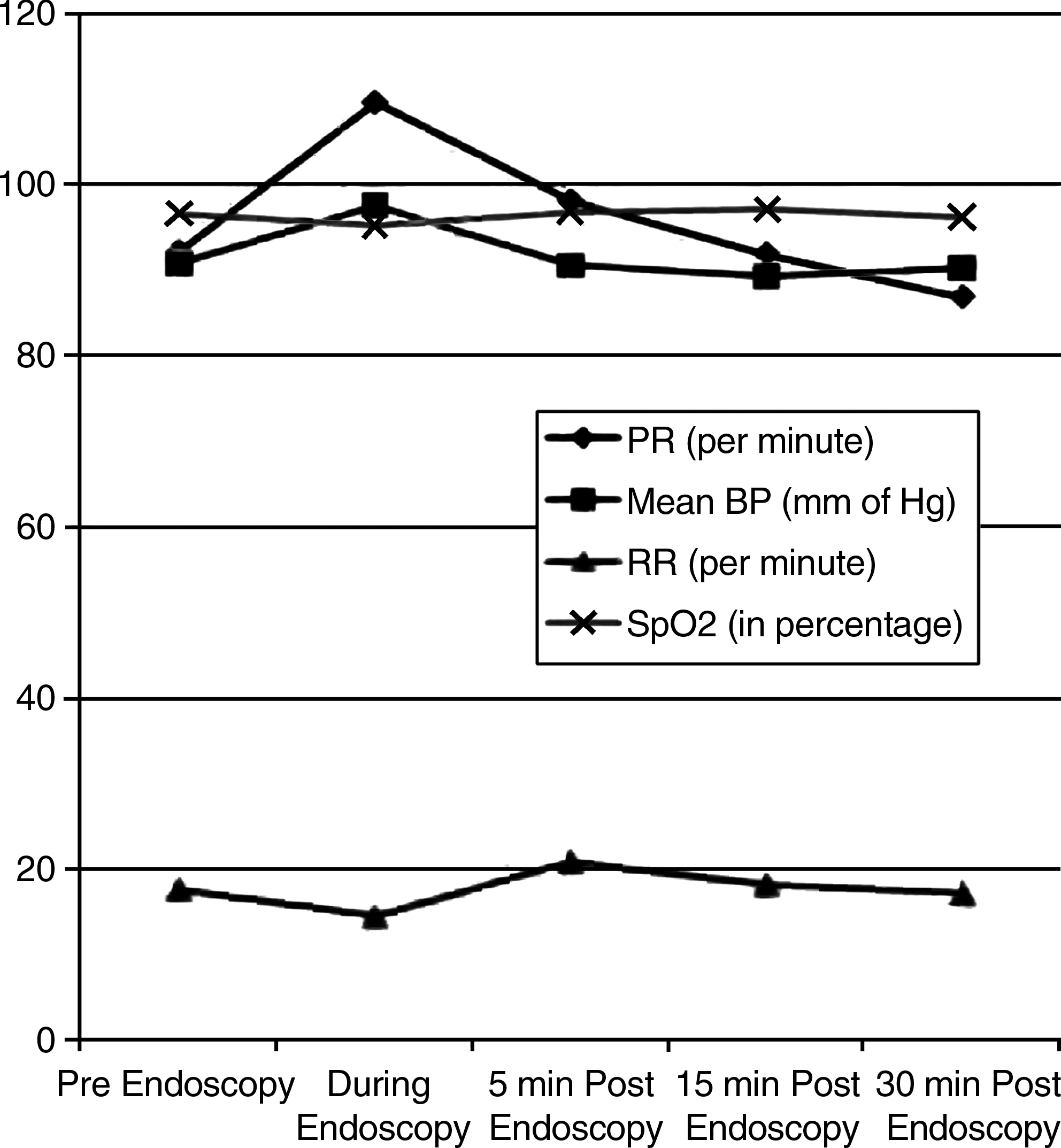
Changes in pulse rate (PR), respiratory rate (RR), mean blood pressure (BP), and oxygen saturation (SpO2) during endoscopy.
Pre-endoscopy mean VAS score to assess the expected level of discomfort during endoscopy was 3.93±2.36 (95% CI 3.32–4.54). Post-endoscopy mean VAS score to assess the actual level of discomfort during endoscopy was 4.73±2.69 (95% CI 4.04–5.43), which was not statistically different from pre-endoscopy mean VAS score (mean difference 0.80, 95% CI −0.01 to 1.61, P=.05).
Forty-four patients (73.3%) showed their willingness to undergo repeat non-sedated endoscopy in the future if required. Binary logistic regression analysis to predict factors for unwillingness to undergo repeat non-sedated endoscopy identified young age (P=.018), male gender (P=.010), and prolonged duration of procedure (P=.009) as significant factors. Pre-endoscopy VAS score was not significantly related (P=.187) to willingness to undergo repeat non-sedated endoscopy.
Discussion
There are numerous published studies evaluating factors affecting patients' tolerance for non-sedated routine diagnostic upper GI endoscopy and others comparing patients' preference for sedated versus non-sedated endoscopy or comparing medications used for conscious sedation. There are many reasons why some patients prefer to undergo upper GI endoscopy without sedation. It is devoid of any significant cardiorespiratory compromise. Although our study documented a significant change in PR, RR and mean BP, these changes return to normal within 15–30 minutes of completion of the procedure. Moreover, there was no significant change in SpO2 during endoscopy. This suggests that long-duration monitoring of patients is not required following non-sedated endoscopy. This translates into several advantages. First, patients will not be required to be kept in endoscopy suites for long for post-endoscopy monitoring. This will also avoid the cost associated with employment of skilled manpower and sophisticated and expensive monitoring gadgets. The number of endoscopies per day may be increased to a large extent. Patients can go back to their work following the procedure, thus making it an “office procedure.” Patients may not require being escorted by their relatives for the procedure. These are advantages associated with non-sedated endoscopy in developing countries where there is a dearth of health resources. There is a long waiting time for upper GI endoscopy in developing countries in view of the large number of patients and few endoscopists. Moreover, most of the patients are poor, and they work for daily wages. Being an office procedure and allowing immediate return to work, non-sedated endoscopy proves especially useful for these patients. This is particularly useful as patients need not be escorted by their relatives as they themselves may also be working on daily wages, and it may not be feasible for them to get time off from their work. Aljebreen 5 stated that, in his experience, the most common reasons for patients opting for gastroscopy not under sedation are the lack of requirement for an escort, the fear of the usual sedation-related complications, and restrictions on activities for almost one full day; there is another group of patients who want to know the result of their upper GI endoscopy on the spot and who do not want to feel anxious waiting for their next visit.
In today's world, the patient's wishes are of paramount importance and cannot be ignored, especially in the context of informed consent and clinical governance. So, we also asked the patients who underwent non-sedated upper GI endoscopy whether they would be willing to undergo the same process in the future if required. There were 44 (73.3%) patients who indicated their willingness. Young age, male gender, and long duration of procedure were significantly associated with unwillingness of the patients to undergo non-sedated upper GI endoscopy in the future, whereas pre-endoscopy expected level of discomfort as determined by VAS score was not significantly associated. Campo et al. 6 also identified first-time endoscopy, young age, female gender, and high level of pretext anxiety as being significantly associated with poor patient tolerance of non-sedated endoscopy. Thanvi et al. 7 showed that acceptability to the patient of non-sedated endoscopy was no different between old and young patients.
Both sedated and non-sedated upper GI endoscopies have their own pros and cons. Patients should be informed about not only the benefits but also the drawbacks of sedation. They should also be informed that non-sedated endoscopy is a feasible, safe, and fast office procedure and seems well tolerated by most patients. This information will help them make a balanced decision.
Footnotes
Acknowledgments
This study was conducted as a part of a short-term Studentship 2011 project by the Indian Council of Medical Research awarded to Abhishek Pratap Singh (Student) and Pankaj Kumar Garg (Supervisor).
Disclosure Statement
No competing financial interests exist.