
Abstract
Abstract
Objective:
Several minimally invasive techniques using natural orifices as an entrance site to the peritoneal cavity have been described recently. Pure natural orifice translumenal endoscopic surgery (NOTES) techniques have been mainly implemented to perform cholecystectomies and appendectomies, while more complex operations like colon resections have been described in a hybrid setting and with the use of the transumbilical approach. Here we describe the technique of transvaginal sigmoid colon resection for cancer with standard laparoscopy equipment.
Materials and Methods:
After developing the transvaginal technique of sigmoid colon resection in an experimental sheep model, we have performed this operation in a human patient for cancer. Twelve months of follow-up is reported.
Results:
A totally transvaginal R0 resection of the sigmoid colon for adenocarcinoma has been successfully performed in a female patient with laparoscopy equipment. The specimen included 13 lymph nodes, all of which were free of metastasis. Twelve months after surgery the patient is alive with no evidence of disease.
Conclusion:
A pure transvaginal NOTES approach to sigmoid colon cancer is feasible in human patients.
Introduction
Laparoscopic colon resections proved to be effective and safe. 1 A less invasive approach, namely, minilaparoscopic-assisted natural orifice surgery (MANOS), a hybrid technique that uses laparoscopic transabdominal ports and a transvaginal port, allowed further minimization of operative injury, eliminating the need for abdominal incision for specimen extraction 2 and further diminishing the levels of postoperative pain. 3
A further step towards minimizing surgical stress was the development of single-incision and pure NOTES approaches. Colon resection with the single-incision umbilical approach has been described recently. 4 As for NOTES colon resection, it has been proven to be feasible in animal models through the transgastric 5 as well as the transvaginal 6 route.
Materials and Methods
We have developed a technique for sigmoid colon resection using transvaginal access route in an experimental animal (sheep) model. After safely performing two resections in sheep we have decided to introduce this technique in a human patient. The technique has been approved by the ethics committee of the Consorcio Sanitario Publico del Aljarafe, Hospital San Juan de Dios, Bormujos, Sevilla, Spain. The patient was informed about the experimental nature of the technique and gave her informed, written consent.
The procedure was designed to use the vaginal port for the camera as well as for the surgical instruments and specimen extraction. Nonetheless, we have also used a 5-mm transumbilical laparoscope as an additional safety measure.
The patient was an 83-year-old woman with sigmoid colon adenocarcinoma localized 23 cm from the anal verge and preoperatively staged as a cT2N0M0 tumor. The patient had no other co-morbidities.
Technique description
The surgical technique can be divided into the following phases:
1. Transvaginal introduction of the TriPort™ device (Advanced Surgical Concepts, Bray, County Wickow, Ireland) 2. Positioning of the colon 3. Division of the vascular pedicle and localization of the ureter 4. Division and extraction of the specimen 5. Anastomosis
1. Introduction of the TriPort device
The patient is placed in the lithotomy position. The surgeon and first assistant stand between the patient's legs, whereas the second assistant alternates between this position and the right-hand side of the patient in order to control the umbilical laparoscope.
A 5-mm umbilical trocar is placed with the open technique, and pneumoperitoneum is reached. The procedure starts with a 1.5-cm colpotomy in the posterior part of the vaginal roof with the help of a colposcope. Through this incision the TriPort device is introduced, the intra-abdominal ring is placed, and the device is locked/sutured to the external genitals in order to minimize air leaks (Fig. 1).

Placement of the TriPort device.
2. Positioning of the colon
With two atraumatic articulated graspers introduced through the vaginal port, the small bowel loops are placed in the upper part of the abdomen; this maneuver helps expose the sigmoid colon and its mesocolon.
If we retract the sigmoid colon toward the roof of the peritoneal cavity, the inferior mesenteric artery runs perpendicular to the axis of the abdominal aorta. Thus, if we place a laparoscope in the pelvis through the TriPort inferior vaginal port, we have a vertical view of the left mesocolon, which does not allow a frontal view.
That is the reason why the following step is to place the left mesocolon vertically so that we have a frontal view. This is why we use the lateral to medial approach focusing on Toldt's fascia and the peritoneum of the minor pelvis on its left side.
This maneuver is performed by tightening the sigma with atraumatic articulated graspers, which are introduced by the TriPort port on the surgeon's right-hand side, that is to say, cross-tightening using the Harmonic® scalpel (Ethicon Endosurgery) manipulated from the Triport left port in order to open Toldt's fascia. After that, we introduce the Endograb™ (Virtual Ports, Ltd., Misgav, Israel) retractor through the TriPort right port; with the atraumatic articulated graspers of the left port we suspend the mesocolon as near the mesenteric border of the sigmoid colon as possible in order to apply the Endograb attacher. Once the most proximal part of the mesocolon is attached, we anchor it to the roof of the peritoneal cavity with the Endograb applied to the most distal part of the mesocolon (Fig. 2). In this way we attach the sigmoid colon to the parietal peritoneum, thus allowing a frontal view of the mesocolon.

Endograb applied to the most distal part of the mesocolon.
3. Division of the vascular pedicle and localization of the ureter
The dissection starts by opening the peritoneum over the sacral promontory and ascending until the localization of the vascular axis of the sigmoid colon at the point where the artery starts from the abdominal aorta. The view from the pelvis is very good because the vascular axis is just in front of the laparoscope introduced transvaginally.
The dissection of the mesocolon is continued from the mesenteric axis toward the pelvis. In order to do this, we pass the right-hand articulated grasper just under the exit of the axis of the mesentery until it appears on the opposite side. With a nonarticulated dissector we separate the mesocolon off the lax adhesions.
Before dissection of the inferior mesenteric artery, the left ureter is localized as in the conventional laparoscopic technique.
At this point, the use of an articulated laparoscope that allows 90° vision becomes necessary. We have used the EndoEYE™ video laparoscope (Olympus).
Once the ureter is localized, we proceed to divide the vascular pedicle. The vascular elements can be divided with the help of metallic clips, absorbable clips, endosuturing devices, or vascular cutting and sealing systems such as LigaSure™ (Covidien) or a Harmonic scalpel. We have decided to use double metallic clips to divide the mesenteric vein and a 45-mm cartridge endostapler (model TSW 45; Ethicon Endosurgery), to divide the inferior mesenteric artery. The division is easy as the vascular elements are in front of the laparoscope.
4. Division and extraction of the specimen
Before dividing the surgical specimen, we have to divide the distal mesocolon in order to allow the endocutter to enter without any difficulty.
This maneuver is performed with the 5-mm LigaSure Advance™ vascular sealer: the sealer will be controlled from the TriPort, while traction is applied by passing articulated graspers under the mesocolon from the surgeon's right-hand side.
Then the model TSW 45 45-mm cartridge endostapler is introduced through the TriPort's left working port. The sigmoid colon stays perpendicular at the entering of the stapler, and it is easily divided with just one stapler load.
After dividing the specimen, we check that the proximal end of the colon can descend down to the vagina without difficulty. It is important that the patient have sufficient colon length that does not require liberating splenic flexure as it would be extremely difficult to achieve with transvaginal approach.
Having observed the absence of tension, we take the distal end of the sigmoid colon with a straight-handle grasper so that the distal end is guided. We withdraw the TriPort device after extracting the pneumoperitoneum, and we substitute a Vi-Drape® isolation bag (Medical Concepts Development) for it, which we place by passing it through the straight handle of the grasper. We do not need a colposcope to introduce the device.
5. Anastomosis
After exteriorizing the sigmoid colon through the vagina, we proceed to the proximal section and the introduction of the anvil of the circular CEEA™ stapler (Covidien) (Fig. 3). This technique has been successfully applied in hybrid (e.g., MANOS) approaches.
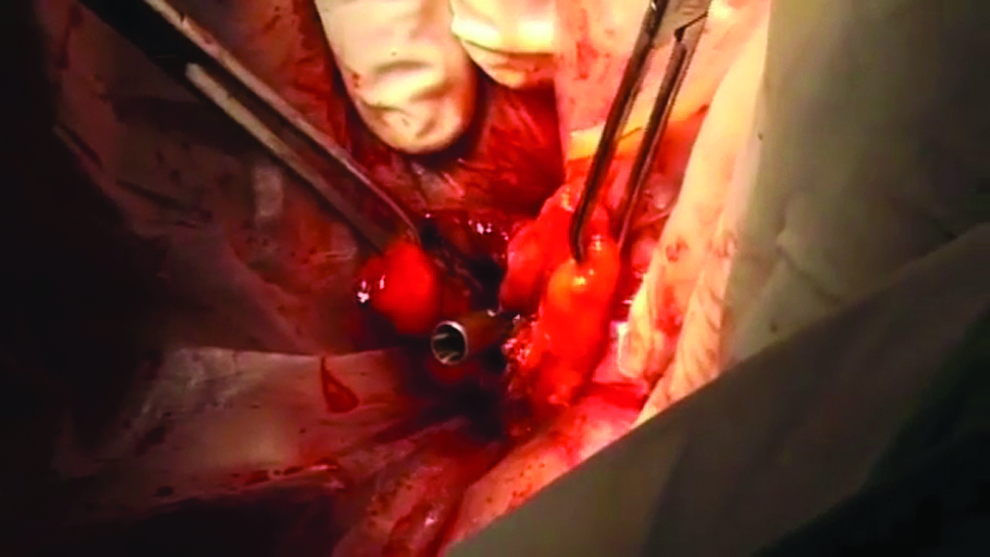
Introduction of the anvil of the circular CEEA stapler after the sigmoid colon is exteriorized through the vagina.
We re-introduce the colon in the abdominal cavity through the vagina and insert the TriPort device again.
We introduce the CEEA through the anus until the distal portion of the colon is seen in front of the tranvaginal laparoscope. We proceed to exteriorize the cutting tip of the transanally placed CEEA, introducing it in the anvil, which is already inserted in the proximal end of the colon to be anastomosized.
To perform the anchoring of the two CEEA pieces, we introduce a Diamond Flex™ semicircular retractor (Surgical Innovations Group) through one of the TriPort port. When the retractor in the peritoneal cavity, we articulate it until we get a rigid semicircle. This semicircle is applied behind the head of the anvil introduced in the proximal end of the colon. We apply a traction of the Diamond Flex until we hear the anchoring click and get the image of a perfect union of the two CEEA pieces (Fig. 4). Then we proceed to perform the anastomosis with the circular stapler.
Application of the Diamond Flex to connect the two CEEA pieces.
We extract the TriPort and suture the vagina partially with the help of a colposcope, with the purpose of the closure being essentially hemostatic.
Results
The patient began oral fluid intake in the night of the procedure. The analgesia was achieved with intravenous paracetamol during the first 48 hours and then oral paracetamol. The pain scores, evaluated every 8 hours by Visual Analog Scale (from 0=no pain to 10=unbearable pain), were below 3. Walking was started after 24 hours, and a solid diet was tolerated 48 hours after surgery. The patient was discharged home on postoperative Day 4. Twelve months after surgery the patient is alive and well with no evidence of disease.
The pathology report showed a 35-cm-long colon specimen, with adenocarcinoma infiltrating the muscularis propria, free margins, and 13 lymph nodes with no metastatic spread, which according to the seventh revision of the American Joint Committee on Cancer/TNM staging system is pT2N0M0 Stage I disease. 7
Discussion
Minimally invasive surgical approaches to the peritoneal cavity have gained important attention in recent years. The NOTES techniques, using natural body orifices as an entrance site, have been used to perform cholecystectomies 8 and appendectomies. 9 The best minimally invasive or possibly NOTES approach to colon resection is still a matter of debate. Several investigators have described transanal, 10 trangastric, 11 and transvaginal 6 approaches to colon and sigmoid resections. Those approaches, however, were until now tested only in experimental animal in vivo and ex vivo models. Another minimally invasive approach to the colon, the single-incision transumbilical approach, has been, on the other hand, shown to be feasible in human patients.12,13 At the same time, the use of the transvaginal approach to colon resections in human patients was until very recently limited to a hybrid technique with the use of additional transabdominal laparoscopic ports. This hybrid approach has been coined the MANOS technique. 2
After our initial experience with the hybrid MANOS technique 3 we have developed a technique allowing for relatively safe totally transvaginally resection of the sigmoid colon. The technique has been successfully implemented in an experimental in vivo sheep model. 6 The present report describes our initial experience with the application of the technique in a human patient with 12 months of follow-up.
The potential advantages of the transvaginal approach to colon cancer include no visible scar, faster recovery, and low levels of postoperative pain. Low levels of pain have been shown for sigmoid resections in series of the MANOS hybrid technique.2,3 On the other hand, the potential for complications arising from incision of the vaginal roof is frequently raised. 4 The current experience with transvaginal approaches does not support this concern, as in the published transvaginal MANOS series there were no complications of this kind reported.2,3 Another disadvantage of the transvaginal access route is the fact that it is technically demanding for the surgeon. This is caused by the operative field view distinct from the classic laparoscopy view 14 and by the low possibility of triangulation of the instruments and absence of the off-axis vision. 12 The several instruments are also distinct from the classic laparoscopy instruments and are more technically advanced. However, some investigators are evaluating the use of classic laparoscopy instruments for pure transvaginal NOTES in the cholecystectomy setting. 15
One of the concerns of the transumbilical single-incision approach is the potential for developing an incisional hernia. 14 This risk is absent in the transvaginal approach.
The technique presented in this report is quite technically demanding. The atypical intraoperative view offered by the transvaginal laparoscope and lack of off-axis vision makes this technique complicated even for an experienced laparoscopic surgeon. It seems necessary to start the learning curve of this technique either with animal models or possibly with simulators.
Logically, one of the main questions to be answered is the oncological safety of the technique presented. While it was possible to reach R0 resection and adequate lymphadenectomy in our case, it is crucial to carefully choose patients for future intervention of this type in order to make sure that the approach itself is not compromising oncological outcome. The strict follow-up of each patient is obligatory.
Conclusion
Totally transvaginal R0 resection for sigmoid colon cancer with adequate lymphadenectomy is feasible in human patients.
Footnotes
Disclosure Statement
A.L.K. reports receiving congress attendance, travel, and course fees from Karl Storz Germany and Ethicon Spain. For the remaining authors no competing financial interests were declared.